

Review of the Efficacy of Immediate Implants
An examination of the current science supporting immediate placement of dental implants.
An examination of the current science supporting immediate placement of dental implants
PURCHASE COURSE
This course was published in the June 2019 issue and expires June 2022. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the June 2019 issue and expires June 2022. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
Immediate implant placement has become a successful method for replacing missing teeth.1 Traditionally, after extraction of a failing tooth or teeth, clinicians waited four to six months before implant placement to allow complete mineralization of bone in the extraction sites. However, bone resorption following tooth extraction can compromise the hard and soft tissue outcomes and favorable implant positioning.2 Additionally, this approach prolongs treatment and increases surgical morbidity.2 In edentulous patients with generalized terminal dentition, delayed implant placement diminishes quality of life, as the patient must wear dentures during the healing period.
In recent decades, improved biological and biomechanical understanding has revolutionized implant dentistry by allowing predictable outcomes with immediate implant placement and immediate loading/function.3 Immediate placement (without immediate loading) reduces treatment time; it also eliminates a second surgery, as well as the need for open flap surgery and possible hard and soft tissue grafting. In addition to these advantages, immediate implant placement and provisionalization in partially edentulous patients (especially in the anterior region) provide esthetic, functional and psychological benefits. Immediate implant placement and loading in patients with terminal dentition has the potential to immediately transform the patient’s quality of life. This can also increase case acceptance.3–5
Although the concept of immediate placement was first proposed by Schulte and Heimke6 in 1976, Lazzara7 was the first to report immediate implant placement in an extraction socket in humans in 1989. It is important to understand immediate implant placement is only a temporal description. In addition, the procedure should be distinguished as: (1) immediate implant placement into alveolar bone proper, as done in partially edentulous arches; and (2) immediate implant placement mostly into basal bone (after resection of the extraction socket), as usually done in terminal dentition patients being treated with removable overdentures or complete-arch fixed implant-supported prostheses.

Immediate Implant Placement Into Alveolar Bone Proper: Immediate implant placement into alveolar bone proper (e.g., extraction sockets) is typically associated with partially edentulous spaces in which there is adequate bone height, good soft tissue volume and adequate prosthetic space. The goal is to replace a missing tooth or teeth to mimic contralateral teeth, and use existing hard and soft tissue to support the overall esthetic restoration. However, not all extraction sites are suitable for immediate implant placement in partially edentulous patients. Elian et al8 classified anterior extraction sockets indicated for immediate implant placement into three types, based on the presence or absence of buccal hard and soft tissue:
- Type I Socket: Adequate buccal plate of bone, along with adequate soft tissue and no recession (Figure 1)
- Type II Socket: Absence of adequate buccal plate of bone, but adequate soft tissue and no recession (Figure 2)
- Type III Socket: Absence of adequate buccal plate of bone and absence of adequate soft tissue, but presence of recession (Figure 3)
Elian et al8 noted only Type I extraction sockets should be considered for immediate implant placement. Type II and Type III sockets require regenerative procedures involving hard and soft tissues, which should be done in a staged approach; therefore they are not suitable for immediate placement. The authors also cautioned that a Type II socket would lend itself to being misdiagnosed as favorable by an inexperienced clinician due to the presence of adequate soft tissue, but the inadequate buccal plate of bone would result in extremely apical implant placement and catastrophic esthetic failure.8
It is essential that extraction of teeth indicated for immediate implant placement be performed in an atraumatic manner, which entails flapless extraction and careful preservation of intact buccal plate, as well as facial and interproximal gingiva.9 A systematic review of 32 randomized controlled clinical trials showed that flapless extractions resulted in a mean loss of buccal-lingual width of 2.7 mm, and a 1.7 mm mean loss of height. This is in sharp contrast to data related to open flap extractions that resulted in an average loss of 4 mm in width and height.9 This is mainly because 90% of the blood supply to the buccal plate is provided by the periodontal ligament, which is lost once the tooth is extracted. The remaining blood supply to the buccal plate primarily arises from the overlying periosteum, which is left intact in flapless extractions.9

As noted by Rojas-Vizcaya,10 many authors have suggested immediate implant placement in extraction sockets should follow the 3A-2B rule. This proposes that implants be placed at least 3 mm apical to the existing gingival margin in Type I sockets without any gingival recession, and 2 mm palatal to the buccal bone in Type I sockets where there is an intact buccal plate (Figure 4 and Figure 5). This not only ensures a thicker volume of hard and soft tissues around the facial aspect of the implant, it also allows restoration with a screw-retained prosthesis for the provisional and definitive restorations.10

implant placement is contraindicated. This is a Type III socket and contraindicated for immediate implant placement.
