
 ALEX-MIT/ISTOCK/GETTY IMAGES PLUS
ALEX-MIT/ISTOCK/GETTY IMAGES PLUS
Simplified Denture Duplication for Implant Surgical Guides
This denture duplication technique can simplify in-house fabrication of dental implant surgical guides.
 Mandibular overdentures have become the gold standard treatment option for edentulous patients because they offer superior retention and support, as well as a high degree of patient satisfaction, compared to the traditional mandibular denture.1,2 When planning for implant placement, fabrication of a surgical guide is highly recommended so the fixtures are in an ideal restorative position.3
Mandibular overdentures have become the gold standard treatment option for edentulous patients because they offer superior retention and support, as well as a high degree of patient satisfaction, compared to the traditional mandibular denture.1,2 When planning for implant placement, fabrication of a surgical guide is highly recommended so the fixtures are in an ideal restorative position.3
Multiple surgical guide options are available, ranging from vacuum-formed clear trays to three-dimensionally printed resin guides.3 Another technique is using a duplication of a patient’s existing denture as a template. A simplified technique for duplicating a well-fitted denture in clear acrylic was described by Lindquist et al4 in 1997. In this technique, the dentist can either send the patient’s existing denture to a laboratory for replication (although this means sending the patient home without teeth for a couple of days), or the denture can be duplicated in-house.
This report will present a predictable denture duplication technique that does not require special equipment (such as a duplicating jig), and can be performed by auxiliary personnel in-house.
![FIGURE 2. Two maxillary plastic stock trays without polyvinyl siloxane adhesive.]() Materials and Methods
Materials and Methods

An edentulous patient presented to the advanced education in general dentistry program clinic at the Dental College of Georgia at Augusta University with the chief complaint of “I want my lower denture to stay in place better.” After the clinical team and patient discussed the risks, benefits and alternatives of all treatment options, the patient decided on a two-implant overdenture.
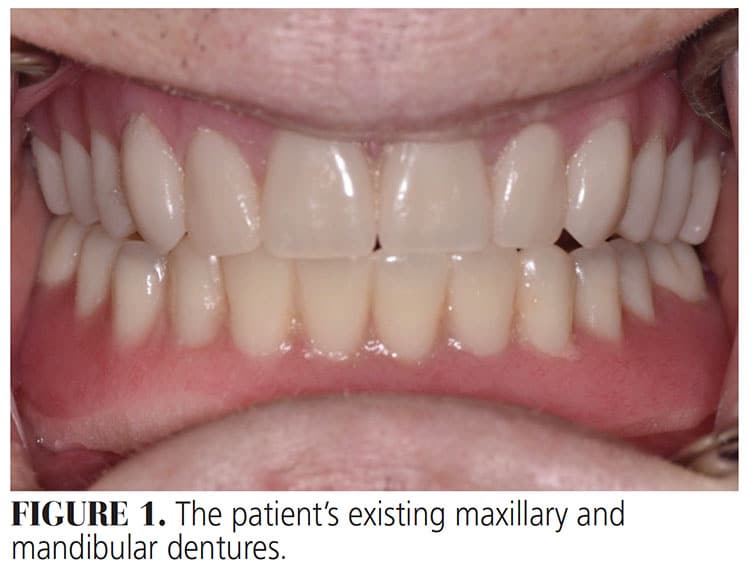
The existing mandibular denture was obtained from the patient and its integrity was visually inspected, followed by an intraoral fit check (Figure 1). In this case, the denture fit was clinically acceptable, so it was determined the existing denture could be duplicated to serve as a radiographic and surgical template for implant placement.
A simple technique using putty material was selected to complete the duplication process. First, in order to contain the impression material, two stock, plastic maxillary impression trays were utilized (Figure 2). There is no need to coat the trays with polyvinyl siloxane (PVS) tray adhesive to complete the duplication. A PVS putty base and catalyst were hand mixed and the first maxillary impression tray was filled with the mixture.
