
 YACOBCHUK/ISTOCK/GETTY IMAGES PLUS
YACOBCHUK/ISTOCK/GETTY IMAGES PLUS
Setting Risk-Based Periodontal Recare Intervals
Careful assessment of these factors will help dental teams establish appropriate, risk-based recare intervals for periodontal maintenance.
PURCHASE COURSE
This course was published in the February 2020 issue and expires February 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the February 2020 issue and expires February 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Define the central tenets of using risk-based recare intervals, and their role in periodontal maintenance.
- Discuss the typical components of a maintenance visit, and risk factors for periodontal disease progression.
- Describe the dental team’s role in determining risk-based recare intervals.
In 2018, the American Academy of Periodontology (AAP) and European Federation of Periodontology published a new classification system for periodontal health and disease, changing the way dental professionals consider the clinical parameters of a patient’s periodontal status. Caton et al1,2 published the comprehensive criteria in both the Journal of Periodontology and Journal of Clinical Periodontology. (A thorough summary by Katsaros3 also appears in the October 2018 issue of Decisions in Dentistry, available at decisionsindentistry.com.) A major component of the new classification system is the use of staging and grading to focus on disease complexity and progression based on an individual’s protective behaviors and risk factors.1,2 Implementation of the new system offers clinicians an opportunity to educate patients about their role in maintaining or improving oral health. One way clinicians can integrate staging and grading into educational efforts is by providing risk-based assessments — which, in turn, will help determine an individual’s periodontal maintenance recare interval.
The most important function of risk-based assessment is tying that information back into the clinical determination of the treatment plan and recare interval.4,5 Once risk factors have been identified, the dental team and patient can work together to modify detrimental behaviors and conditions to improve treatment outcomes.5 A careful determination of risk factors changes the focus of care to arresting the disease process, rather than repairing the outcomes of disease destruction.6 Oral health professionals can use the completed risk assessment as a means of opening communication with patients regarding how their behaviors affect oral health, and the potential positive or negative outcomes based on how they incorporate recommended modifications.6,7 When patients understand their role in maintaining or improving oral health, they are more likely to accept recommendations and treatment, and comply with recare intervals, as determined by individual risk and needs. Risk-based recare intervals (RBRIs) can help clinicians establish a link between completed clinical assessments and proposed treatment plans.7
PERIODONTAL MAINTENANCE
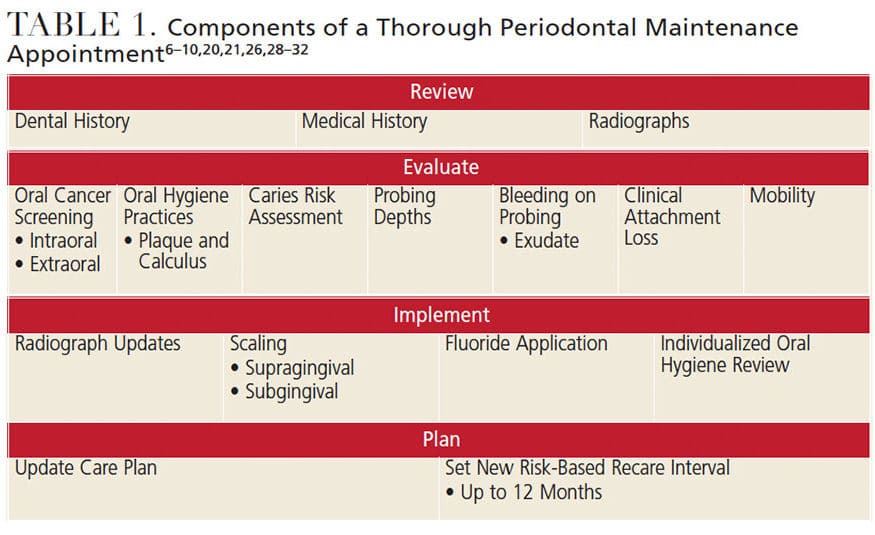
The AAP describes periodontal maintenance as the treatment provided to individuals after the completion of initial (nonsurgical) periodontal therapy, with the intention of preventing further disease progression and maintaining the health of the periodontium.8,9 The purpose of a rigorous maintenance schedule is to allow time for tissues to heal after initial therapy, followed by appropriate support to preserve the treatment outcomes — without relapse to a diseased state.10 A typical periodontal maintenance appointment includes a review of medical and dental histories, clinical assessment, scaling areas of new deposits, and other therapies, as determined by the dental team (Table 1).8
