
 UJIT KANTAKAD/ISTOCK/GETTY IMAGES PLUS
UJIT KANTAKAD/ISTOCK/GETTY IMAGES PLUS
Decision-Making in Restoring an Implant-Supported Overdenture
This case report demonstrates the challenges of a full-mouth rehabilitation with a maxillary implant-supported overdenture and single implant restorations in the mandibular arch.
Implant-supported overdentures can be a successful treatment modality for the fully edentulous maxillary arch to achieve patient satisfaction, reliable function, and implant/prosthesis longevity. These types of restorations reliably address patient’s issues with lack of retention and stability with a conventional removable prosthesis.1,2 Undertaking a multidisciplinary approach is crucial to delivering a predictable and esthetic restorative outcome. This report focuses on the assessment, treatment planning, guided surgery, and final rehabilitation of a 75-year-old patient with a history of previous trauma to the orofacial complex.
The patient’s past dental history included a fixed full-mouth rehabilitation completed 25 years ago that was failing. Due to the patient’s social history and needs, the treatment required a surgically staged approach in order to accommodate the patient’s comfort, function and social demands. An interdisciplinary approach utilizing a sequenced serial extraction protocol at the beginning of therapy, and guided surgery for the final prosthesis, was key to achieving a successful rehabilitation.3,4
Overview: A 75-year-old woman, Mrs. C, was referred for comprehensive oral evaluation and implant evaluation, as she had emergency extractions completed recently. The patient expressed concerns about losing more teeth as part of needed treatment, principally for fear of not being able to confidently smile in public. Mrs. C’s demanding social lifestyle and professional roles frequently involved public speaking.
History of Present Illness: The patient had on and off dental care over the years, especially after a full mouth rehabilitation due to a gunshot injury to the face. She was made aware that comprehensive treatment was needed many years ago, but was afraid of losing the ability to smile. At this time, she was seeking full comprehensive care.

CLINICAL PRESENTATION
The patient’s updated medical history was unremarkable. Initial examination established the presence of localized, plaque-induced gingivitis and recurrent caries underneath existing splinted restorations, as well as multiple missing teeth (Figure 1 and Figure 2). A panorex also showed left mandibular reconstruction from a past sagittal split procedure. Provisionalization of existing ill-fitting restorations was done in order to assess the extent of the caries and determine restorability of the remaining teeth.
An extraoral and temporomandibular joint assessment was conducted. The patient presented with a square-tapering-shaped face and facial asymmetry, with depression on the left side associated with past trauma. Mrs. C did not present with any associated lymphadenopathy or muscle tenderness. Her temporomandibular joints were asymptomatic, with no signs of clicking, crepitus, or tenderness to palpation. Soft-tissue examination of the lips showed dry, friable tissues. Her saliva appeared to be of viscous consistency and normal in quantity. Other intraoral findings were within normal limits.
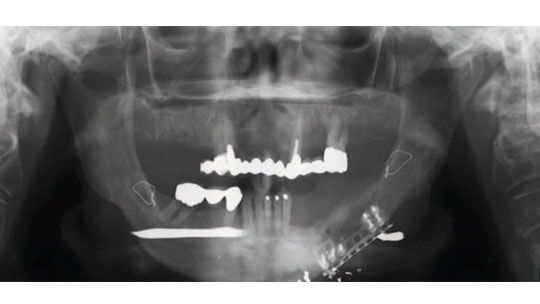
reconstruction, and metal wires at the body of the mandible and ramus.
The patient’s vertical dimensions and vertical dimension of rest were also within normal limits. The maxillary arch was a one-unit splinted fixed dental prosthesis (FDP) supported by four remaining teeth (#5, 6 root tip, 11 and 14). The maxillary ridge presented with a U-shaped form, and the palatal mucosa was within normal resiliency. Existing dentition presented with calculus and associated inflammation. The current fixed prosthesis had an occlusal discrepancy, showing a lower occlusal plane on the left side.
One of the challenges was to transition the maxillary arch from a tooth-supported fixed restoration to an implant-supported FDP (i.e., implant-supported overdenture). As the maxilla presented with a failing dentition, treatment options and patient preferences were considered. A plan to address a fully edentulous maxilla and partially edentulous mandible was developed. Options considered for the maxilla were an implant fixed prosthesis, implant-supported hybrid fixed prosthesis, implant-supported overdenture, and complete denture. For the mandibular arch, single-unit implant restorations versus an interim removable partial denture were considered. Choosing the most adequate treatment involved bone and soft tissue assessment since there was limited opening and tightness of the lip on the left side due to past grafting in the area where the gunshot injury occurred. The unsplinted design with stud abutments for the maxillary overdenture will work favorably, as there was sufficient maxillo-mandibular space for the denture base, teeth and locator attachments. A palateless overdenture will improve patient satisfaction, and after her prior facial reconstruction, the patient wanted the least invasive treatment.