It is recommended the space between the implant and buccal plate of bone (called “jumping distance”) be filled with a bone graft material with a low substitution rate, such as a xenograft or allograft.11 Tarnow et al11 compared four groups of patients to study the change in horizontal ridge dimension associated with immediate implant placement after flapless extractions. In Group 1, patients did not receive a bone graft or provisional restoration; Group 2 patients received a provisional but no bone graft; Group 3 patients received a bone graft but no provisional; and Group 4 patients received both a bone graft and provisional restoration. The authors report that patients in whom the extraction socket received bone grafting in combination with a custom healing abutment or a provisional restoration had the least change in horizontal ridge dimension.
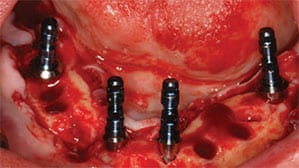
Immediate Implant Placement Into Mostly Basal Bone: Immediate implant placement mostly into basal bone is typically associated with patients with terminal dentition in which there is inadequate hard and soft tissue volume. The goal is to replace all teeth with either overdentures or a full-arch fixed implant-supported prosthesis, where prosthetic gingiva will compensate for the loss of hard and soft tissue volume.12 To ensure adequate prosthetic space for the chosen prosthetic design, resection of some or all of the alveolar bone proper is necessary (Figure 6). This not only allows adequate strength for the biomaterial and prosthetic components, it also provides sufficient space for the gingival prosthesis and an esthetic emergence profile. Biologically, this will lead to placement of implants mostly into basal bone; thus, the biological aspects of healing around immediate implant placement into extraction sockets do not completely apply. Implant position and placement is not governed by the 3A-2B rule, but is purely dictated by biomechanical aspects of treatment, such as implant distribution, anterior-posterior spread and cantilever lengths. Furthermore, it is known that basal bone is cortical in nature, allows good primary stability, and undergoes less resorption.13 Therefore, it is important to recognize that in single implant sites survival outcomes for implants placed mostly into basal bone are distinct from survival outcomes for implants placed into alveolar bone proper.

apical to the existing gingival margin.
Immediate Implant Placement With Immediate Loading: Though immediate implants are often described along with immediate loading/immediate function, indiscriminate use of immediate loading should be avoided.3 For single implants in the maxillary anterior — which is one of the most popular regions for immediate implant placement/loading — all the biological advantages of immediate provisionalization can be achieved by using a custom healing abutment (Figure 7). This is especially advantageous in scenarios with questionable primary stability of the implant, deep vertical overlap, unfavorable occlusion, and in patients who brux.
For immediate implants placed in terminal dentition (indicated for full-arch fixed prostheses) where most of the implant is positioned in basal bone, favorable outcomes of up to 97.3% have been reported.14 Achievement of good primary stability is essential, and when one or more of the immediately placed implants fails to achieve adequate primary stability (especially with distal implants), immediate loading is unsafe. Despite splinting all the implants, unfavorable stresses and off-axial loading result in micromotion and subsequent fibrous encapsulation, leading to early implant failure.3 In such scenarios, it is advisable to submerge the implants during the healing period and provide an immediate denture. Placing multiunit abutments or even healing abutments for single-stage healing can cause premature loading of the implants by the overlying complete denture, and may lead to implant failure.

