

Angled Screw-Retained Crowns Advance Esthetics and Function
These new abutments combine the benefits of screw retention with improved esthetics.
Designing a single implant crown in the maxilla has consistently posed challenges, primarily due to the available bone volume and the desired final position of the restoration. In the pursuit of achieving optimal esthetics, a cement-retained implant prosthesis is frequently favored due to its compatibility with anatomical conditions, superior mechanical performance, and a reduced likelihood of mechanical complications. Despite these advantages, the presence of residual cement can lead to potential biological issues, such as peri-implantitis.1
On the other hand, the screw-retained crown offers easy retrievability, thereby avoiding complications arising from residual cement.1,2 Nonetheless, traditional screw-retained restoration designs encounter challenges in adapting to intra-arch spaces and angle correction, along with addressing concerns related to the position of the screw hole access, potential loosening of the screw, and the risk of ceramic chipping.
In 2004, the dynamic abutment was introduced, offering a unique design allowing the screw access angle to deviate from the implant’s angulation.3 This abutment permits adjustments of up to 28°, facilitating screw-retained restorations even in cases where the implant’s angle isn’t ideal. Angle corrections are made prior to casting the restorative framework, enhancing flexibility in implant placement and restoration.
Newly technologies now enable the creation of screw-retained implant-supported restorations utilizing an angled screw-channel (ASC) abutment system. This approach offers the advantages of a screw-retained crown, ensuring easy retrieval, while also mitigating the risk of cement-related peri-implantitis. Moreover, the system considers the natural angulation of teeth in the maxilla and addresses the typical challenges posed by the anatomy of the esthetic zone.4
Implant Digital Planning and Screw Positioning
Prostheses supported by implants employing the ASC system yield favorable outcomes in both anterior and posterior regions. This is achieved by the strategic relocation of the access hole to the lingual face in anterior teeth or the occlusal surface in posterior teeth, allowing for precise control over the material thickness.
 The placement of dental implants in the anterior maxilla is challenging because of esthetic and functional considerations,5 as the screw hole primarily affects the esthetic outcome. To address this, the primary objective was to position the implant in a palatal/lingual orientation, facilitating a palatal emergence of the screw channel. This involved placing the implant 1.5 to 2.0 mm palatal to the incisal margin of the central maxillary incisors, while ensuring a minimum of 2 mm of buccal bone remained.6
The placement of dental implants in the anterior maxilla is challenging because of esthetic and functional considerations,5 as the screw hole primarily affects the esthetic outcome. To address this, the primary objective was to position the implant in a palatal/lingual orientation, facilitating a palatal emergence of the screw channel. This involved placing the implant 1.5 to 2.0 mm palatal to the incisal margin of the central maxillary incisors, while ensuring a minimum of 2 mm of buccal bone remained.6
However, this palatal placement compromises the esthetic outcomes and the implant survivability7 as it results in a final restoration with an excessively convex contour and a collapsed soft tissue at 1 year follow up. For the same reason, Testori et al7 suggested that the long axis of the fixture should correspond to the incisal edge of the future crown to allow for a more natural emergence angle (15°).
In an observational study to determine the prevalence of digitally placed implants in the anterior maxilla that would allow screw-retained implant-supported restorations with either a straight or an ASC abutment, out of the 200 virtually placed implants, 48 (24%) permitted screw-retained restorations with a straight abutment, while the remaining 152 (76%) necessitated an angled abutment, requiring angular corrections of ≤15°.8 All digitally placed implants in this study were eligible for screw-retained restorations, eliminating the need for cement-retained restorations within the study’s scope.
Clinical Longevity and Success Rates
The most common complications of implant-supported prostheses are screw loosening, screw fracture, and implant fracture. Among them, screw loosening is the most common. It can be caused by several factors, including screw settling, excessive screw thread, and internal surface during loading.4
In a longitudinal retrospective study, with 105 subjects, and 162 implants, the survival rate of implant-supported prostheses adopting ASC were 92%, similar to what is reported for conventional screw-retained restorations.9 The results provide a favorable outcome both in the posterior and anterior regions and can therefore be adopted to treat cases where the implant angulation is unfavorable for a conventional screw-retained prosthesis. Monolithic zirconia restorations (n = 52) had a higher success rate (95%) when compared to partially veneered restorations (n = 53), which experienced an elevated number of complications (90%).
