

Sedation Regulation Changes and Their Impact on Dental Practice
An examination of how regulatory trends in dental anesthesia align with professional guidelines and evidence-based care.
An examination of how regulatory trends in dental anesthesia align with professional guidelines and evidence-based care
Ever since early American dentist Horace Wells demonstrated effective use of nitrous oxide in the 1840s, anesthesiology and procedural sedation have been ingrained within dentistry. Without these modalities, many patients would not be able to receive professional dental care.1 Accordingly, rules and regulations for procedural sedation have been established and updated to guide care delivery, ensure patient safety, and maintain adequate access to anesthetic care during dental treatment. Nationally, governance and decision-making regarding dental sedation regulations are often varied and influenced by local or regional systems of education and/or care.2
While most dental procedures do not require the use of pharmacological intervention, the benefits of the administration of sedation agents have been well-litigated and its use in dentistry has increased.2–5 Recent analyses have found that 70% of board-certified pediatric dentists and 40% of general dentists provide some form of sedation.6,7 In addition, correlations have been found between improved practice marketability and providing in-office sedation.8 Deaths following sedation during dental care typically receive national attention,9,10 and media coverage of severe adverse events is associated with legislative and regulatory changes in dentistry.2 These changes directly impact the way sedation care is delivered and how providers perform that care. Thus, it is imperative for dental providers to understand how sedation is safely delivered and the regulations that govern its use. This article will explore trends in regulatory changes and the impacts on today’s dental practice.
LEVELS OF SEDATION
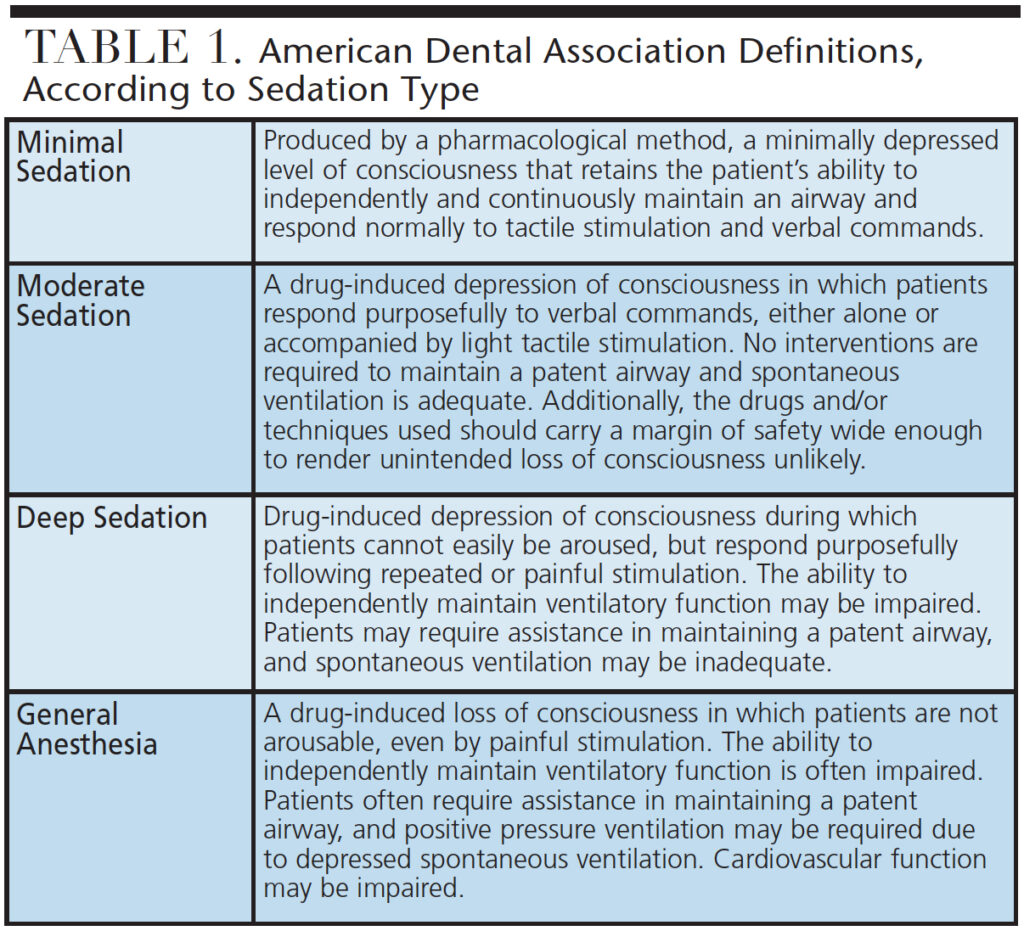
Over the last 15 years, significant changes have occurred in dental sedation and anesthesia regulations and policies. In fact, regulatory changes during the early millennium occurred at two per year, compared to approximately 13 per year since 2006.2,11 One reason for the increased number of regulatory amendments is the change in how the levels of sedation are defined and utilized (Table 1). Prior to inclusion of the terms “minimal,” “moderate” and “deep” sedation, many state practice acts correlated the route of administration (such as intravenous, oral or inhalational) with the depth of sedation. Currently, more than half (27) of U.S. state dental boards (SDBs) exclusively use the new terms (minimal, moderate and deep) to describe requirements for training, site and personnel.2
PEDIATRIC CARE
