

The Future of Periodontology
Even with the exciting advances seen in today’s periodontal treatment, more promising therapies loom on the horizon.
Even with the exciting advances seen in today’s periodontal treatment, more promising therapies loom on the horizon
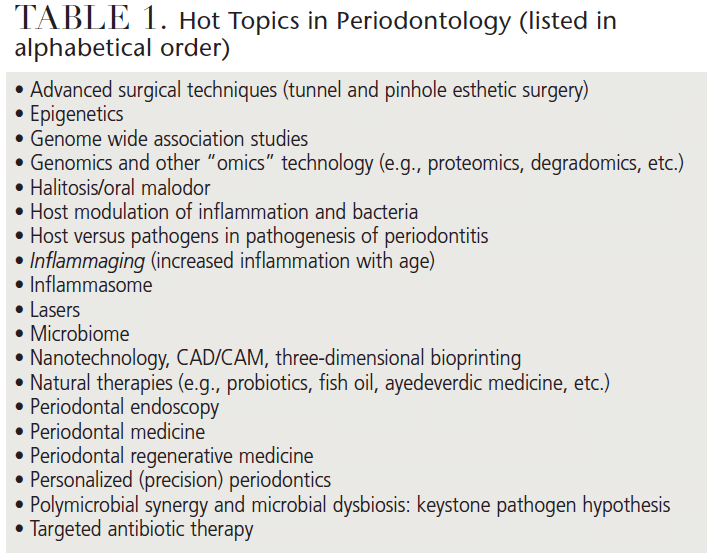
Over the decades, oral health care has seen many advances that have significantly impacted the practice of periodontics. One of periodontology’s greatest strengths is that it is not a static field; rather, it continues to evolve and readjust its focus on the basis of contemporary research spanning a vast array of scientific endeavor. A tantalizing list of topics that are currently under investigation is shown in Table 1 (page 18). Due to space limitations, this review will discuss some, but not all, of the developments that are expected to help reshape periodontal therapy over the next 10 years.
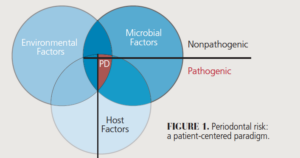
Accurate assessment of individual risk is considered one of the most important aspects of periodontal examination, diagnosis, prognosis and treatment planning. To date, this has been elusive, but, nonetheless, it will remain an important aspect of periodontal research and practice in the years to come. Recognition that periodontitis is a multifactorial disease involving a complex interplay between host, environment and microbes is central to current scientific understanding.1
While it is well accepted that development of periodontitis is intimately associated with the bacteria residing in the subgingival biofilm, it is also evident there are some patients who, despite the presence of considerable plaque deposits, do not develop periodontitis. Conversely there are individuals who develop advanced and destructive forms of periodontitis, yet appear to have minimal deposits of plaque. It seems that although plaque is necessary for periodontitis to develop, it alone is insufficient for the development of periodontal disease.2,3
Indeed, it is now evident that in addition to plaque, other risk factors — such as opportunistic pathogens, environmental influences, genetics, host responses, connective tissue metabolism and bone metabolism — are critical to the clinical manifestation of periodontitis (Figure 1).
Understanding this multifactorial nature has led to the development of a more informed management process. Such processes dictate that, in addition to recognizing the fundamental role of oral hygiene, other risk factors that contribute to periodontitis must be controlled in order for treatment to be successful.4,5 For example, plaque (and its constitutive elements) appears to account for only 20% of the risk for developing periodontitis.6 Therefore, there must be another 80% of risk elements (i.e., modifying and predisposing factors) that must be taken into account when assessing a patient’s periodontal condition. This can be thought of as the personalized medicine/personalized dentistry approach to diagnosing and treating periodontal disease.7
In the future, identifying individual risk factors within the paradigm of personalized medicine/personalized dentistry will become central to periodontal practice. In this context, the emerging field of genomics8,9 will play an increasingly important role. Furthermore, completion of the human genome project now allows the utilization of sophisticated approaches — such as genome-wide screening of populations — to determine the genetic contributions to periodontitis in its various forms.10 That noted, it is recognized that genetics alone cannot fully account for the etiology and progression of the disease process.11
Epigenetics is the study of cellular and physiological phenotypic trait variations caused by external or environmental factors that switch genes on and off.12 Clearly, this has great potential to impact scientific understanding of periodontitis and how environment and genes interact in the clinical manifestation of disease.13,14 However, while it seems entirely probable this extra genetic material may have a great deal of interplay with disease, at present, its role is poorly understood.