Several systematic reviews have confirmed that both retention systems are equally satisfactory.10,11 Cement-retained systems can be useful to correct unfavorable angulation without exerting additional stress on the crestal bone.10 Screw-retained systems allows easy retrieval and better marginal fit at the crown-implant interface, but with higher rates of prosthetic complications.11 As such, clinicians need data on the clinical outcomes they might expect when dealing with either of the two systems.
A recent meta-analysis12 reported greater marginal bone level changes and lower bleeding on probing at short term (1 year) and similar outcome at medium term (3 to 4 years) for the screw-retained vs cement-retained implant crowns. One explanation is that cement materials may act as a filling material and absorb stresses. Other clinical factors (eg, probing depth, plaque index, papilla index, pink esthetic scores and soft tissue thickness) were deemed similar at short- and medium-term periods.
A greater plaque accumulation and probing depth for cement-retained crowns have also been reported.13 An acceptable explanation for this outcome is that the submucosal interface between the crown and implant abutment results in excessive cement left in the peri-implant tissue, leading to a higher bleeding index. The meta-analysis concluded that, on the short-term, both systems are suitable for retention, especially when used with zirconia abutments and that other factors, such as the dentist’s expertise, may affect the outcomes.
A recent study on abutment screw torque loss showed that crowns with ASC on a narrow diameter implant with original components may perform better than those with nonoriginal components.14 A high percentage of abutment screw torque loss was observed, and periodic recall of the restoration should be planned to check for torque loss. They concluded that the design of the screws could be the most important factor contributing to screw loosening. In this study, screws used for NB-0, NB-20, and DA-20, have tapered-head screws, while ATL-20 used flat-head screws.
Technical considerations about Angled Screw Channel abutments
In 2004, the dynamic abutment was introduced3 to allow the angulation of the screw access to diverge from the implant axis up to 28°. This abutment consists of a base with a semisphere on which a burnout chimney sits, and which can be freely moved to deviate from the axis by up to 28°. The fixation screw is unique and allows tightening while off axis with a screwdriver with a hexagonal 1.30-mm-faceted sphere. This system is compatible with many major implant systems. An alternative to the direct abutment is the angled screw-channel abutment system, which would facilitate the retrieval of a screw-retained crown and avoid the problems associated with a cement-retained crown. The use of ASC abutments facilitated the placement of a screw-retained implant restoration in 76% of the time.8
Various types of angled screw channel abutments are available, with the titanium base being the most commonly used. Many implant manufacturers offer variations of these bases. Additionally, third-party manufacturers produce angled bases compatible with various companies. Thus, even if the implant system lacks an angled solution, alternatives may still be accessible regardless of the manufacturer.
The titanium bases share a uniform design and function. They are primarily utilized for screw-retained restorations, where the crown is fabricated with an access hole and subsequently cemented to the base in the laboratory. Titanium bases for angled solutions usually offer only one margin height option, which can occasionally pose a challenge for implants placed deeply. Moreover, the width of the base, coupled with the thickness of the restorative material, may lead to excessive blanching or even interference with the bone.
The ASC abutment combines zirconia with a mechanically retained titanium base, eliminating the need for cement. These versatile ASC abutments can be configured as full-contour zirconia crowns or with cutback options for direct porcelain stacking. Additionally, they can serve as custom zirconia abutments for screwmentable crowns. Another advantage is their availability with nonengaging titanium bases, suitable for bridge applications.
