

The Evolution of Cone-Beam Computed Tomography
Advancements in this digital diagnostic technology have helped support precision while optimizing patient care.
Over the past three decades, the use of cone-beam computed tomography (CBCT) has increased due to the advances in image quality, digital dentistry, and artificial intelligence, as well as the decreased radiation exposure and lower equipment costs.1-3 Cone-beam technology provides tremendous benefits to clinicians and patients in diagnosis, treatment planning, and post-treatment assessment.
The need for dental CBCT imaging has evolved primarily due to the limitations in traditional radiographic techniques, such as panoramic and intraoral imaging. Additionally, the high radiation doses to produce an image and the lack of accessibility to medical CT machines made these machines unfeasible for dental use. These more traditional forms of two-dimensional (2D) dental radiography come with many disadvantages, including image magnification and distortion, as well as superimposition and distortion of structures.4,5 Despite these limitations, CBCT is not recommended as a replacement for more traditional radiography techniques but rather as an adjunct that should be limited to specific applications.1
CBCT machines function by acquiring several hundred 2D projections as the X-ray source and flat detector rotate around a point located in the center of the area of interest. These projections are then rendered into a three-dimensional (3D) volume.3
One of the primary advantages of CBCT, when compared to multidetector computed tomography (MDCT), is the significantly lower dosage employed by the imaging modality (resulting from a lower current).6 However, this comes at the expense of increased noise levels, lower contrast resolution, and the characteristically poor soft-tissue contrast seen in dental CBCT images compared to MDCTs.6
Additionally, with scan times typically ranging from 10 to 20 seconds, CBCT images often experience motion-induced artifacts.1,7 These artifacts can be mitigated with machine designs that allow the patient to remain seated or with the utilization of patient stabilizers, but they cannot be eliminated entirely.
Dose Optimization
One of the most important principles to consider regarding any radiographic examination is the principle of keeping radiation exposure to dental patients “as low as reasonably achievable;”8 otherwise known as the ALARA rule. With the emergence of CBCT came the ability for operators to control field of view (FOV) and voxel size to optimize the dose delivered to the patient.3 This has led to a new concept in dental radiography: CBCT images should be captured in a FOV and resolution that is “as low as diagnostically acceptable,” or ALADA, in a similar effort to minimize patient exposure.8
Advantages and Limitations
The most significant advantage of CBCT is its capability to overcome the limitations that accompany conventional 2D radiography. A 3D image offers crucial insights into complex anatomical structures and pathoses that are often impossible to visualize in a 2D image.9 When compared to conventional CT machines, CBCT machines offer rapid scan time, lower radiation dose, lower cost, greater availability, and high image accuracy.6
Although CBCT presents a variety of advantages over alternative imaging modalities, limitations remain. The most well-known is the poor soft tissue contrast that is inherent in CBCT images when compared to conventional CT machines. This is a product of increased image noise and the divergence of the X-ray beam.10 The second limitation of CBCT imaging is image artifacts. Artifacts are distortions or errors in an image unrelated to the scan’s subject. Artifacts may be caused by beam hardening due to metal crowns, implants, gutta-percha, or silver posts in endodontically treated teeth resulting in streaks and dark bands; patient-related artifacts (patient motion); and scanner-related artifacts (ring-shaped artifact from improper calibration).10
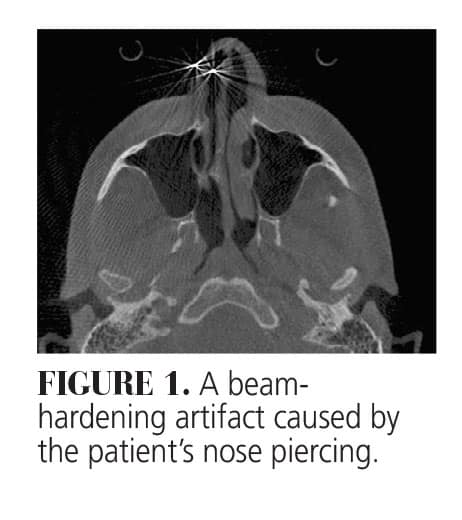 Figure 1 provides a great visual for how beam hardening artifacts appear on CBCT scans surrounding metal objects. In this case, the artifact results from the patient leaving her nose ring in for the scan. Although the nose ring is unlikely to affect diagnostic interpretation, beam hardening resulting from gutta percha, dental implants, or a metal post can be far less innocuous.