Because periodontal diseases can be treated, but not completely eradicated, periodontal maintenance intervals are often set at three to four months for the life of the affected dentition, or while the patient is at risk of losing more teeth from compromised periodontium due to disease (periodontitis stage III and IV). Yet perhaps an opportunity is being missed for patient education and investment by using the same recare interval for all individuals.1,2,8,11 However, with evidence showing many patients have poor compliance with routine periodontal maintenance, and no evidence demonstrating the same interval is beneficial for all individuals, risk-based treatment approaches are clinically appropriate.9,12,13
RISK ASSESSMENT
Risk assessment is the process of evaluating clinical, behavioral, genetic and environmental factors to determine the overall protective or destructive influence on a patient’s oral health.14,15 These individual factors can impact disease onset, presentation and rate of progression.14 For periodontal diseases, common factors include:
- Clinical findings, such as bleeding on probing, periodontal probing depth and clinical attachment loss
- Response to past therapies
- Behavioral factors, such as oral hygiene practices, smoking and nutrition
- Environmental factors, including fluoride intake and socioeconomic status (access to dental insurance can impact an individual’s ability to comply with maintenance appointments)10,14
A wide array of additional factors contributes to the development of periodontal disease that can be evaluated during routine appointments. Clinicians should also consider possible genetic factors when periodontitis does not resolve posttreatment (Table 2).6,10,15,16 As behaviors and clinical findings can change over time, risk assessments should be completed for every periodontal treatment plan and included in all comprehensive and periodic evaluations.14
A host of computer programs can help in determining a patient’s overall risk, based on multidimensional analyses of independent risk factors.4 Although not the focus of this article, several of these programs have been independently tested and validated in clinical studies.4,17 When determining the need for an adjunct risk assessment tool, or deciding which program to use, the dental team should consider if the tool has been independently validated, is easy to use and understand, includes sufficient risk factors in the analysis, is evidence-based, and provides accurate classification and prognosis until the next appointment.18,19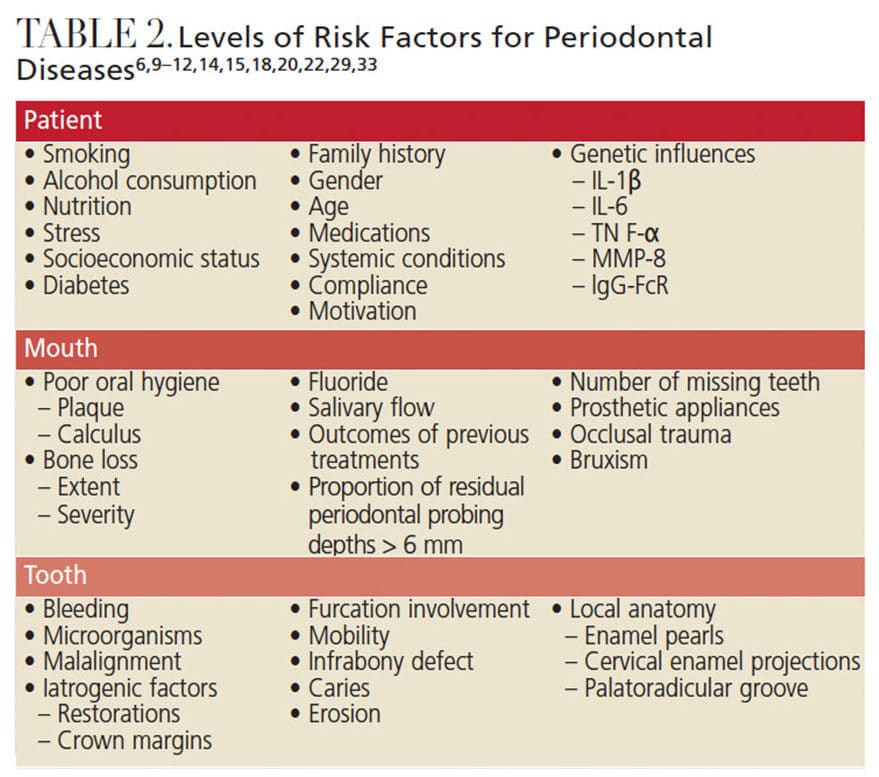
RISK-BASED RECARE INTERVALS
Once risk assessment is completed, the next step is to determine the most appropriate recare interval for the patient. Using evidence-based decision-making, clinicians should weigh the impact of risk variables to determine overall risk of disease progression.10 For example, in the new AAP classification system, all individuals begin at a presumed Grade B, indicating a predicted moderate rate of disease progression. Clinicians then use risk analysis and clinical evidence to determine if the patient should be classified as Grade A or Grade C.1–3 Individuals with Grade B may be placed on a typical three- to four-month recare interval.1–3,9,10