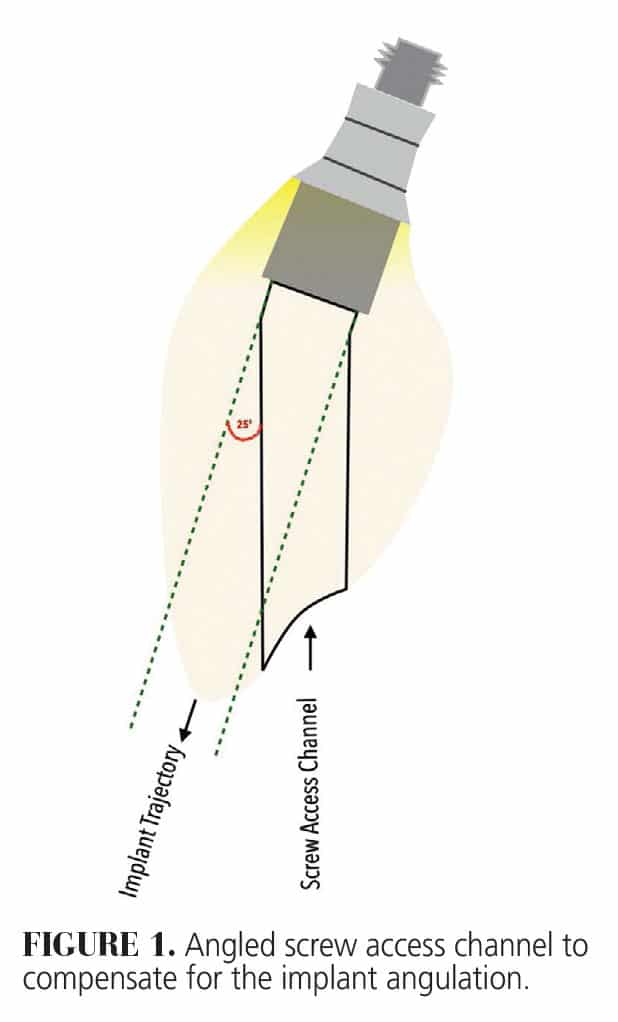
 Operating via the Omnigrip screw, they require a specialized driver but maintain torque at 35 Ncm. The access hole can be adjusted up to 25° (Figure 1). However, limitations in abutment thickness may be influenced by implant placement and available space. Caution is advised during handling to prevent the loss of the semi-loosely fitting titanium base, which holds the two components together when torqued into place.
Operating via the Omnigrip screw, they require a specialized driver but maintain torque at 35 Ncm. The access hole can be adjusted up to 25° (Figure 1). However, limitations in abutment thickness may be influenced by implant placement and available space. Caution is advised during handling to prevent the loss of the semi-loosely fitting titanium base, which holds the two components together when torqued into place.
In addition to the titanium bases, some companies offer alternative ASC options instead of standard bases. For instance, customized and directly veneerable bases