Figure 1 provides a great visual for how beam hardening artifacts appear on CBCT scans surrounding metal objects. In this case, the artifact results from the patient leaving her nose ring in for the scan. Although the nose ring is unlikely to affect diagnostic interpretation, beam hardening resulting from gutta percha, dental implants, or a metal post can be far less innocuous.
CBCT has proven to be a valuable diagnostic imaging technique for endodontics, periodontics, implantology, orthodontics, temporomandibular joint (TMJ) analysis, soft tissue (airway) analysis, diagnosis of hard tissue pathology and facial fractures, and even forensic odontology.1
Implantology
The expansion of dental implantology within modern practice has played an instrumental role in expanding CT technology into dentistry. CBCT is now regarded as the gold standard in dental implant surgical planning.11 The case below highlights a patient interested in replacing congenitally missing lateral incisors (Figure 2A).
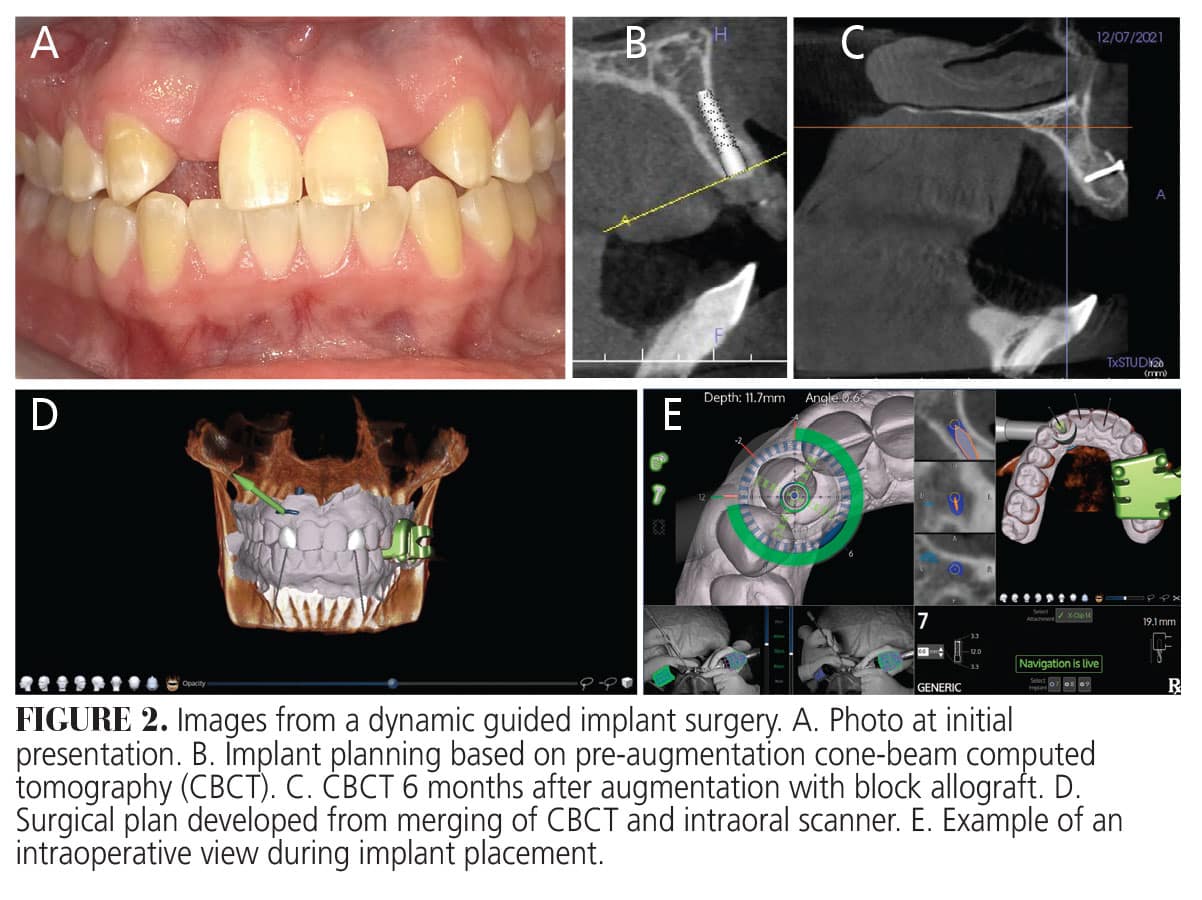
CBCT was used for presurgical assessment and aided in identifying the lack of adequate ridge width for implant placement (Figure 2B). Block allografts were performed at each site, and after 6 months of healing (Figure 2C), implants were placed in the #7 and #10 sites. The crowns were designed, and then the virtual implants were placed, allowing the real implants to be placed in the ideal prosthetic position.