Removal of extensive caries and provisionalization with an interim prosthesis was planned. The FDP at #28 to 30 was sectioned at the pontic region mesially of 29, and 30 was extracted at an emergency visit by her former provider.

TREATMENT RESULTS
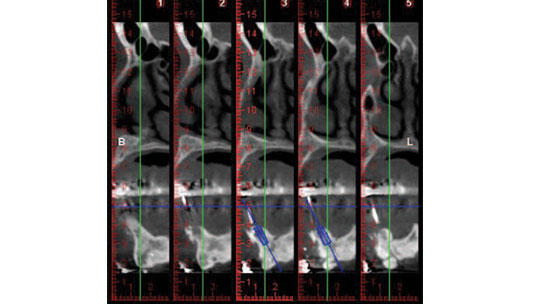
The plan called for extraction of #6 due to extensive caries and delivery of an Essix appliance (Figure 3). A fixed provisional was provided on the remaining teeth #5, 11 and 14.5 This allowed preparation of a maxillary immediate complete denture, and implant placement for single units in the mandibular region.6,7 A cone beam computed tomogram with a radiographic template surgical guide was taken in preparation for the stage approach of implant placement at sites #6, 11, 21, 29 and 30 (Figure 4, Figure 5 and Figure 6).

and 30, respectively.
After full extraction of the remaining maxillary teeth and immediate implant placement at the #6 and 11 regions, an immediate complete denture was delivered. There was sufficient space between the coronoid process and tuberosity area. This will allow for a favorable fabrication of a palateless, implant-supported overdenture with a U-shaped metal framework.8,9

sites #21, 29 and 30.

Implants #21, 29 and 30 were placed in a single-stage approach in the mandibular region. A free vascular graft had been done in the past to reconstruct the left region of the mandible, and this presented a challenge in the number of implants that could be placed. Therefore, on the left side the most posterior implant that could be placed was at the first premolar region (Figure 7).

place.
Teeth #24 and 28 were prepared for provisional crowns, along with implant provisional crowns for 21, 22, 29 and 30. In the maxilla, guided surgery software helped establish parallelism of future implants #3, 5, 12 and 14 with existing sites 6 and 11.10,11 Radiographic markers were placed in the immediate complete denture. Dual-arch scanning was done of the immediate complete denture, and with the patient wearing the denture. Planning for guided surgery was done utilizing specialized software (Figure 8). One additional implant at site #9 was planned as an anterior stop in order to prevent anterior posterior movement and incisive papilla irritation. A guide utilizing titanium sleeves was printed12,13 (Figure 9), and guide stability was achieved with guide pins (Figure 10).


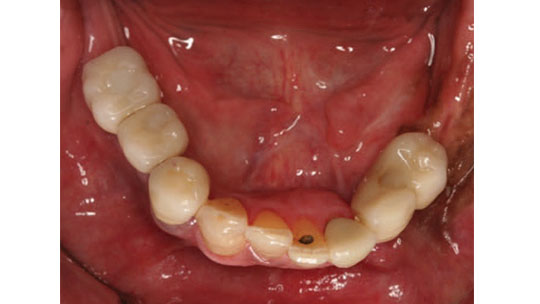
The immediate maxillary denture allowed for completion of the mandibular arch while waiting for healing of the maxillary implants. At the provisional stage, jaw records were taken and verified at time of metal framework try-in for the mandibular region (Figure 11 and Figure 12). Implant restorations were completed for #21, 22, 29 and 30 as porcelain-fused-to-metal appliances (Figure 13). Tooth #21 was a single crown, with a cantilever pontic at the 22 region to provide an occlusal stop for the future maxillary overdenture.