are available in a single abutment piece, ensuring an individualized emergence profile created according to the patient’s specific situation. These customized abutments deliver high esthetics outcomes for single tooth screw-retaining restorations, with a screw channel angulation of up to 30°.
Other custom ASC abutments provide precise control over design elements including height, margin placement, and emergence profile. These options are tailored for patient-specific and screw-retained single-tooth restorations for various implant systems. The angled screw access channel allows for optimal positioning, improving esthetics and installation procedures. With the ability to angle the screwdriver access channel up to 30° off the implant axis, these bases ensure secure screw capture within the abutment/crown after cementation, eliminating the need for subsequent removal.
Case Report
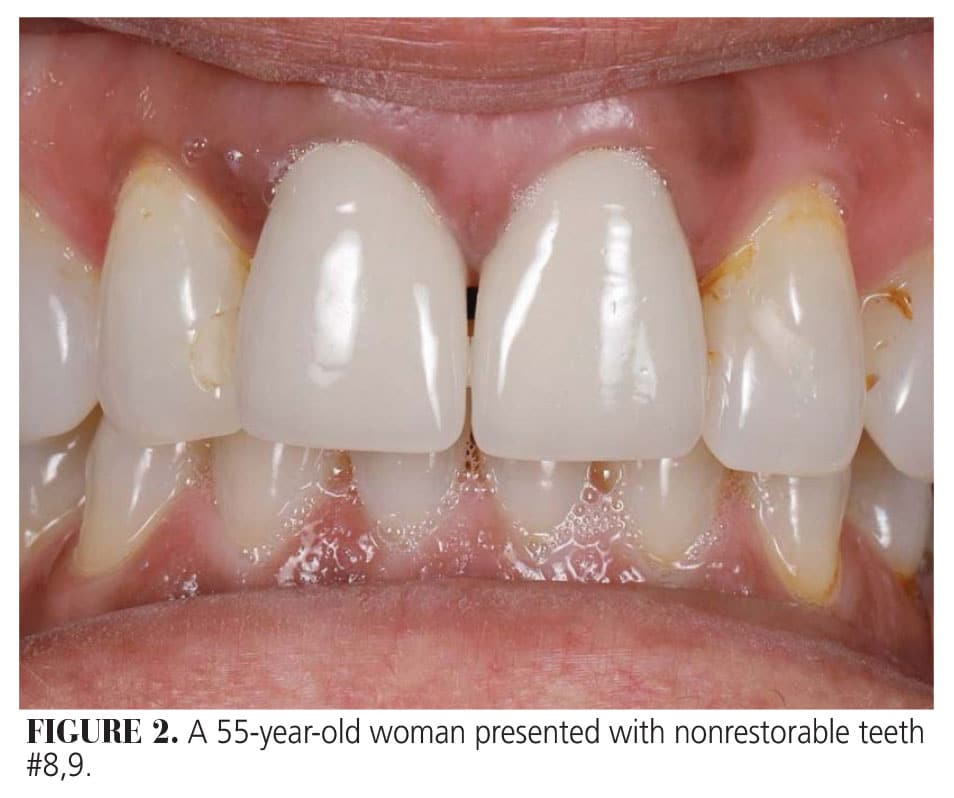
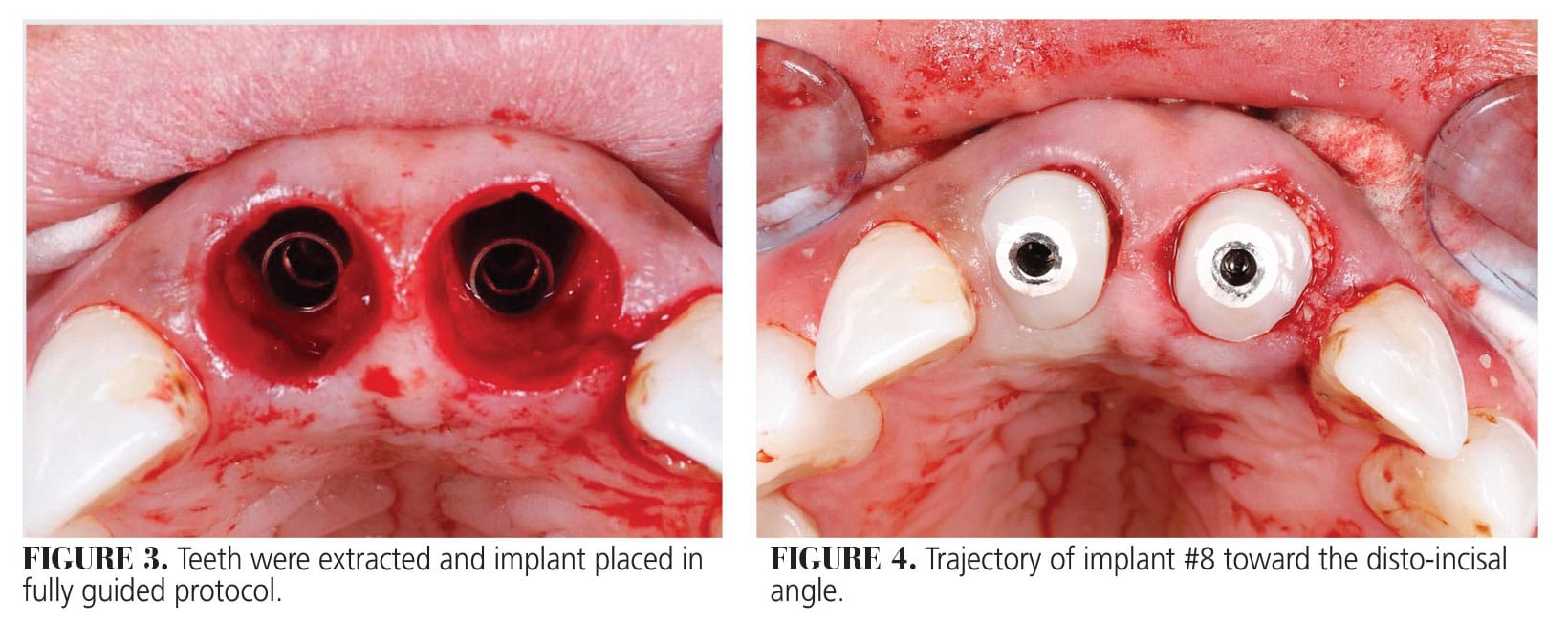
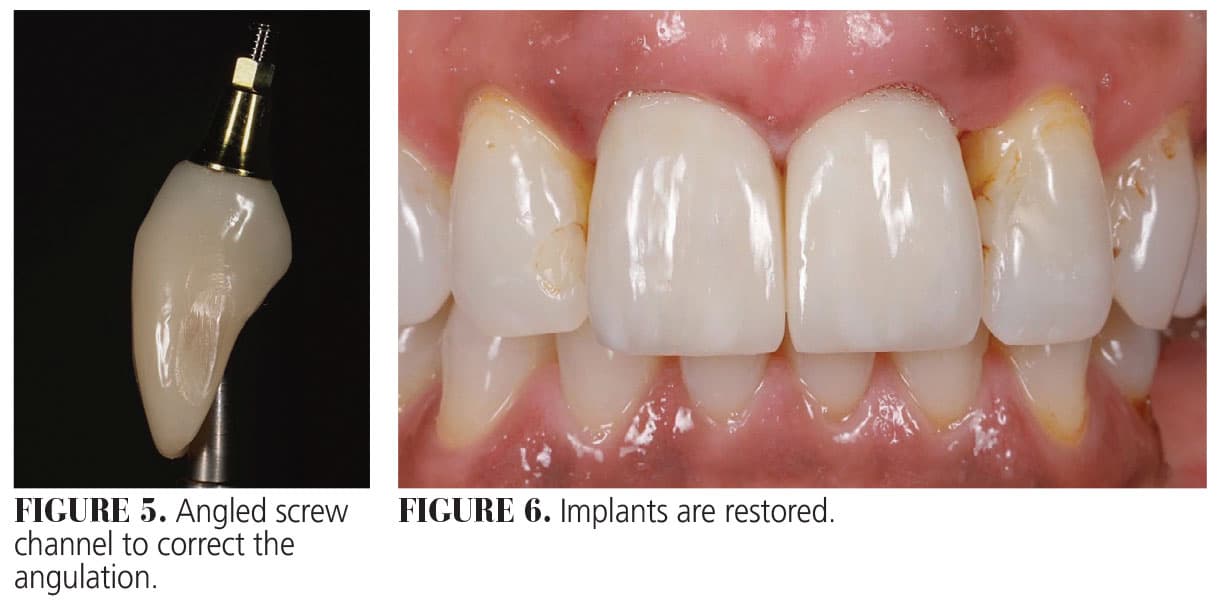
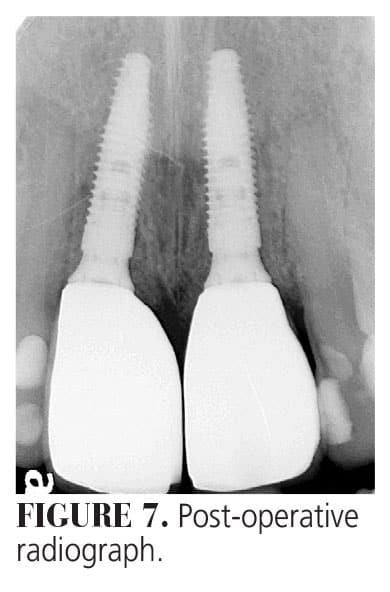
A 55-year-old woman presented to a private practice in Ontario, Canada, with nonrestorable teeth #8,9 (Figure 2). Teeth were extracted with minimal trauma. Due to anatomic limitations, implant #8 was planned to avoid the existing nasopalatine canal with its emergence toward the disto-incisal aspect (Figures 3 and 4), which would not allow the use of a screw-retained crown as the screw access would be emerging from the incisal edge, compromising esthetics and function. Therefore, an ASC was used to compensate for its angulation (Figure 5) and both implants were restored with screw-retained crowns (Figures 6 and 7), with the screw access from the palatal aspect of the crown.
Limitations
 ASC abutments have inherent limitations across all systems. One major restriction is the degree to which the screw access hole can be angled. While this varies slightly by manufacturer, the angulation typically allows correction for access holes emerging at incisal edges or cusps but not through the facial or buccal surfaces.