DICOM data from the CBCT and the STL file from the intraoral scanner (IOS) were merged with the software (Figure 2D), and the implants were placed using dynamic guided surgery. This method provides interactive guidance for the clinician by using a sensor above the patient’s head to correlate a tracker fixed to the patient’s arch and a tracker attached to the surgeon’s handpiece (Figure 2E). By preplanning the ideal implant position based upon the CBCT and IOS, the surgeon can confidently perform the osteotomies and implant placement while looking at a screen that guides depth, position, and angulation (Figure 2E).
Endodontics
Research strongly supports the superiority of CBCT over 2D radiography in the assessment of periapical lesions. One area where this superiority is most noteworthy is in precisely assessing lesion juxtaposition to the maxillary sinus.12 Additionally, CBCT has proven useful in endodontics when assessing the number and morphology of roots and canals, determining working length, classifying the source of lesion, and diagnosing horizontal and vertical root fractures.12
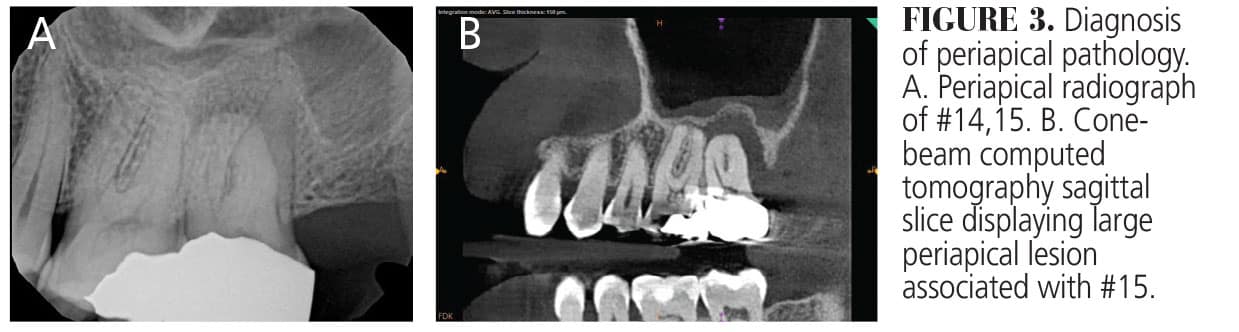
The value of being able to discriminate the boarders and extent of a periapical lesion is displayed in Figures 3A and B (page 24). This patient presented with significant sensitivity to percussion on the upper left molars. A periapical radiograph was taken to assess the area but was inconclusive (Figure 3A). It was not until a CBCT was taken that the lesion could be clearly visualized, leading to the extraction of #15 (Figure 3B).
Orthodontics
The patient in Figure 4 requested orthodontic therapy to fix her crowded teeth (Figure 4A). The full-mouth X-ray did not reveal any interproximal bone loss. After taking a CBCT, however, it was evident that there was little to no bone on the facial of the mandibular anterior teeth (Figures 4B and 4C).