Together, these new technologies are sure to represent essential components of future periodontal diagnosis and risk assessment.
HOST-PATHOGEN RELATIONSHIPS
Understanding the central role of the host response in the development of periodontitis also opens new avenues for patient management. These will not replace current treatment approaches of mechanical subgingival debridement, but will serve as adjuncts to traditional approaches to improve and hasten treatment outcomes. It is expected that such adjunct therapies aimed at controlling the host inflammatory response will also result in modification of the subgingival environment and, thus, significantly influence the microbial ecology.
The proposal of the “ecological plaque hypothesis” in 2003 was a significant development in the conceptual understanding of the subgingival environment and how the local environment can influence bacterial composition.15,16 However, this hypothesis was poorly embraced because it was considered discordant with conventional periodontal microbiology concepts at the time that dictated specific bacteria were solely responsible for periodontitis.17 Nonetheless, the concept that host modification of the periodontal pocket whereby inflammatory conditions select for so-called pathogenic species through a process known as “reciprocal interaction” was eventually embraced.18 The process, by which the host can modify the subgingival bacterial environment, has significant ramifications for future host modulation based on controlling the inflammation, rather than focussing solely on elimination of infection.2,19–21
Despite the defining role of the host response, the subgingival microbiota cannot be completely overlooked. Through the unravelling of the human microbiome, current understanding of how microbial communities interact — both with themselves, as well as the host — allows scientists and clinicians to view the periodontal microbiota and its role in the development and progression of periodontitis in a new light.22 Recently, oral microbiologists have proposed the concept of bacterial dysbiosis as playing a key role in the pathogenesis of periodontitis.23,24 In this model, changes within the subgingival milieu cause microbial shifts and imbalances, resulting in the overgrowth of pathogenic microbes.25 This concept of polymicrobial synergy and microbial dysbiosis is well aligned with the role of host modulation of microbial periodontal infection described above, and supports the value of considering host modulation therapy as a viable adjunct to conventional treatment.
PERIODONTAL REGENERATION
Regeneration of tissues damaged by periodontitis has long been considered a key goal of periodontal treatment. Numerous techniques and products have been investigated to achieve periodontal regeneration, and these have generally involved root surface conditioning or implantation of bone substitutes into periodontal defects. Yet, despite efforts to improve periodontal regeneration, each of these procedures remains technique sensitive and clinically unpredictable. This is due, in part, to a lack of understanding of the requirements for periodontal regeneration — namely, the encouragement the regrowth of new cementum, bone and periodontal ligament. Nonetheless, the profession has become obsessed with filling holes in bone rather than studying the natural healing processes required to regenerate the periodontal attachment apparatus.26 A lack of clarity regarding the contribution of the various tissue components in periodontal wound healing explains the widespread misuse of bone transplantation in the treatment of intrabony pockets that pervades some areas of periodontology.27
It is now clear that periodontal regeneration must be founded on sound biologic principles, taking into account each functional stage of reconstruction.28 By applying biologically sound principles to the problem of periodontal regeneration, the clinical procedure of guided tissue regeneration (GTR) was developed in the 1980s.29 At the time, this was a significant advance. However, it soon became apparent that although periodontal regeneration was possible, it was difficult to achieve reliably due to a vast range of patient and operator variables.30 More recently, the application of biological agents onto root surfaces has been shown to induce significant regeneration of damaged periodontal tissues.31 Compared to GTR, an advantage is that biological agents are simpler to use and provide comparable — and sometimes superior — results.32 Like GTR clinical outcomes, the regenerative capacity of biologic agents depends on many variables.
In recent years, implantation of mesenchymal stem cells into periodontal defects has been investigated as a means of inducing periodontal regeneration.33 The first report about the isolation and characterization of periodontal ligament stem cells was published in 2004, and since then the field of dental stem cells has advanced quickly, particularly with regard to its potential use for periodontal regeneration.34–37
Another recent development is the utilization of gene therapy for periodontal regeneration. However, this technology requires extremely sophisticated technical manipulation of cells and also results in considerable caries morbidity issues.38,39
In order for these cell-based regenerative therapies to be successful, suitable delivery devices will need to be developed so the cells can be successfully delivered to the sites of interest. The development of biocompatible scaffolds will be crucial in the next phases of this technology.40 Indeed, this is an active area of research involving the development of biodegradable materials, smart materials and three-dimensional bioprinting.41–45
While the field of cell-based tissue engineering for periodontal regeneration is exciting and the future looks promising, considerable work must be done before such modalities can become a reliable and predictable approach to treatment. This will involve large-scale collaborative efforts between bioengineers, nanotechnologists, cell biologists and molecular biologists. As the field advances, other significant issues will include biosafety and sound manufacturing principles, as well controlling the cost of such technologies.