ASC abutments have inherent limitations across all systems. One major restriction is the degree to which the screw access hole can be angled. While this varies slightly by manufacturer, the angulation typically allows correction for access holes emerging at incisal edges or cusps but not through the facial or buccal surfaces.
Additionally, despite the angled channel, the abutment itself extends straight from the implant. This design can create bulky contours on the crown’s facial side, particularly in cases of suboptimal implant placement. The need for larger access holes to accommodate the tilted screw during insertion is another drawback. Reducing the access hole size is possible but would make the screw captive within the crown after cementation. Although tightening or loosening the screw remains possible, replacement would require separating the crown from the abutment.
Lastly, ASC abutments necessitate the use of a specialized screwdriver. While the screw remains fixed at an angle, the driver’s ball-end design enables angled engagement. This adds complexity and requires compatible tools for proper handling
Conclusions
Angled screw-retained crowns can help achieve better esthetic outcomes by allowing the screw hole to emerge from a better position, avoiding incisal edge or buccal aspect in some cases. Cases where the implant angulation is challenging, angled screw-retained crowns can eliminate the need for complex abutment components. Unlike cement-retained crowns, screw-retained crowns eliminate the risk of residual cement, which can lead to peri-implant complications.
References
- Sailer I, Mühlemann S, Zwahlen M, Hämmerle CHF, Schneider D. Cemented and screw‐retained implant reconstructions: a systematic review of the survival and complication rates. Clin Oral Implants Res. 2012 Oct;23(s6):163–201.
- Priest G. A current perspective on screw‐retained single‐implant restorations: a review of pertinent literatureJ J Esthet Restor Dent. 2017;29:161–171.
- Berroeta E, Zabalegui I, Donovan T, Chee W. Dynamic abutment: a method of redirecting screw access for implant-supported restorations: technical details and a clinical report. J Prosthet Dent. 2015;113:516–519.
- Chen YH, Wu YL, Chen HS, Lin CP, Wu AYJ. Reverse torque value of angulated screw channel abutment before and after cyclic loading: an in vitro study. J Funct Biomater. 2023;14:124.
- Buser D, Chappuis V, Belser UC, Chen S. Implant placement post extraction in esthetic single tooth sites: when immediate, when early, when late? Periodontol 2000. 2017;73:84–102.
- Buser D. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations. Int J Oral Maxillofac Implants. 2004;19 Suppl:43-61.
- Testori T, Weinstein T, Scutellà F, Wang H, Zucchelli G. Implant placement in the esthetic area: criteria for positioning single and multiple implants. Periodontol 2000. 2018;77:176–196.
- Edmondson EK, Trejo PM, Soldatos N, Weltman RL. The ability to screw-retain single implant-supported restorations in the anterior maxilla: a CBCT analysis. J Prosthet Dent. 2022;128:443–449.
- Rella E, De Angelis P, Damis G, D’Addona A, Manicone PF. The application of angulated screw-channels in metal-free, implant-supported restorations: a retrospective survival analysis. Materials (Basel). 2021;14:7006.
- Al‐Omari WM, Shadid R, Abu‐Naba’a L, Masoud BE. Porcelain fracture resistance of screw‐retained, cement‐retained, and screw‐cement‐retained implant‐supported metal ceramic posterior crowns. J Prosthodont. 2010;19:263–73.
- Shadid R, Sadaqa N. A comparison between screw- and cement-retained implant prostheses. a literature review. J Oral Implantol. 2012;38:298–307.
- Dini C, Borges GA, Costa RC, Magno MB, Maia LC, Barão VAR. Peri‐implant and esthetic outcomes of cemented and screw‐retained crowns using zirconia abutments in single implant‐supported restorations — a systematic review and meta‐analysis. Clin Oral Implants Res. 2021;32:1143–158.
- Weber HP, Kim DM, Ng MW, Hwang JW, Fiorellini JP. Peri‐implant soft‐tissue health surrounding cement‐ and screw‐retained implant restorations: a multi‐center, 3‐year prospective study. Clin Oral Implants Res. 2006;17:375–379.
- Bhumpattarachai S, Kan JYK, Goodacre CJ, et al. Effects of cyclic loading on loss of abutment screw torque of angled screw channel single implant crowns on narrow diameter implants. J Prosthet Dent. 2023;130:741:1-741.
From Decisions in Dentistry. January/February 2025;11(1):10-17.