With a significant disease burden and the need for behavior management, patients in pediatric dental offices are more often reliant on sedation and general anesthesia to complete comprehensive dental care than other populations.2 Younger pediatric patients, individuals with special health care needs, and populations with concomitant medical conditions appear most at risk.2,12 Recently, pediatric dental care with sedation has been implicated in a number of cases involving either morbidity or mortality.12 Subsequently, media coverage showcased the public’s desire for a higher level of transparency and increased patient safety measures. To improve the safety of care, regulatory bodies have focused on enhancing accountability with care administration, and improving prevention of adverse outcomes. Effective patient monitoring plays a central role in achieving these goals because inadequate or ineffective monitoring is frequently a root cause when adverse events or complications occur during pediatric sedation.2,13,14
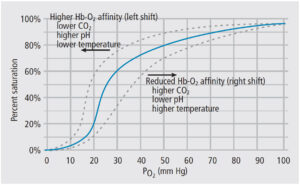
Although monitoring guidelines for children are similar to those for adults, children differ in many physiological characteristics and require a high level of provider awareness and observation. For instance, children have a metabolic oxygen demand that is nearly 60% greater than adults.2 Thus, hypoxemia can develop rapidly and impair necessary organ perfusion. Adequate oxygenation relies not only on adequate ventilation, but also on the oxygen content of the inhaled gas and perfusion of alveoli. As seen in Figure 1, the oxygen-hemoglobin disassociation curve provides context for the relationship between hemoglobin saturation and arterial partial pressure. A pulse oximeter is the most common device for measuring oxygenation. Using red and infrared light to measure the partial pressure of oxygen in arterial blood, pulse oximeters process the balance between the wavelengths to provide a hemoglobin saturation percentage. It should be noted the relay of information — from detection at the finger to the statistical report on the monitor — is delayed by 25 to 45 seconds due to data processing.
With a long history of use during general anesthesia, capnography is the process of measuring the concentration of carbon dioxide in exhaled air, and is a useful mechanism to evaluate respirations. As technology has improved and professional guidelines have changed, its application with moderate sedation has increased. Capnography allows for earlier recognition of respiratory compromise than pulse oximetry, as well as easier identification of hyper-/hypocapnia.11,15,16 Given that respiratory events are primary drivers of morbidity and mortality during procedural sedation, and capnography is effective in detecting these adverse events, four professional organizations have added capnography to their respective guidelines on procedural sedation care: The American Society of Anesthesiologists (ASA) added it in 2011, followed in 2016 by the American Dental Association (ADA), American Academy of Pediatrics and American Academy of Pediatric Dentistry (AAPD).2 It is also worth noting that concerns with the dilution of expired air with oxygen and atmospheric air, and alterations in sample readings with patient movement, have been addressed by some dental professionals.2,17,18 An additional device, the precordial stethoscope, enables providers to hear lung sounds that allows for recognition and detection of turbulent airflow or airway obstruction.