PERIODONTAL MEDICINE
The term “periodontal medicine” was coined in 1996.46 In the ensuing years, the field has developed rapidly and generally encompasses the interactions between periodontal health and disease, and systemic health and disease. The defining concept is that periodontal inflammation and the periodontal microbiome interact, resulting in a significant increase in the overall level of systemic inflammation. In turn, this influences the incidence, severity and progression of other chronic inflammatory conditions. Furthermore, it has been proposed there may be a bidirectional relationship between periodontitis and some systemic conditions, in which periodontitis can affect systemic health — and the opposite may also occur.
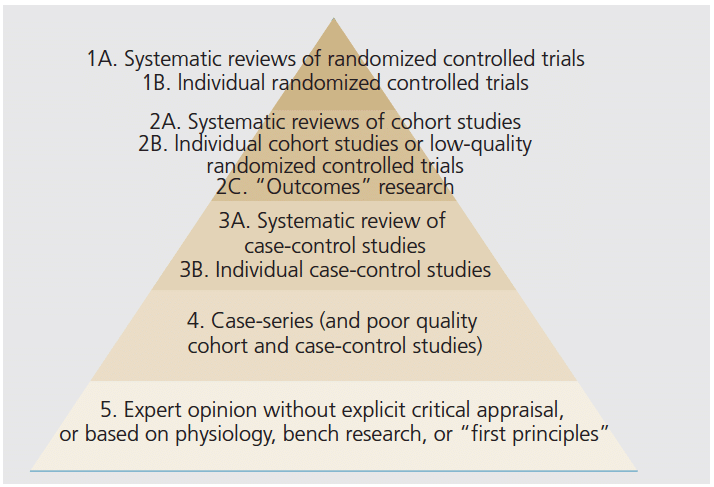
 The interest in periodontal/systemic relationships has resulted in the number of conditions associated with periodontitis growing to unrealistic levels. Therefore, it is timely to consider these reported associations and their relevance to periodontal medicine. The continually expanding list of conditions supposedly associated with periodontitis is becoming problematic. A literature search will reveal an increasing number of reports of associations that have poor biologic plausibility and lack critical scientific assessment. Indeed, there are more than 100 periodontal/systemic associations reported in the literature, most of which are observational studies based on sources of very low evidence. It is well recognized there are many levels of evidence that vary in significance (Figure 2), ranging from so-called expert opinion (the lowest form of evidence) to systematic reviews and randomized clinical trials (the highest forms of evidence). When evaluating the literature, the strength of the evidence presented must be taken into account.
The interest in periodontal/systemic relationships has resulted in the number of conditions associated with periodontitis growing to unrealistic levels. Therefore, it is timely to consider these reported associations and their relevance to periodontal medicine. The continually expanding list of conditions supposedly associated with periodontitis is becoming problematic. A literature search will reveal an increasing number of reports of associations that have poor biologic plausibility and lack critical scientific assessment. Indeed, there are more than 100 periodontal/systemic associations reported in the literature, most of which are observational studies based on sources of very low evidence. It is well recognized there are many levels of evidence that vary in significance (Figure 2), ranging from so-called expert opinion (the lowest form of evidence) to systematic reviews and randomized clinical trials (the highest forms of evidence). When evaluating the literature, the strength of the evidence presented must be taken into account.