The mandibular denture was lightly coated in petroleum jelly, pressed into the impression material (with the cameo surface of the denture contacting the putty), and left undisturbed until set. Once set, three triangular notches were cut into the borders of the putty using a Bard-Parker surgical blade. These notches help ensure the clinician will be able to accurately articulate the two trays together at a later step to avoid errors in duplication. The mandibular denture is left in the tray containing the set putty, and, before continuing, the intaglio surface of the denture, as well as the set putty impression material, were coated with petroleum jelly. This helps prevent the two putties from sticking together, and also eases separation.
Next, a new mixture of PVS putty base and catalyst was placed inside the mandibular denture (intaglio) and molded into the borders and notches. In order to spread and compress the PVS into the intaglio surface of the denture, a second maxillary tray was pressed into the mixture. The putty was allowed to set, the two trays were separated, and the denture was removed from the stock tray, cleaned, and returned to the patient.
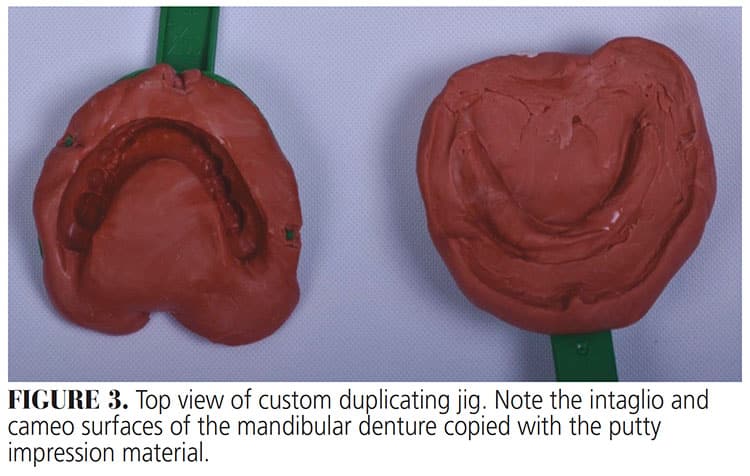
 Once the denture has been duplicated with this technique, the operator will have a copy of the ridge (intaglio surface) on one maxillary tray, and a copy of the denture (cameo surface) on the other tray (Figure 3). The cameo surface mold was filled with clear, self-cure acrylic and the intaglio surface mold was placed on top. Clinicians should be sure to line up the previously marked notches. A rubber band can be used to hold both pieces together (Figure 4). The mated trays were placed in a pressure pot with hot to boiling water at 20 PSI for 20 minutes to create a porosity-free, clear duplicate denture/surgical guide. Next, the template was trimmed, and the provider verified there were no sharp edges before polishing using a wet rag wheel. Once verified to be free of imperfections, four small disc-shape radiopaque composites were placed on the facial surface of teeth #22, 23, 26 and 27 of the duplicated denture and inserted into the patient’s mouth to obtain a cone beam computed tomography (CBCT) scan.
Once the denture has been duplicated with this technique, the operator will have a copy of the ridge (intaglio surface) on one maxillary tray, and a copy of the denture (cameo surface) on the other tray (Figure 3). The cameo surface mold was filled with clear, self-cure acrylic and the intaglio surface mold was placed on top. Clinicians should be sure to line up the previously marked notches. A rubber band can be used to hold both pieces together (Figure 4). The mated trays were placed in a pressure pot with hot to boiling water at 20 PSI for 20 minutes to create a porosity-free, clear duplicate denture/surgical guide. Next, the template was trimmed, and the provider verified there were no sharp edges before polishing using a wet rag wheel. Once verified to be free of imperfections, four small disc-shape radiopaque composites were placed on the facial surface of teeth #22, 23, 26 and 27 of the duplicated denture and inserted into the patient’s mouth to obtain a cone beam computed tomography (CBCT) scan.