Patients who have responded well to previous treatment, comply with self-care, and have no additional systemic or behavioral risk factors may have their classification adjusted to Grade A, which suggests longer intervals of six to 12 months between periodontal maintenance appointments.1–3,9,10 Individuals who show poor response to treatment or have increased risk due to systemic disease or smoking could be modified to a Grade C, and seen on a bimonthly basis until periodontal stability has been achieved and the risk of disease progression is deemed moderate or slow.1–3,9,10 Discussing a patient’s grading classification as a means of scheduling intervals for future appointments affords dental teams another opportunity to reinforce the impact of behavior and self-care habits, empowering patients to take a more active role in their oral health.1–3,7 The 2005 National Institute for Health and Care Excellence Guidelines recommend preventive maintenance recare intervals of anywhere between three and 24 months for adults.20 For periodontal maintenance appointments, studies have shown recare intervals as long as once per year can still be beneficial in maintaining periodontal health.21,22
Most studies on recare intervals evaluate patient outcomes based on attending three-month recare intervals (complete compliers versus erratic compliers), but have not investigated the effect of various recare intervals on periodontal health.23 Currently, a four-year, multicenter, parallel randomized control trial with blinded outcomes assessment is underway in the United Kingdom.24 This study is evaluating the oral health and quality of life outcomes of patients assigned to preventive appointments at six-month, 24-month, or variable risk-based intervals, as well as the effect of such intervals on provider workload and health care costs.
A central tenet of the RBRI is patient education about how and why a specific interval was set. Clinicians can go through the patient’s risk assessment and point out areas where the individual is doing well or areas that need improvement, and elaborate on how these could affect future recare intervals.10 Patient compliance significantly impacts the success of treatment and oral health maintenance. By using the RBRI as a concrete example of how the patient’s past behavior impacts future treatment, dental teams can reinforce the need for improved performance in self-care and compliance with recare appointments.10,20
As risk factors can be modified, RBRIs are fluid. A patient who is currently on a three-month recare may only need to be seen twice a year if his or her oral hygiene improves and attachment levels remain stable. If the patient relapses in self-care and bleeding on probing increases, the recare interval may need to be shortened to every four months.10 Using risk factors to schedule appointments has been successfully tested in various dental settings globally.10,13,25–27
TEAM-BASED CARE
The periodontal maintenance team includes office staff, dental assistants, dental hygienists, dentists and periodontists. For proper patient-centered care, all team members should work together in collaboration with the patient to determine effective treatment strategies and scheduling options. While dentists and periodontists are responsible for advanced periodontal treatment options (e.g., surgical interventions), dental hygienists are often at the forefront of patient care, performing many of the assessments, initial nonsurgical periodontal therapies, and maintenance after active periodontal therapy has been completed.28
As personalized precision dentistry is the way of the future, oral health professionals should be prepared to conduct risk-based assessments and identify independent risk factors, developing that knowledge into implementable therapeutic care tailored to each individual. Through adequate assessment and documentation of past and current risk factors, along with previous treatment strategies and outcomes, the care team can determine the most appropriate treatment plan, including the most effective RBRI for periodontal maintenance.