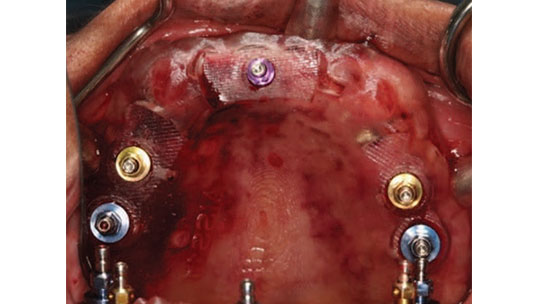
A second-stage surgery was performed for the maxilla, and the immediate maxillary complete denture was adjusted. After six weeks of healing, the patient presented for locator abutment selection. Once locators were obtained, the final impression of the maxillary arch was completed. An impression of the locator abutments and locator housings was made, and the U-shaped metal framework was fabricated14–16 (Figure 14 and Figure 15). The framework was tried in and interocclusal records were made. The teeth were tried in with the framework and records were verified.17 This try-in was sent to the lab for final fabrication (Figure 16). A fit checker was used to check the internal relief for the future acrylic space. Each locator attachment was picked up individually with pattern resin at areas #3, 11 and 14, and the remaining implant locators were picked up (Figure 17). Block-out spacers were utilized to eliminate excess resin material. Oral hygiene instructions were provided, and a follow-up appointment was made to change the male “processing” housings to an appropriate force-retention male housing.18,19 The patient was comfortable and satisfied with the ease of placement and retrieval of the maxillary implant-supported overdenture (Figure 18).
DISCUSSION
The literature indicates that implant-retained maxillary overdentures are a successful treatment modality.20,21 In order to maintain osseointegration, some studies advocate that maxillary implants must be splinted to retain an implant-retained overdenture.15,22 A systematic review sought evidence for establishing criteria for selecting an implant-retained maxillary overdenture.23 Factors such as number/length/distribution of implants, bone quality, available prosthesis space, and maintenance considerations have been suggested as factors or evidence-based criteria. However, there are relatively few evidence-based guidelines; hence, patient-mediated considerations should be used to direct treatment planning (Figure 19).15,24 An implant-supported overdenture significantly improves quality of life and masticatory performance because four to six locator abutments provide optimal anterior posterior support for the prosthesis.2,25



Although an implant-supported overdenture can be a successful treatment modality, the prosthesis may require subsequent adjustment. Proper management and maintenance of peri-implant mucosal health is crucial. Attachments will require periodic evaluations and maintenance to assess the level of retention.26,27
One challenge in this case was the patient’s concern over changes to her appearance. As noted, this prompted staged treatment to ensure the stability of the immediate and interim prostheses. A guided surgery approach to facilitate an implant-supported overdenture allows accurate placement of multiple implants, and reduces surgical operating time.