Immediate Implant Placement in the Anterior Region: Achieving optimal dentogingival esthetics is a prime goal in the anterior region, and a number of factors affect the esthetic success of immediate implant placement and provisionalization.5 These include intrinsic (patient dependent) factors, such as gingival biotype, relationship between soft and hard tissues, and sagittal root position in the alveolar bone. Extrinsic (clinician dependent) factors include three-dimensional implant position and angulation, contour of the abutment, and the provisional restoration.
Additionally, implant diameter, length, macrogeometry and microgeometry are important. Providing the clinician selects a suitable patient, the literature shows good scientific evidence supporting immediate implant placement in the maxillary anterior region. Proper selection includes (but is not limited to) a patient having intact buccal plate, absence of acute infection at the extraction site, and availability of bone apical and palatal to the socket to provide primary stability.15 Additional soft tissue augmentation using autogenous connective tissue grafts has been shown to improve the soft tissue outcomes, especially in thin tissue phenotypes.16
A systematic review by Yan et al17 showed that compared with conventional protocols, immediately placed, restored or loaded single-tooth implants in the esthetic area resulted in similar hard and soft tissue changes. In a systematic review of immediately placed single-tooth implants in the esthetic zone, Slagter et al18 showed a 1-year implant survival rate of 97.1%, with minimal dimensional changes in peri-implant soft and hard tissue. Another systematic review reported a 95.6% survival rate for postextraction implants, compared to 99.4% for those placed at healed sites.19 The authors concluded that in the esthetic zone (anterior maxilla), immediate implant placement and restoration has an excellent prognosis.19
A systematic review by Pigozzo et al20 found no significant differences in terms of survival and marginal bone loss at one or three years between early and immediate loading protocols for single implant-supported crowns. The overall survival rates at one and three years for early loading were 97.5% and 97.6%, respectively, whereas it was 97.3% in both intervals for immediate loading.
Immediate Implant Placement in the Posterior Region: Immediate implant placement in the posterior region is a relatively new modality based on its success in other regions. It should be considered from three aspects: (1) maxillary posterior teeth versus mandibular posterior teeth; (2) single-rooted posterior teeth versus multiple-rooted posterior teeth; and (3) premolars versus molars. Each of these variables can affect implant survival outcomes. Immediate implant placement in the mandibular posterior region may pose a challenge if the apices of the socket are in proximity to the inferior alveolar nerve (and potentially not allow apical bone preparation to support primary stability). Additionally, the presence of any lingual concavity in the apical region may pose a high risk of lingual plate perforation.21

Similarly, in many cases the posterior maxilla may increase the challenge due to presence of soft trabecular bone. According to Lekholm and Zarb,22 bone quality in the posterior maxillary region is usually type III or IV and characterized by thin cortical bone and low-density trabecular bone. Furthermore, the maxillary sinus may sometimes be pneumatized, leaving minimal bone for apical stability during immediate implant placement. Therefore, with immediate molar implants, using precise technique for sectioning the roots, along with wide-diameter implants with aggressive macrogeometry, allow the implant to engage the adjacent bony walls, which is crucial to favorable outcomes.
In a long-term follow-up study of 300 immediately placed implants over 11 years, Smith et al23 reported an overall survival rate of 97.3%, similar to previously reported survival in delayed molar implant placement protocols. Ketabi et al24 published a systematic review and meta-analysis of outcomes following immediate molar implant placement in both arches. A total of 768 immediate molar implants were placed in 757 patients. The study showed an implant survival rate of 98%, with no difference between the maxilla and mandible. However, a higher implant failure was found for ultrawide (> 6- to 9-mm) implants compared to wide (4- to 6-mm) implants.