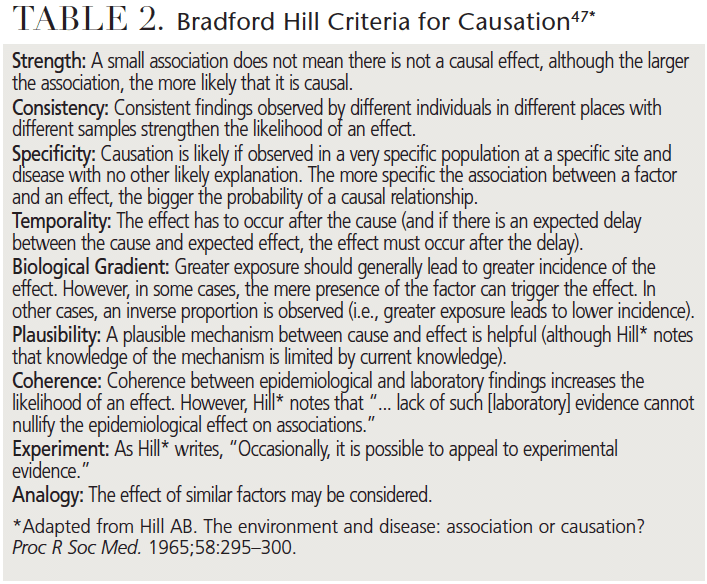
Another issue that must be considered is causality versus association. While associations can be made easily, causality is a far more complex problem. Hill’s47 criteria was developed to help determine causality (Table 2). If one considers these criteria, it would appear unlikely that periodontitis will be determined to be causal of other conditions. However, disease associations may be just as important to understand because they allow researchers to identify conditions and individuals who are likley to agreggate with common conditions and underlying pathologic processes. A disease association checklist has been proposed to help determine how a condition may be related to periodontitis.48 By answering four questions (Table 3, page 22), it should be possible to determine the significance of an association, and whether it is likely to be real or spurious.
The emergence of periodontal medicine as a subdiscipline of periodontology has resulted in a new direction in the understanding of periodontal disease. Classical periodontal therapy has been focused only within the oral environment to preserve or restore the structure, function and esthetics of the dentition. However, science’s current understanding that periodontal inflammation and infection may be intricately associated with other chronic systemic conditions has led to a new focus directed to whole body health, and managing the negative effects of periodontitis on systemic health.
 While the emergence of periodontal medicine is an important development, clinicians and researchers must be mindful to focus only on those associations that have been established through sound scientific investigation, and not merely poorly founded observational studies. At a joint meeting of the American Academy of Periodontology and European Federation of Periodontology, it was concluded there was evidence in the literature to support the concept that periodontitis is associated with some, but not all, of the diseases and conditions reviewed.49 Currently, it appears that the conditions with the strongest evidence for association with periodontitis are cardiovascular disease, diabetes mellitus, obesity, metabolic syndrome and rheumatoid arthritis.
While the emergence of periodontal medicine is an important development, clinicians and researchers must be mindful to focus only on those associations that have been established through sound scientific investigation, and not merely poorly founded observational studies. At a joint meeting of the American Academy of Periodontology and European Federation of Periodontology, it was concluded there was evidence in the literature to support the concept that periodontitis is associated with some, but not all, of the diseases and conditions reviewed.49 Currently, it appears that the conditions with the strongest evidence for association with periodontitis are cardiovascular disease, diabetes mellitus, obesity, metabolic syndrome and rheumatoid arthritis.
Periodontal medicine opens new vistas in periodontology, especially in the fields of using a medical approach to diagnosis and treatment. It also promotes closer interactions with medical colleagues, as well as educational opportunities to alert both the profession and community to the most significant interrelationships, and how these may impact general health and well being.
CONCLUDING COMMENTS
While there are many important topics that could be addressed, the topics that were selected for this review illustrate both the challenges facing periodontology, and the robust nature of this specialty. All of the topics and areas chosen for discussion have the potential to significantly impact prevention, diagnosis and management of one of the most common chronic inflammatory conditions afflicting humans. As periodontology and dentistry continue to evolve, one thing is abundantly clear: The future is exciting.
KEY TAKEAWAYS
- Accurate assessment of individual risk is considered one of the most important aspects of periodontal examination, diagnosis, prognosis and treatment planning.
- It is now evident that in addition to plaque, other risk factors — such as opportunistic pathogens, environmental influence, genetic factors, host responses, connective tissue metabolism and bone metabolism — are critical to the clinical manifestation of periodontitis.
- In the future, identifying individual risk factors within the paradigm of personalized medicine/personalized dentistry will become central to periodontal practice.
- In this context, the emerging field of genomics8,9 will play an increasingly important role Epigenetics has great potential to impact scientific understanding of periodontitis and how environment and genes interact in the clinical manifestation of disease.13,14 At present, however, its role is poorly understood.
- While the future looks promising for cell-based tissue engineering for periodontal regeneration, considerable work must be done before such modalities can become a reliable and predictable approach to treatment.