CONCLUSION
This case presents a successful application of a maxillary implant-supported overdenture with minimal palatal coverage and individual mandibular implant restorations. As previously stated, due to the patient’s history of facial reconstruction and oral rehabilitation, she opted for minimally invasive treatment. Therefore, surgical case planning targeted the existing volume of bone. Ultimately, the staged approach of the treatment plan was able to meet the patient’s work and social demands.
KEY TAKEAWAYS
- Serial extraction and immediate implant placement in a staged approach can help the transition from failing natural dentition to a removable, implant-supported overdenture.
- Possible setbacks in a staged approach include extended treatment time and multiple provisional restorations; however, patient preference and comfort are important considerations.
- A maxillary immediate complete denture serves as a three-dimensional guide, allowing for prosthetically driven implant placement utilizing a guided surgery approach.
Acknowledgement: The authors thank Elias Rivera, DDS, MS, for his help with surgical implant planning, and also acknowledge the contributions of dental assistant Amy Scott.
REFERENCES
- Boven GC, Raghoebar GM, Vissink A, Meijer HJ. Improving masticatory performance, bite force, nutritional state and patient’s satisfaction with implant overdentures: a systematic review of the literature. J Oral Rehabil. 2015;42:220–233.
- Sadowsky SJ, Zitzmann U. Protocols for the maxillary overdenture: a systematic review. Int J Oral Maxillofac Implants. 2016;31(Suppl):s182–s191.
- Cordaro L, Torsello F, Ercoli C, Galluci G. Transition from failing dentition to a fixed implant-supported restoration: a staged approach. Int J Periodontics Restorative Dent. 2007; 27:481–487.
- Cavallaro J Jr. The classification and clinical application of the serial extraction protocol for full-and partial-arch fixed prostheses. Pract Proced Aesthet Dent. 2008;20:377–382.
- Cho SC, Shetty S, Froum S, Elian N, Tarnow D. Fixed and removable provisional options for patients undergoing implant treatment. Compend Cont Educ Dent. 2007;11:604–608.
- Misch CE. Maxillary arch implant considerations: treatment plans for partial and complete edentulous fixed and overdenture Prostheses. In: Dental Implant Prosthetics, 2nd Ed. St. Louis: Mosby; 2015:615–649.
- Gallucci GO, Morton D, Weber HP. Loading protocols for dental implants in edentulous patients. Int J Oral Maxillofac Implants. 2008;24(Suppl):132–146.
- Takahashi T, Gonda T, Mizuno Y, Fujinami Y, Maeda Y. Influence of palatal coverage and implant distribution on implant strain in maxillary implant overdentures. Int J Oral Maxillofac Implants. 2016;31:e136–e142.
- Cavallaro J Jr, Tarnow D. Unsplinted implants retaining maxillary overdentures with partial palatal coverage: report of 5 consecutive cases. Int J Oral Maxillofac Implants. 2007;22:808–814.
- Raghoebar GM, Meijer H, Slot W, Huddleston J, Vissink A. A systematic review of implant-supported overdentures in the edentulous maxilla, compared to the mandible: how many implants? Eur J Oral Implant. 2014;7(Suppl):s1–s11.
- Bover-Ramos F, Viña-Almunia J, Cervera-Ballester J, Peñarrocha-Diago M, García-Mira B. Accuracy of implant placement with computer-guided surgery: a systematic review and meta-analysis comparing cadaver, clinical, and in vitro studies. Int J Oral Maxillofac Implants. 2018;33:101–115.
- Tallarico M, Martinolli M, Kim YJ ,et al. Accuracy of computer-assisted template-based implant placement using two different surgical templates designed with or without metallic sleeves: A randomized controlled trial. Dent J (Basel). 2019;7:41.
- El-Amier N, Elsaih E, Gibreel M, El-Motaiam H. Effect of implant location on palateless complete overdenture retention: an in vitro study. J Oral Maxillofac Res. 2018;9:e3.
- El-Amier NM, Elsaih E, El-Motaiam HA, Al-Shahat MA. Effect of implant location on palateless complete overdenture retention: preliminary study. J Dent Impl. 2015;5:6–11.
- Sadowsky SJ. Treatment considerations for maxillary implant overdentures: a systematic review. J Prosthet Dent. 2007;97:340–348.
- Baker B, Reaney D. Implant supported-overdentures. Available at: https://implantpracticeus.com/ce-articles/implant-supported-overdentures/. Accessed June 15, 2020.
- Shafie HR. Clinical and Laboratory Manual of Implant Overdentures. Iowa: Blackwell; 2007:104–131.
- Kutkut A, Bertoli E, Frazer R, Pinto-Sinai G, Hidalgo R, Studts J. A systematic review of studies comparing conventional complete denture and implant retained overdenture. J Prosthodont Res. 2018;62:1–9.
- Mericske-Stern R, Venetz E, Fahrländer F, Bürgin W. In vivo force measurements on maxillary implants supporting a fixed prosthesis or an overdenture: a pilot study. J Prosthet Dent. 2000;84:535–547.
- Jivra JS, Chee W, Corrado P. Treatment planning of the edentulous maxilla. Br Dent J. 2006;201:261–279.
- Klemetti E. Is there a certain number of implants needed to retain an overdenture? J Oral Rehabil. 2008;35(Suppl 1):80–84.
- Dudley J. Maxillary implant overdentures: current controversies. Australian Dent J. 2013;58:420–423.
- Di Francesco F, De Marco G, Carnevale UA, Lanza M, Lanza A. The number of implants required to support a maxillary overdenture: a systematic review and meta-analysis. J Prosthodont Res. 2019;63:15–24.
- Dimililer G, Kücükkurt S, Cetiner S. Biomechanical effects of implant number and diameter on stress distributions in maxillary implant-supported overdentures. J Prosthet Dent. 2018;119:244–249.
- Zembic A, Tahmaseb A, Wismeijer D. Within-subject comparison of maxillary implant-supported overdentures with and without palatal coverage. Clin Implant Dent Relat Res. 2015;17:570–579.
- Vahidi F, Pinto-Sinai G. Complications associated with implant-retained removable prostheses. Dent Clin N Am. 2015;59:215–226.
- Zarb GA. A panacea for the edentulous predicament. Int J Prosthodont. 2013;26:405–406.
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. July/August 2020;6(7):10-12,14.