Moraschini and Porto Barboza25 conducted a meta-analysis to compare immediately and conventionally loaded single mandibular posterior implants and found no statistically significant difference between the two with respect to marginal bone loss and implant survival at a follow-up of 31.2 months. While implant survival ranged from 91.7% to 100% for immediately loaded implants, it was 96.6% to 100% for conventionally loaded groups. Amato26 investigated the outcomes of implants in the posterior maxilla and mandible that were functionally loaded immediately after placement, and found a cumulative success rate of 98.6% after 8.6 months follow-up. The author concluded that partially edentulous maxillary and mandibular posterior sites can be confidently treated with immediately loaded implants. By comparison, Atieh et al27 reported a 33% failure rate for immediately placed and restored wide-diameter implants (8 to 9 mm) in molar sites.
There is still a paucity of data regarding immediate implant placement and immediate loading in the maxillary molar region. There are also conflicting data regarding immediate implants in the posterior mandibular area. Hence, while planning for immediate implants in these areas, clinicians should select cases carefully, thoroughly evaluate all parameters, and proceed with caution.
SUMMARY
There is adequate scientific evidence and rationale to support immediate implants in the anterior region whenever preexisting hard and soft tissues are in favorable condition. The decision to immediately load these single implants should be made carefully. When immediate loading is not possible, a custom healing abutment should be used. Adequate scientific evidence also supports immediate implant placement and immediate loading with full-arch fixed prostheses, but there is limited evidence for immediate loading with overdentures. Consequently, careful case selection is needed to ensure successful outcomes.
While emerging evidence supports immediate molar implants, proper case selection remains a key consideration. In addition, clinicians must closely evaluate anatomic structures (such as the inferior alveolar nerve and maxillary sinus) and choose wide-diameter implants with appropriate macrogeometry.

REFERENCES
- Huynh‐Ba G, Oates TW, Williams MA. Immediate loading vs. early/conventional loading of immediately placed implants in partially edentulous patients from the patients’ perspective: a systematic review. Clin Oral Impl Res. 2018;29(Suppl 16):255–269.
- Chrcanovic BR, Martins MD, Wennerberg A. Immediate placement of implants into infected sites: a systematic review. Clin Implant Dent Relat Res. 2015;17(Suppl 1):e1–e16.
- Barndt P, Zhang H, Liu F. Immediate loading: from biology to biomechanics. Report of the Committee on Research in Fixed Prosthodontics of the American Academy of fixed Prosthodontics. J Prosthet Dent. 2015;113:96–107.
- Chen H, Zhang G, Weigl P, Gu X. Immediate placement of dental implants into infected versus noninfected sites in the esthetic zone: a systematic review and meta-analysis. J Prosthet Dent. 2018;120:658–667.
- Kan JY, Rungcharassaeng K, Deflorian M, Weinstein T, Wang HL, Testori T. Immediate implant placement and provisionalization of maxillary anterior single implants. Periodontol 2000. 2018;77:197–212.
- Schulte W, Heimke G. The Tübinger immediate implant. Quintessenz. 1976;27:17–23.
- Lazzara RJ. Immediate implant placement into extraction sites: surgical and restorative advantages. Int J Periodontics Restorative Dent. 1989;9:332–343.
- Elian N, Cho SC, Froum S, Smith RB, Tarnow DP. A simplified socket classification and repair technique. Pract Proced Aesthet Dent. 2007;19:99–104.
- Jambhekar S, Kernen F, Bidra AS. Clinical and histologic outcomes of socket grafting after flapless tooth extraction: a systematic review of randomized controlled clinical trials. J Prosthet Dent. 2015;113:371–382.
- Rojas-Vizcaya F. Biological aspects as a rule for single implant placement. The 3A-2B rule: a clinical report. J Prosthodont. 2013;22:575–580.