REFERENCES
- Genco RJ, Borgnakke WS. Risk factors for periodontal disease. Periodontol 2000. 2013;62:59–94.
- Bartold PM, Van Dyke TE. Periodontitis: a host-mediated disruption of microbial homeostasis. Unlearning learned concepts. Periodontol 2000. 2013;62:203–217.
- Clarke NG, Hirsch RS. Personal risk factors for generalized periodontitis. J Clin Periodontol. 1995;22:136–145.
- Braun TM, Doucette-Stamm L, Duff GW, Kornman KS, Giannobile WV. Counterpoint: risk factors, including genetic information, add value in stratifying patients for optimal preventive dental care. J Am Dent Assoc. 2015;146:174–178.
- Lang NP, Suvan JE, Tonetti MS. Risk factor assessment tools for the prevention of periodontitis progression a systematic review. J Clin Periodontol. 2015;42(Suppl 16):S59–S70.
- Grossi SG, Zambon JJ, Ho AW, et al. Assessment of risk for periodontal disease. I. Risk indicators for attachment loss. J Periodontol. 1994;65:260–267.
- Kornman KS, Duff GW. Personalized medicine: will dentistry ride the wave or watch from the beach? J Dent Res. 2012;91(Suppl 7):8S–11S.
- Grant MM. What do ‘omic technologies have to offer periodontal clinical practice in the future? J Periodontal Res. 2012;47:2–14.
- Trindade F, Oppenheim FG, Helmerhorst EJ, Amado F, Gomes PS, Vitorino R. Uncovering the molecular networks in periodontitis. Proteomics Clin Appl. 2014;8:748–761.
- Vaithilingam RD, Safii SH, Baharuddin NA, et al Moving into a new era of periodontal genetic studies: relevance of large case-control samples using severe phenotypes for genome-wide association studies. J Periodontal Res. 2014;49:683–695.
- American Dental Association Council on Scientific Affairs. Genetics and oral health. Available at: ada.org/en/member-center/oral-health-topics/genetics-and-oral-health. Accessed October 3, 2017.
- Barros SP, Offenbacher S. Epigenetics: connecting environment and genotype to phenotype and disease. J Dent Res. 2009;88:400–408.
- Barros SP, Offenbacher S. Modifiable risk factors in periodontal disease: epigenetic regulation of gene expression in the inflammatory response. Periodontol 2000. 2014;64:95–110.
- Larsson L, Castilho RM, Giannobile WV. Epigenetics and its role in periodontal diseases: a state-of-the-art review. J Periodontol. 2015;86:556–568.
- Marsh PD, Head DA, Devine DA. Ecological approaches to oral biofilms: control without killing. Caries Res. 2015;49(Suppl 1):46–54.
- Marsh PD. Dental diseases-are these examples of ecological catastrophes? Int J Dent Hyg. 2006;4(Suppl 1):3–10.
- Feres M, Cortelli SC, Figueiredo LC, Haffajee AD, Socransky SS. Microbiological basis for periodontal therapy. J Appl Oral Sci. 2004;12:256–266.
- Socransky SS, Haffajee AD. Periodontal microbial ecology. Periodontol 2000. 2005;38:135–187.
- Gokhale SR, Padhye AM. Future prospects of systemic host modulatory agents in periodontal therapy. Br Dent J. 2013;214:467–471.
- Elavarasu S, Sekar S, Murugan T. Host modulation by therapeutic agents. J Pharm Bioallied Sci. 2012;4(Suppl 2):S256–S259.
- Hasturk H, Kantarci A, Van Dyke TE. Paradigm shift in the pharmacological management of periodontal diseases. Front Oral Biol. 2012;15:160–176.
- Darveau RP. Periodontitis: a polymicrobial disruption of host homeostasis. Nat Rev Microbiol. 2010;8:481–490.
- Hajishengallis G. Periodontitis: from microbial immune subversion to systemic inflammation. Nat Rev Immunol. 2015;15:30–44.
- Pérez-Chaparro PJ, Gonçalves C, Figueiredo LC, et al. Newly identified pathogens associated with periodontitis: a systematic review. J Dent Res. 2014;93:846–858.
- Darveau RP, Hajishengallis G, Curtis MA. Porphyromonas gingivalis as a potential community activist for disease. J Dent Res. 2012;91:816–820.
- Becker W, Becker BE. Periodontal regeneration: a contemporary reevaluation. Periodontol 2000. 1999;19:104–114.