Discussion
One of the benefits of this technique is it does not require a denture duplicating jig. When using the jig, the recommended impression material is irreversible hydrocolloid — which has been reported to have low dimensional stability, which could affect the final product fit.5,6 On the other hand, if the operator uses PVS putty in combination with a traditional jig, it will require a considerable amount to fill the entire jig. In addition, it creates challenges when cleaning the jig for a new duplication. In contrast, plastic stock maxillary trays are commonly found in every general dentistry practice, and the amount of putty required to fill them is normally two to three scoops. Once used, there is no need for cleanup because the trays and material are disposable. A disadvantage of this approach to denture duplication is that it can be technique sensitive, and if certain steps are not followed precisely, duplication will not be successful.
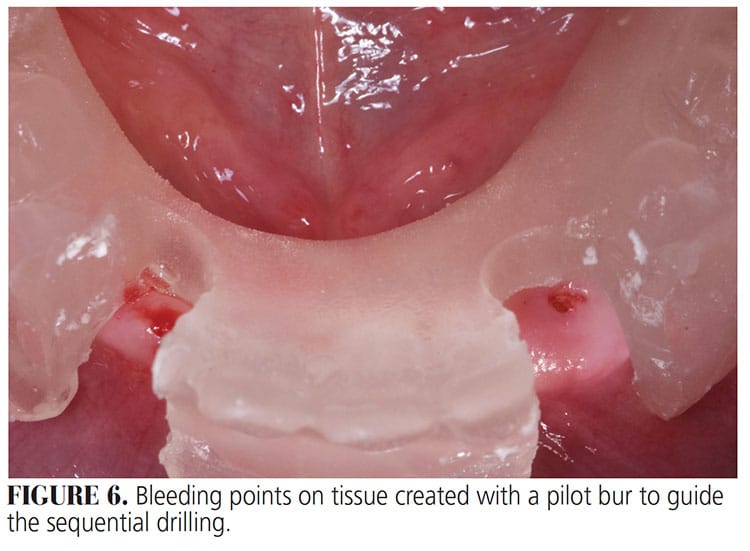
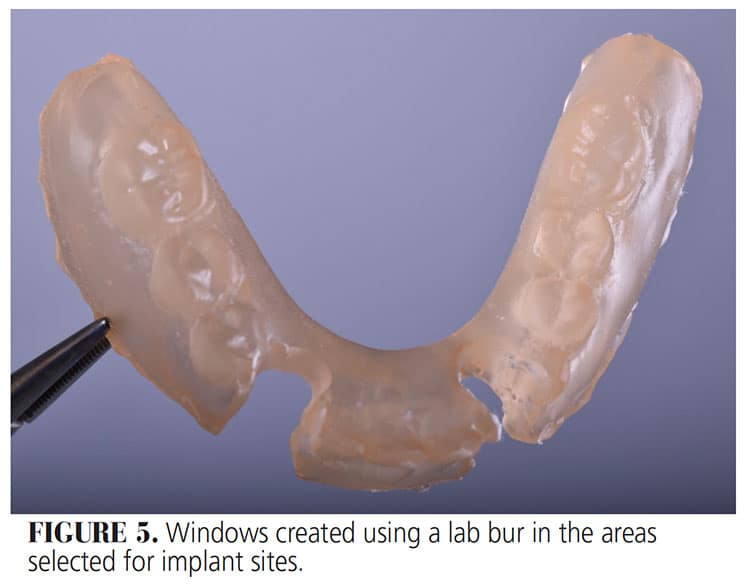
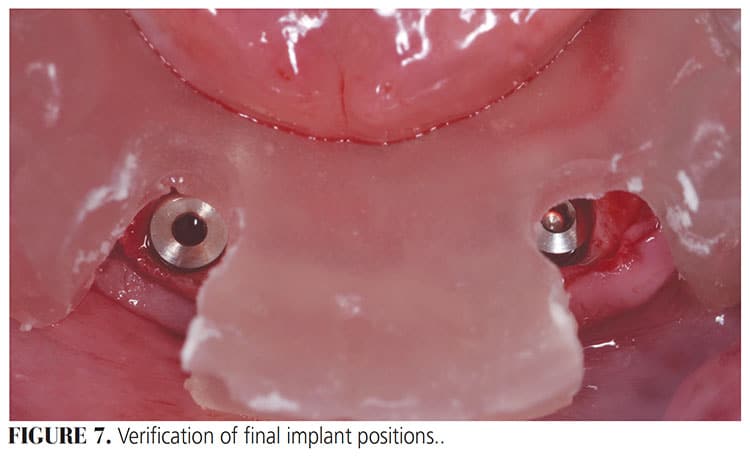
After duplication, the denture is originally used as a radiographic template incorporating composite discs. The composite discs are radiopaque and can easily be seen on the CBCT, which provides a positional reference point on the edentulous arch. In this case, once the CBCT was analyzed, sites #23 and 27 were chosen for implant placement. This was followed by creating two windows in the duplicated denture using an acrylic bur in the selected areas corresponding to teeth #23 and #27 (Figure 5). During the surgical procedure, the duplicated denture becomes a surgical template. With the template in place, bleeding points are obtained using a pilot drill prior to tissue reflection (Figure 6), followed by a full thickness flap and sequential drilling to fit two 3.7 x 10-mm tapered screw vent implants. Once cover screws are placed, the surgical template (i.e., duplicate denture) is seated to verify final implant position (Figure 7).
Conclusion
Radiographic and surgical templates are important aids during implant planning and placement. Regardless of the fabrication method, they need to fit properly in the patient’s mouth so implant accuracy errors are minimized. The advantages of the technique presented in this report is that it minimizes polymerization deformation, and reduces the cost of fabrication compared to using a conventional duplicating jig and alginate impression material, or outsourcing to a commercial lab. This denture duplication technique can be performed in-house, further saving time and cost when fabricating surgical guides. With more accurate implant planning and placement, dentists can produce better restorative results for patients.