TEAM-BASED CARE
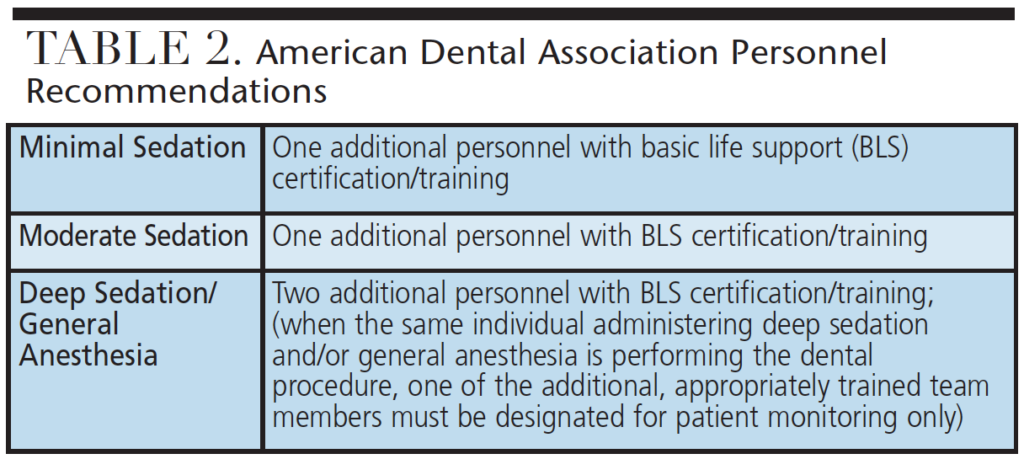
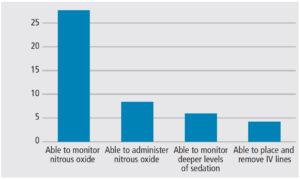
As regulations evolved to include team-based care, the level of sedation being administered dictated the policies for personnel training and scope of practice (Table 2). As seen in Figure 2, dental assistants have a wide range of sedation care tasks and roles, depending on training and office location. This level of variation can create confusing education and training pathways, depending on location of practice.2 Some professional organizations and educational institutions provide dental assistants with a coordinated curriculum for sedation training. Similar to policies for dental assistants, dental hygiene regulations also vary between states. The majority of SDBs (32, in fact) allow the administration of nitrous oxide by dental hygienists. State training requirements range from 2 to 30 hours, with differing requirements for curriculum or course content.2 Recent trends indicate that team-based regulation will be adopted across all SDBs, and the scope of practice for dental assistants and dental hygienists will continue to expand.
In California, the death of 6-year-old Caleb Sears from complications of dental care with an office-based ambulatory anesthesia delivery mode resulted in a policy review and new regulations concerning pediatric dental sedation. An area still being debated relates to the use of the operator-anesthetist model, in which the surgical/dental care provider also administers the anesthetic agents and monitors the patient. While this model has been successfully employed for many years, its use and record of safety are being more thoroughly explored and challenged, especially in pediatric care. The ASA and AAPD recently inserted new language into their guidelines for procedural sedation that recommends the pediatric dental sedation care team have a dedicated, qualified anesthesia provider for moderate or deep sedation, as well as for general anesthesia.2,19
OFFICE INSPECTIONS AND PORTABILITY OF CARE
The last decade has brought increased scrutiny and oversight regarding the physical location of procedural sedation care. The profession enforces and self-regulates the specifications regarding office/facility inspections through peer-reviewed procedures. The most recent data demonstrate that 47 SDBs require some type of site inspection.2 Office inspections are most likely conducted at the site of care. Equipment, safety parameters and site/personnel readiness are evaluated during a live-patient review by designated inspectors. Office/site inspectors are frequently private contractors or subcontractors serving as peer-reviewers for a SDB. Depending on the state, working in certain health care facilities exempts practitioners from needing a portable anesthesia inspection to provide their services. Inspection requirements are site oriented, specific to the level of sedation permitted, and require providers to have each place in which sedation occurs to undergo independent inspection. These inspections are often associated with additional (or duplicate) fees for multiple sites of practice. Office inspection processes for portable care may have impactful fees and result in building and equipment costs that may limit access to care.