CONCLUSION
With an increased focus on disease risk and no evidence that a single recare interval is beneficial for all individuals, clinicians are encouraged to implement formal risk-based assessment into clinical appointments — including setting RBRIs for periodontal maintenance.13
Periodontal risk assessment should include a thorough evaluation of patient behaviors, systemic conditions and environmental factors, as well as risk factors at the tooth, mouth and patient level to determine the risk of disease progression in individual sites and the dentition overall. Risk factors are modifiable and should be evaluated at each appointment to ensure timely detection of disease and implementation of treatment strategies and patient education designed to improve oral health.10
By establishing patient-specific RBRIs, dental teams can help patients increase their understanding and compliance with self-care and professional treatment recommendations, and thus improve and maintain periodontal health.
REFERENCES
- Caton JG, Armitage G, Berglundh T, et al. A new classification scheme for periodontal and peri-implant diseases and conditions — Introduction and key changes from the 1999 classification. J Periodontol. 2018;89(Suppl 1):S1–S8.
- Caton JG, Armitage G, Berglundh T, et al. A new classification scheme for periodontal and peri-implant diseases and conditions — Introduction and key changes from the 1999 classification. J Clin Periodontol. 2018;45(Suppl 20):S1–S8.
- Katsoros T. Overview of the new peri-implant and periodontal disease classification system. Decisions in Dentistry. 2018;4(10):25–30.
- Lang NP, Suvan JE, Tonetti MS. Risk factor assessment tools for the prevention of periodontitis progression a systematic review. J Clin Periodontol. 2015;42(Suppl 16):S59–S70.
- Ramseier CA. Potential impact of subject-based risk factor control on periodontitis. J Clin Periodontol. 2005;32(Suppl 6):283–290.
- Francisco EM, Johnson TL, Freudenthal JJ, Louis G. Dental hygienists’ knowledge, attitudes and practice behaviors regarding caries risk assessment and management. J Dent Hyg. 2013;87:353–361.
- Gurenlian JR, Swigart DJ. Dental hygiene diagnosis. Dimensions of Dental Hygiene. 2018;16(12):36–39.
- Cohen RE, Research, Science and Therapy Committee, American Academy of Periodontology. Position paper: periodontal maintenance. J Periodontol. 2003;74:1395–1401.
- Ramseier CA, Nydegger M, Walter C, et al. Time between recall visits and residual probing depths predict long-term stability in patients enrolled in supportive periodontal therapy. J Clin Periodontol. 2019;46:218–230.
- Darcey J, Ashley M. See you in three months! The rationale for the three monthly periodontal recall interval: a risk-based approach. Br Dent J. 2011;211:379–385.
- Echeverria JJ, Echeverria A, Caffesse RG. Adherence to supportive periodontal treatment. Periodontol 2000. 2019;79:200–209.
- Lee CT, Huang HY, Sun TC, Karimbux N. Impact of patient compliance on tooth loss during supportive periodontal therapy: a systematic review and meta-analysis. J Dent Res. 2015;94:777–786.