Key Takeaways
- Compared to the traditional mandibular denture, mandibular overdentures have become the gold standard treatment option for edentulous patients because they offer superior retention and support, as well as a high degree of patient satisfaction.
- This article describes a technique for using a duplication of a patient’s existing denture as a template for fabricating a surgical guide for dental implant placement.
- This denture duplication technique does not require special equipment (such as a duplicating jig), and can be performed by auxiliary personnel in-house.
- A disadvantage of this approach is that it can be technique sensitive.
- The technique uses polyvinyl siloxane putty material and two stock, plastic maxillary impression trays — items commonly found in general dentistry practices.
- Once the denture has been duplicated with this technique, the operator will have a copy of the ridge (intaglio surface) on one maxillary tray, and a copy of the denture (cameo surface) on the other tray.
- Utilizing this approach will minimize polymerization deformation and reduce fabrication costs compared to using a conventional duplicating jig and alginate impression material, or outsourcing to a commercial lab.
References
- Melescanu Imre M, Marin M, Preoteasa E, Tancu AM, Preoteasa CT. Two implant overdenture — the first alternative treatment for patients with complete edentulous mandible. J Med Life. 2011;4:207–209.
- Feine JS, Carlsson GE, Awad MA, et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Gerodontology. 2002;19:3–4.
- D’souza KM, Aras MA. Types of implant surgical guides in dentistry: a review. J Oral Implantol. 2012:38:643–652.
- Lindquist TJ, Narhi TO, Ettinger RL. Denture duplication technique with alternative materials. J Prosthet Dent. 1997:77:97–98.
- Kusugal P, Chourasiya RS, Ruttonji Z, Astagi P, Kumar Nayak A, Patil A. Surface detail reproduction and dimensional stability of contemporary irreversible hydrocolloid alternatives after immediate and delayed pouring. Contemp Clin Dent. 2018:9:20–25.
- Sedda M, Casarotto A, Raustia A, Borracchini A. Effect of storage time on the accuracy of casts made from different irreversible hydrocolloids. J Contemp Dent Pract. 2008;9:59–66.
From Decisions in Dentistry. December 2020;6(11): 12-14.