- Tarnow DP, Chu SJ, Salama MA, et al. Flapless postextraction socket implant placement in the esthetic zone: part 1. The effect of bone grafting and/or provisional restoration on facial-palatal ridge dimensional change- a retrospective cohort study. Int J Periodontics Restorative Dent. 2014;34;323–331.
- Bidra AS, Agar JR. A classification system of patients for esthetic fixed implant-supported prostheses in the edentulous maxilla. Compend Contin Educ Dent. 2010;31:366–368,370,372–374 passim.
- Garg R, Mishra N, Alexander M, Gupta SK. Implant survival between endo-osseous dental implants in immediate loading, delayed loading, and basal immediate loading dental implants a 3-year follow-up. Ann Maxillofac Surg. 2017;7:237–244.
- Balshi TJ, Wolfinger GJ, Slauch RW, Balshi SF. A retrospective analysis of 800 Brånemark System implants following the All-on-Four™ protocol. J Prosthodont. 2014;23:83–88.
- Morton D, Chen ST, Martin WC, Levine RA, Buser D. Consensus statements and recommended clinical procedures regarding optimizing esthetic outcomes in implant dentistry. Int J Oral Maxillofac Implants. 2014;29 Suppl:216–220.
- Noelken R, Moergel M, Pausch T, Kunkel M, Wagner W. Clinical and esthetic outcome with immediate insertion and provisionalization with or without connective tissue grafting in presence of mucogingival recessions: a retrospective analysis with follow-up between 1 and 8 years. Clin Implant Dent Relat Res. 2018;20:285–293.
- Yan Q, Xiao LQ, Su MY, Mei Y, Shi B. Soft and hard tissue changes following immediate placement or immediate restoration of single-tooth implants in the esthetic zone: a systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2016;31:1327–1340.
- Slagter KW, den Hartog L, Bakker NA, Vissink A, Meijer HJ, Raghoebar GM. Immediate placement of dental implants in the esthetic zone: a systematic review and pooled analysis. J Periodontol. 2014;85:e241–50.
- Del Fabbro M, Ceresoli V, Taschieri S, Ceci C, Testori T. Immediate loading of postextraction implants in the esthetic area: systematic review of the literature. Clin Implant Dent Relat Res. 2015;17:52–70.
- Pigozzo MN, Rebelo da Costa T, Sesma N, Laganá DC. Immediate versus early loading of single dental implants: a systematic review and meta-analysis. J Prosthet Dent. 2018;120:25–34.
- Chrcanovic BR, de Carvalho Machado V, Gjelvold B. Immediate implant placement in the posterior mandible: a cone beam computed tomography study. Quintessence Int. 2016;47:505–514.
- Lekholm U, Zarb GA. Patient selection and preparation. In: Branemark PI, Zarb GA, Albrektsson T, editors. Tissue Integrated Prostheses: Osseointegration in Clinical Dentistry. Chicago: Quintessence Publishing Co; 1985:199–209.
- Smith RB, Tarnow DP, Sarnachiaro G. Immediate placement of dental implants in molar extraction sockets: an 11-year retrospective analysis. Compend Contin Educ Dent. 2019;40:166–170.
- Ketabi M, Deporter D, Atenafu EG. A systematic review of outcomes following immediate molar implant placement based on recently published studies. Clin Implant Dent Relat Res. 2016;18:1084–1094.
- Moraschini V, Porto Barboza E. Immediate versus conventional loaded single implants in the posterior mandible: a meta-analysis of randomized controlled trials. Int J Oral Maxillofac Surg. 2016;45:85–92.
- Amato F. Immediate functional loading of posterior implants placed in partially edentulous patients: a preliminary report on a prospective clinical study. Int J Periodontics Restorative Dent. 2015;35:239–245.
- Atieh MA, Alsabeeha NH, Duncan WJ, et al. Immediate single implant restorations in mandibular molar extraction sockets: a controlled clinical trial. Clin Oral Implants Res. 2013;24:484–496.
From Decisions in Dentistry. June 2019;5(6):36–38,41.