- Patel S, Bay RC, Glick M. A systematic review of dental recall intervals and incidence of dental caries. J Am Dent Assoc. 2010;141:527–539.
- American Academy of Periodontology. American Academy of Periodontology statement on risk assessment. J Periodontol. 2008;79:202.
- Rudick CP, Lang MS, Miyamoto T. Understanding the pathophysiology behind chairside diagnostics and genetic testing for IL-1 and IL-6. Oral Dis. 2019;25:1879–1885.
- Hodges KO. Evaluate disease potential. Dimensions of Dental Hygiene. 2015;13(6):24–26.
- Mullins JM, Even JB, White JM. Periodontal management by risk assessment: a pragmatic approach. J Evid Based Dent Pract. 2016;16(Suppl):91–98.
- McGowan T, McGowan K, Ivanovski S. A novel evidence-based periodontal prognosis model. J Evid Based Dent Pract. 2017;17:350–360.
- Brocklehurst PR, Ashley JR, Tickle M. Patient assessment in general dental practice — risk assessment or clinical monitoring? Br Dent J. 2011;210:351–354.
- Bader J. Risk-based recall intervals recommended. Evid Based Dent. 2005;6:2–4.
- Rosén B, Olavi G, Badersten A, Rönström A, Söderholm G, Egelberg J. Effect of different frequencies of preventive maintenance treatment on periodontal conditions. 5-year observations in general dentistry patients. J Clin Periodontol. 1999;26:225–233.
- Gay IC, Tran DT, Weltman R, et al. Role of supportive maintenance therapy on implant survival: a university-based 17 years retrospective analysis. Int J Dent Hyg. 2016;14:267–271.
- Farooqi OA, Wehler CJ, Gibson G, Jurasic MM, Jones JA. Appropriate recall interval for periodontal maintenance: a systematic review. J Evid Based Dent Pract. 2015;15:171–181.
- Clarkson JE, Pitts NB, Bonetti D, et al. INTERVAL (investigation of NICE technologies for enabling risk-variable-adjusted-length) dental recalls trial: a multicentre randomised controlled trial investigating the best dental recall interval for optimum, cost-effective maintenance of oral health in dentate adults attending dental primary care. BMC Oral Health. 2018;18:135.
- Bader JD, Shugars DA, Kennedy JE, Hayden WJ, Jr, Baker S. A pilot study of risk-based prevention in private practice. J Am Dent Assoc. 2003;134:1195–1202.
- Jepsen S, Blanco J, Buchalla W, et al. Prevention and control of dental caries and periodontal diseases at individual and population level: consensus report of group 3 of joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J Clin Periodontol. 2017;44(Suppl 18):S85–S93.
- Mettes TG, van der Sanden WJ, Mulder J, Wensing M, Grol RP, Plasschaert AJ. Predictors of recall assignment decisions by general dental practitioners performing routine oral examinations. Eur J Oral Sci. 2006;114:396–402.
- General Dental Council. Scope of practice: dental hygienists. Nature BDJ Team. 2018;5:18072.
- Lang NP, Tonetti MS. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev Dent. 2003;1:7–16.
- Angst PDM, Stadler AF, Oppermann RV, Gomes SC. Microbiological outcomes from different periodontal maintenance interventions: a systematic review. Braz Oral Res. 2017;4:e33.
- Leavy PG, Robertson DP. Periodontal maintenance following active specialist treatment: Should patients stay put or return to primary dental care for continuing care? A comparison of outcomes based on the literature. Int J Dent Hyg. 2018;16:68–77.
- Renvert S, Persson GR. Supportive periodontal therapy. Periodontol 2000. 2004;36:179–195.
- Costa FO, Vieira TR, Cortelli SC, et al. Effect of compliance during periodontal maintenance therapy on levels of bacteria associated with periodontitis: A 6-year prospective study. J Periodontol. 2018;89:519–530.
From Decisions in Dentistry. February 2020;6(2):36—39.