Over the last two decades, the regulation of sedation portability has become more restrictive and focused on fixed sites of operation. Very few SDBs (Texas, New Mexico, North Carolina and Massachusetts) have portable or mobile anesthesia regulations and specific permits for providers who perform anesthesia services in other practitioners’ offices. Additional analysis may be warranted to determine the best office inspection practices and protocols, and how regulation may or may not affect access to, and the safety of, needed services.
CONTINUUM OF SAFETY
In 2017, the U.S. Department of Health and Human Services identified the Dental Patient Safety Foundation (DPSF) as a patient safety organization. The DPSF was formed to address the increasing incidence of negative patient safety events in dentistry, and the lack of a mechanism for reporting such incidents.20 The foundation collects reported data on adverse events and compiles the information for public and professional reporting; more information on the DPSF can be found at dentalpatientsafety.org.
Maintaining a continuum of safety requires an understanding of adverse events and solutions designed to reduce or eliminate their occurrence. Mandatory continuing education (CE) has long been used to ensure that practitioners remain up-to-date on best practices and evidence-based protocols for providing safe care. In the 1990s, SDBs began requiring sedation permit holders to obtain anesthesia-specific CE. Today, 29 SDBs require various types of CE and ongoing training to renew sedation permits.2 Additionally, 11 SDBs require non-permitted dentists that employ third-party providers for sedation services to obtain specific hours of CE for license renewal. The objectives of such regulations are to improve the margin of safety and create peer accountability during sedation care.
ADVERTISING AND CONSUMER COMMUNICATION
In a recent ruling, a U.S. District Court in Texas determined that dentists who do not practice one of the nine ADA specialties (anesthesiology is not considered a specialty by the ADA) can advertise as specialists under First Amendment protection. The court directed that dentists with bona fide professional certification can market their services within the dental profession and to consumers.11 Recently, the Fifth Circuit Appellate Court affirmed the lower court’s ruling that the dental specialty advertising restriction promulgated by the Texas Dental Board violated First Amendment rights.21
THE OPIOID CRISIS AND ACCOUNTABILITY
The opioid crisis is a public health emergency, and efforts to address opioid addiction have brought changes that affect dental sedation care. Providers are subject to increased scrutiny and tracking of agents administered, wasted and destroyed. This is beyond patient record documentation. Providers need a separate log for shipping and receiving, patient administration, and traveling with controlled substances (including mileage, location addresses and storage). This also involves any administration of oral agents for sedation care. For multistate practices and providers, the U.S. Drug Enforcement Administration (DEA) states that practitioners who wish to administer or dispense controlled substances in multiple states have the following options regarding a DEA registration: (1) obtain a separate DEA registration in each state where they plan to administer or dispense agents; (2) use a hospital/health care system DEA registration (if care is taking place within the registered confines of the sponsoring system); or (3) transfer an existing DEA registration from one state to another as needed (the DEA will investigate each modification as a new application).2
CONCLUSION
The capacity of anesthesiology extends beyond the operating room to include components of many professions and practice models. While dentistry has maintained a level of safety with sedation care at or better than other areas of health care, the current public and media viewpoint demands improvement in safety margins and a reduction in adverse events.
Health policy regulation is one mechanism to improve outcomes and provide transparency. However, in light of changing legislation and significant variations in dental sedation regulations throughout the United States, dental professionals and health care delivery sites may find it challenging to effectively and efficiently align regulatory compliance and evidence-based care. When it comes to anesthesia and procedural sedation, the key to safe care is to remain abreast of professional guidelines and SDB policies.
KEY TAKEAWAYS
- Regulations for procedural sedation are updated regularly to guide care delivery and ensure patient safety.
- Nationally, governance and decision-making regarding dental sedation regulations are often varied and influenced by state, regional and/or local authorities.2
- Studies suggest that 70% of board-certified pediatric dentists and 40% of general dentists provide some form of sedation.6,7
- Correlations have been found between improved practice marketability and providing in-office sedation.8
- As regulations evolved to include team-based care, the level of sedation being administered dictates the policies for personnel training and scope of practice.
- It is imperative for dental providers to understand how to deliver sedation safely and the regulations that govern its use.
References
- American Dental Association. ADA Policy Statement: The Use of Sedation and General Anesthesia by Dentists. Available at: ada.org/~/media/ADA/Education%20and%20Careers/Files/ADA_Sedation_Policy_Statement.pdf?la=en. Accessed February 20, 2018.