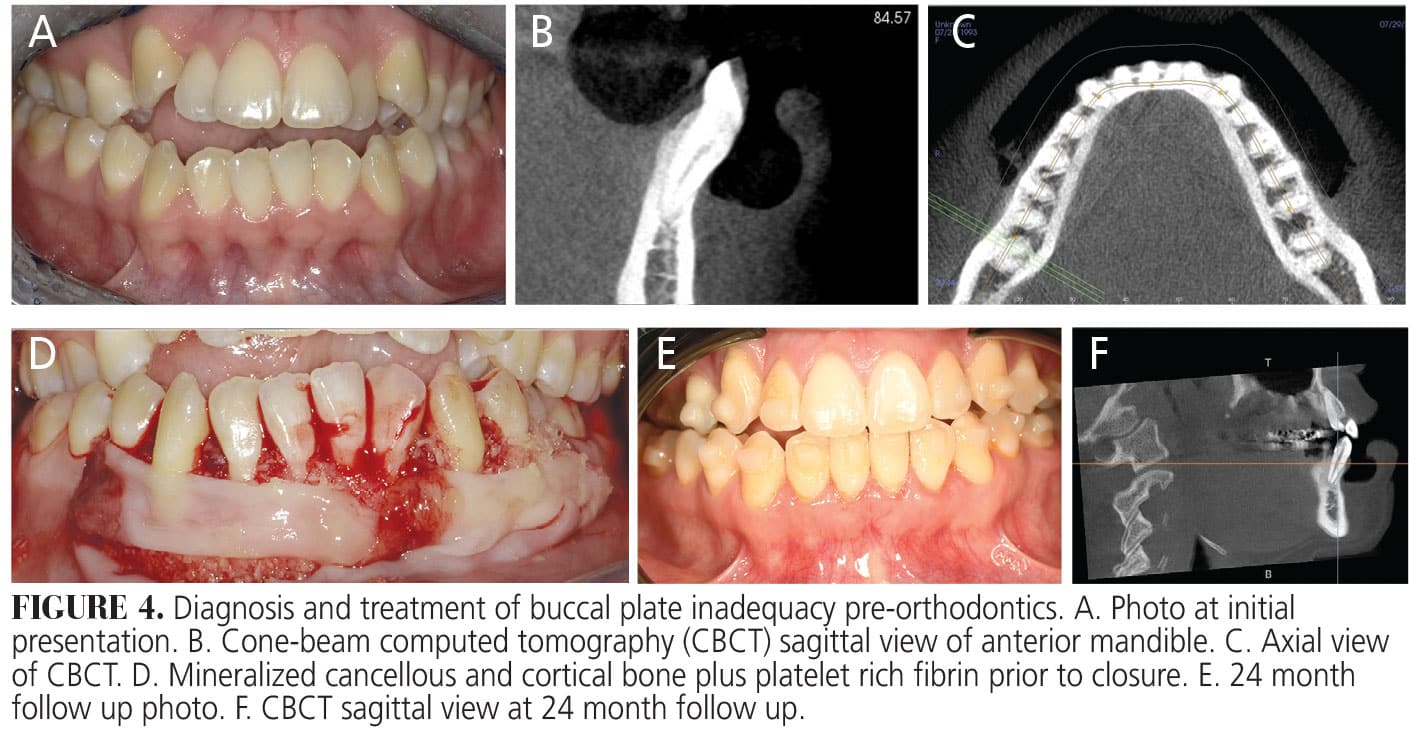
In the CBCT scans, the “lift-lip” technique was utilized in which a cotton roll was inserted into the vestibule, between the lip and alveolus, to aid in the evaluation of the buccal bone thickness.13 It was determined that this patient would benefit from Wilckodontics to activate the bone with the regional acceleratory phenomenon.14 This is characterized by a rapid acceleration of normal cellular processes as a response to noxious stimuli. In this case, the trauma of corticotomies to the alveolar bone allows for increased speed of orthodontic tooth movement.
A full-thickness flap was elevated, and corticotomies were performed with a bur as well as a piezotome. Mineralized cancellous and cortical bone was added, as well as platelet rich fibrin (Figure 4D). The flaps were approximated and sutured with 4-0 polytetrafluoroethylene sutures. Without the use of CBCT, the diagnosis of thin bone and fenestrations could have been easily missed. If traditional orthodontics had been performed, this patient may have had significant recession by the orthodontic expansion of the arch.
At the 24-month follow up, the clinical appearance shows significantly reduced corrugation over the mandibular anterior teeth, and the CBCT assessment shows a significant gain in cortical bone over the facial aspect of the mandibular anterior sextant (Figure 4E and 4F).
Airway Analysis
CBCT has proven to be a useful aid in assessing a patient’s risk for developing obstructive sleep apnea syndrome (OSAS). CBCT is helpful in calculating the total volume of the airways as well as the area in each of the anatomical planes (sagittal, coronal, transverse). These scans can be used to identify the areas of greatest anteroposterior and laterolateral constriction within the airways.15 Because reduction of the oropharyngeal airway space is a significant predisposing factor to OSAS, CBCT analysis can be a useful screening adjunct when determining need for further clinical evaluation or referral.