- Karring T, Nyman S, Lindhe J, Sirirat M. Potentials for root resorption during periodontal wound healing. J Clin Periodontol. 1984;11:41–52.
- Bartold PM, McCulloch CA, Narayanan AS, Pitaru S. Tissue engineering: a new paradigm for periodontal regeneration based on molecular and cell biology. Periodontol 2000. 2000;24:253–269.
- Karring T, Nyman S, Gottlow J, Laurell L. Development of the biological concept of guided tissue regeneration — animal and human studies. Periodontol 2000. 1993;1:26–35.
- Reynolds MA, Kao RT, Camargo PM, et al. Periodontal regeneration — intrabony defects: a consensus report from the AAP Regeneration Workshop. J Periodontol. 2015;86(Suppl 2):S105–S107.
- Stavropoulos A, Wikesjö UM. Growth and differentiation factors for periodontal regeneration: a review on factors with clinical testing. J Periodontal Res. 2012;47:545–553.
- Koop R, Merheb J, Quirynen M. Periodontal regeneration with enamel matrix derivative in reconstructive periodontal therapy: a systematic review. J Periodontol. 2012;83:707–720.
- Bassir SH, Wisitrasameewong W, Raanan J, et al. Potential for stem cell-based periodontal therapy. J Cell Physiol. 2016;231:50–61.
- Seo BM, Miura M, Gronthos S, et al. Investigation of multipotent postnatal stem cells from human periodontal ligament. Lancet. 2004;364:149–155.
- Bartold PM, Gronthos S. Standardization of criteria defining periodontal ligament stem cells. J Dent Res. 2017;96:487–490.
- Zhu W, Liang M. Periodontal ligament stem cells: current status, concerns, and future prospects. Stem Cells Int. 2015;2015:972313.
- Hynes K, Menicanin D, Gronthos S, Bartold PM. Clinical utility of stem cells for periodontal regeneration. Periodontol 2000. 2012;59:203–227.
- Rios HF, Lin Z, Oh B, Park CH, Giannobile WV. Cell- and gene-based therapeutic strategies for periodontal regenerative medicine. J Periodontol. 2011;82:1223–1237.
- Su F, Liu SS, Ma JL, Wang DS, E LL, Liu HC. Enhancement of periodontal tissue regeneration by transplantation of osteoprotegerin-engineered periodontal ligament stem cells. Stem Cell Res Ther. 2015;6:22.
- Bartold PM, Xiao Y, Lyngstaadas SP, Paine ML, Snead ML. Principles and applications of cell delivery systems for periodontal regeneration. Periodontol 2000. 2006;41:123–135.
- Rasperini G, Pilipchuk SP, Flanagan CL, et al. 3D-printed bioresorbable scaffold for periodontal repair. J Dent Res. 2015;94(Suppl 9):153S–157S.
- Bartold PM, Gronthos S, Ivanovski S, Fisher A, Hutmacher DW. Tissue engineered periodontal products. J Periodont Res. 2016;51:1–15.
- Obregon F, Vaquette C, Ivanovski S, Hutmacher DW, Bertassoni LE. Three-dimensional bioprinting for regenerative dentistry and craniofacial tissue engineering. J Dent Res. 2015;94(Suppl 9):143S–152S.
- Ivanovski S, Vaquette C, Gronthos S, Hutmacher DW, Bartold PM. Multiphasic scaffolds for periodontal tissue engineering. J Dent Res. 2014;93:1212–1221.
- Park CH, Kim KH, Rios HF, Lee YM, Giannobile WV, Seol YJ. Spatiotemporally controlled microchannels of periodontal mimic scaffolds. J Dent Res. 2014;93:1304–1312.
- Offenbacher S. Periodontal diseases: pathogenesis. Ann Periodontol. 1996;1:821–878.
- Hill AB. The environment and disease: association or causation? Proc R Soc Med. 1965;58:295–300.
- Bartold PM, Mariotti A. The future of periodontal-systemic associations: raising the standards. Curr Oral Health Rep. 2017;4:258–262.
- Linden GJ, Lyons A, Scannapieco FA. Periodontal systemic associations: review of the evidence. Jointly published in: J Clin Periodontol. 2013;40(Suppl 14):S8–S19. J Periodontol. 2013;84(Suppl 4):S8–S19
The author has no commercial conflicts of interest to disclose.
FEATURED IMAGE: BRIANAJACKSON/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. January 2018;4(1):8-10,12.