- Boynes SG. Dental Anesthesiology: A Guide to the Rules and Regulations of the United States of America. Ed. 6. Pittsburgh, Penn: No-No Orchard Publishing; 2018.
- Saxen MA, Urman RD, Yepes JF, Gabriel RA, Jones JE. Comparison of anesthesia for dental/oral surgery by office-based dentist anesthesiologists versus operating room-based physician anesthesiologists. Anesth Prog. 2017;64:212–220.
- Griffith SO, Gooch BF, Beltran E, Sutherland JN, Barsley R. Dental services, costs and factors associated with hospitalization for Medicaid-eligible children in Louisiana 1996–1997. J Public Health Dent. 2000;60:21–27.
- Dionne RA, Gordon SM, McCullagh LM, Phero JC. Assessing the need for anesthesia and sedation in the general population. J Am Dent Assoc. 1998;129:167–173.
- Olabi NF, Jones JE, Saxen MA, et al. The use of office-based sedation and general anesthesia by board certified pediatric dentists in the United States. Anesth Prog. 2012;59:12–17.
- Feck A, Sliverman MD. Success with sedation: a profitability comparison of oral, and IV sedation. Dent Economics. 2009; 99:24–26.
- Jackstein J. The Need and Demand for Anesthesia Services in the United States, 2012. (Doctoral dissertation, The Ohio State University).
- Lee HH, Milgrom P, Starks H, Burke W. Trends in death associated with pediatric dental sedation and general anesthesia. Paediatr Anaesth. 2013;23:741–746.
- Snow K. Children at Risk: Kids and Sedation at the Dental Office. Available at: nbcnews.com/megyn-kelly/video/children-at-risk-kids-and-sedation-at-the-dentist-s-office-989892675520. Accessed February 20, 2018.
- Boynes SG. Considerations for sedation in dentistry. Decisions in Dentstry. 2016;2(5):16–22.
- Nelson TM, Xu Z. Pediatric dental sedation: challenges and opportunities. Clin Cosmet Investig Dent. 2015;7:97–106.
- Sammartino M, Volpe B, Sbaraglia F, Garra r, D’Addessi A. Capnography and the bispectral index–their role in pediatric sedation: a brief review. Int J Pediatr. 2010: 828347.
- Cote CJ, Notterman DA, Kaarl HW, Weinberg JA, McCloskey C. Adverse sedation events in pediatrics: a critical incident analysis of contributing factors. Pediatrics. 2000;105:805–814.
- McCarthy C, Brady P, O’Halloran KD, McCreary C. Tetany during intravenous conscious sedation in dentistry resulting from hyperventilation-induced hypocapnia. Anesth Prog. 2016;63:25–30.
- Parker W, Estrich CG, Abt E, et al. Benefits and harms of capnography during procedures involving moderate sedation: A rapid review and meta-analysis. J Am Dent Assoc. 2018;149:38–50.
- Iwaskaki J, Vann WF Jr, Dilley DC, Anderson JA. An investigation of capnography and pulse oximetry as monitors of pediatric patients sedated for dental treatment. Pediatr Dent. 1989;11:111–117.
- Primosch RE, Buzzi IM, Jerrell G. Monitoring pediatric dental patients with mask capnography. Pediatr Dent. 200;22:120–124.
- Hertzberg L. The latest issues facing the ASA. Available at: csahq.org/news/blog/ detail/csa-online-first/2017/09/11/the-latest-issues-facing-the-asa. Accessed February 20, 2018.
- American Dental Society of Anesthesiology. The Pulse Newsletter 2018. Available at: indd.adobe.com/view/79f6d40e-1c61-4a8a-9157-4cf9f5389d7f. Accessed February 20, 2018.
- American Dental Association. Texas Court Ruling Allows Non-ADA Recognized Specialty Dentists to Advertise as Specialists. Available at: ada.org/en/publications/ada-news/2016-archive/january/texas-court-ruling-allows-non-ada-recognized-specialty-dentists-to-advertise-as-specialists. Accessed February 20, 2018.
Featured image by JODIJACOBSON/E+/GETTY IMAGES PLUS
From Decisions in Dentistry. March 2018;4(3):15-16,18,21.