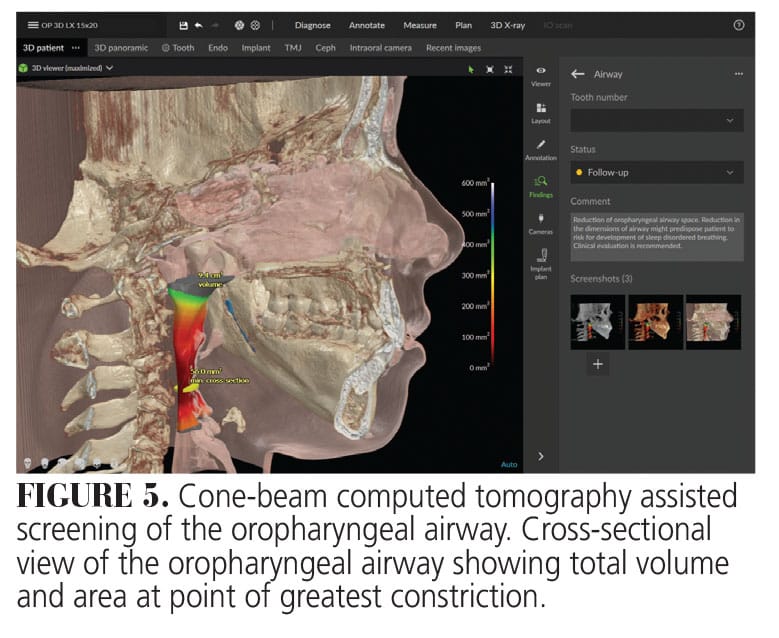
When looking to quantifying risk related to oropharyngeal constriction, an area of < 52 mm2 is considered as having a high risk of OSAS; 52 to 100 mm2, intermediate risk; and > 100 mm2, low risk.16 In the case presented, the patient presents with a 56 mm2 minimum cross-sectional area, placing the risk level at intermediate (Figure 5). Further evaluation would be recommended for this patient, especially in the presence of concurrent risk factors or known symptomology.
Temporomandibular Joint Analysis
A comprehensive analysis of the TMJ complex requires the interpreter to clearly visualize the trabecular pattern of the articular eminence, bony cortices of the head of the condyle and glenoid fossa, calcification level of the head of the condyle, and TMJ spaces. CBCT has proven to be superior to multislice CT and traditional 2D forms of analysis when examining the normal bony anatomy of the TMJ, and when assessing any pathologic or degenerative changes.17 This superiority comes from the ability to produce high resolution images with decreased radiation doses and no superimposition of structures. However, CBCT’s advantage is limited to the osseous components of the TMJ complex, and that magnetic resonance imaging is the preferred imaging modality for assessment of the soft tissue components of the complex due to the notoriously poor soft tissue contrast seen in CBCT imaging.18
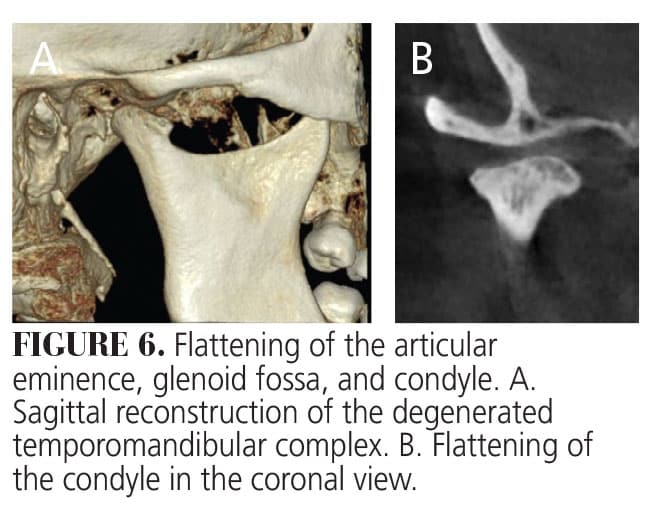
This case highlights the efficacy of CBCT in the assessment of degenerative changes to the TMJ complex. This patient is a 43-year-old woman with moderate to severe flattening of the condylar head, evident in the sagittal (Figure 6A) and coronal (Figure 6B) views. Additionally, an osteophyte can be seen at the anterior portion of the condyle (Figure 6A) and a thickened, sclerotic appearance is seen from the coronal view (Figure 6B). In addition to diagnosing degenerative changes to the TMJ complex, CBCT can be used to diagnose abnormalities during TMJ development, synovial chondromatosis, coronoid hyperplasia, and trauma.17
Conclusion
Since its inception, CBCT has quickly gained profound acceptance and integration into routine dental practice. Given the power of its diagnostic capabilities, it is no surprise that applications have spanned various dental specialties, including endodontics, implantology, orthodontics, oral and maxillofacial surgery, and periodontics. As new technologies emerge and current technology advances, CBCT is poised to play an even more pivotal role in enhancing diagnostic accuracy, treatment planning, and overall patient care.
References
- Jain S, Choudhary K, Nagi R, Shukla S, Kaur N, Grover D. New evolution of cone-beam computed tomography in dentistry: Combining digital technologies. Imaging Sci Dent. 2019;49:179-190.
- Schulz RA, Stein JA, Pelc NJ. How CT happened: the early development of medical computed tomographyJ J Med Imaging (Bellingham). 2021;8:052110.
- Schulze R, Drage N. Cone-beam computed tomography and its applications in dental and maxillofacial radiology. Clinical Radiology. 2020;75(9):647–657.
- White SC, Pharoah MJ. The evolution and application of dental maxillofacial imaging modalities. Dent Clin North Am. 2008;52:689–705.
- Kapshe N, Pujar M, Jaiswal S. (2020). Cone beam computed tomography: areview. International Journal of Oral Health Dentistry. 2020;6:71-77.
- Pauwels R, Beinsberger J, Stamatakis H, et al. Comparison of spatial and contrast resolution for cone-beam computed tomography scanners. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114:127–135.
- Spin‐Neto R, Wenzel A. Patient movement and motion artefacts in cone beam computed tomography of the dentomaxillofacial region: a systematic literature review. Oral Surg Oral Med Oral Pathol Oral Radiol. 2016 Apr 1;121:425–433.
- Benavides E, Krecioch JR, Connolly RT, et al. Optimizing radiation safety in dentistry. J Am Dent Assoc. 2024;155:280-293.
- Tyndall DA, Price JB, Tetradis S, et al. Position statement of the American Academy of Oral and Maxillofacial Radiology on selection criteria for the use of radiology in dental implantology with emphasis on cone beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113:817-826.
- Venkatesh E, Elluru SV. Cone beam computed tomography: basics and applications in dentistry. J Istanb Univ Fac Dent. 2017;51(3 Suppl 1):S102-S121.
- Deporter D, Ebrahimi Dastgurdi M, Rahmati A, G Atenafu E, Ketabi M. CBCT data relevant in treatment planning for immediate maxillary molar implant placement. J Adv Periodontol Implant Dent. 2021;13:49-55.
- Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic applications of cone-beam volumetric tomography. J Endod. 2007;33:1121-1132.
- Rinaldi M, Ganz SD, Mottola A, Lauriola S. Computer-guided applications for dental implants, bone grafting, and reconstructive surgery. Available at http/://ci.nii.ac.jp/ncid/BB18969938. Accessed January 12, 2025.
- Frost HM. The regional acceleratory phenomenon: a review. Henry Ford Hosp Med J. 1983;31:3-9.
- Fonseca C, Cavadas F, Fonseca P. Upper airway assessment in cone-beam computed tomography for screening of obstructive sleep apnea syndrome: development of an evaluation protocol in dentistry. JMIR Res Protoc. 2023;12:e41049.
- Steffy DD, Tang CS. Radiographic evaluation of sleep-disordered breathing. Radiol Clin North Am. 2018;56:177-185.
- Dhabale GS, Bhowate RR. Cone-beam computed tomography for temporomandibular joint imaging. Cureus. 2022;14:e31515.
- Talmaceanu D, Lenghel LM, Bolog N, Hedesiu M, Buduru S, Rotar H, Baciut M, Baciut G. Imaging modalities for temporomandibular joint disorders: an update. Clujul Med. 2018;91:280-287.
From Decisions in Dentistry. January/February 2025;11(1):22-24.
