

Original Research: Vertical Root Fracture Repair With a Resin-Ionomer
This case series examines the methods and outcomes associated with treatment of teeth with vertical root fracture where the patients pursued a repair option
This case series examines the methods and outcomes associated with treatment of teeth with vertical root fracture where the patients pursued a repair option

Vertical root fractures (VRF) have been recognized to be either a complete or an incomplete disruption of the tooth structure, and this can include the enamel, dentin and/or pulp along the axis of the tooth, extending to the apex.1 They can involve one or both sides of the root. The presence of a VRF is generally thought to require immediate extraction or repair, but little data is available to suggest that vertical fractures of the root can be repaired for long-term preservation of the tooth. Regrettably, the diagnosis of VRF commonly corresponds to a poor prognosis for the tooth that usually deteriorates, despite restorative care.2–6
Diagnosis of VRF is challenging, and should be based on a complete and thorough analysis of subjective and objective clinical findings. Despite promising new technologies in radiographic imaging, direct visualization by retraction of a full mucoperiosteal flap is still the most effective way to confirm most VRFs, particularly with the help of fiber-optic light or use of a dye.7–10 Several reports have found that affected teeth are most often mandibular molars and maxillary premolars. In one study, up to one-half of the cases studied had root canal therapy prior to detection of the VRF — a suggestion that endodontic treatments may actually increase the risk of VRF. The condition can occur in the presence of a healthy pulp, but Moule and Kahler8 have stated the clinical presentation can include a number of symptoms or findings. These include an extensive history of mild to moderate pain (often associated with local chronic infection), pain while eating, a history of endodontic treatment that has not resolved symptoms, bleeding during canal filling condensation, soft tissue swelling, sinus tract, or a deep, narrow periodontal pocket.
Reported successful therapy for multirooted teeth involved resection of the affected root and splinting the tooth to the two adjacent teeth.11 This procedure can prove effective in preserving the function and integrity of the dental arch, and in preventing eruption of the opposing tooth — but it is considered by many clinicians to be a temporary fix. Others have proposed repair using various dental materials in order to salvage teeth that would otherwise be lost. These include glass-ionomer cement,12 cyanoacrylate cement and 4-META/MMA-TBB resin.13–16
POTENTIAL DRAWBACKS TO REPAIR
Drawbacks to repair of VRF include the need to complete endodontic therapy if any pulpal symptoms exist, and the potential lack of biocompatibility of dental materials (such as bonding agents and cements) when placed under the gingiva and in connective tissue, possibly resulting in a persistent inflammatory process. Many cements and bonding agents trigger acute and chronic inflammatory responses when they are implanted subcutaneously, and the presence and severity of the reactions cited in the literature differ, depending upon the material used.17–19
One restorative material that has demonstrated long-term success when used in similar surgical settings is amalgam, which has been used to obturate the apex of a tooth after endodontic treatment and apicoectomy. Success rates are high: A radiographic success rate of 86% has been reported, along with a clinical success rate of 73.3%,20 as measured by longevity of the treated teeth. Unfortunately, the physical properties of amalgam render it unsuitable for fracture repair because of its weak response to torqueing forces experienced along the root during mastication.
Newer dental materials with resin components, on the other hand, have greater ability to resist torque and tensional forces. The potential downside is they are also more likely to trigger inflammatory reactions, and may serve as a matrix for microbial populations when used in conditions of deep periodontal pocket exposure.2 Several papers have proposed the use of resin-ionomer and hybrid-ionomer cements to treat fractures.1 Failure of such techniques has not been reported widely, and this case series documenting treatment of VRF using a resin-ionomer — as proposed in prior papers — is presented to provide guidance to clinicians who face the decision to recommend repair or extraction of a VRF-affected tooth.
CASES HISTORIES

Five patients referred to a periodontal practice for management of severe vertical bone loss and suspected VRF were evaluated and found to have vertical fractures located subgingivally, on the root surface and only on one side of the tooth (unilateral). All teeth had previously been treated endodontically, but without resolution of the chronic infection and periodontal pocket associated with the tooth. In all cases, the bony defect was 10 mm or greater and demonstrated bleeding on probing and associated inflammation. Radiographic examination failed to demonstrate the fracture in any of the cases.
The area root surface was exposed using a full-thickness mucogingival flap as part of a diagnostic and therapeutic approach toward resolution. Periodontal debridement, consisting of ultrasonic and hand instrumentation, was completed, and the VRFs were repaired by enlarging the fracture with an inverted cone bur and filling the defect with a resin-ionomer (Figure 1, Figure 2 and Figure 3). The flap was closed using interrupted 4-0 gut sutures and the occlusion was adjusted to eliminate heavy interferences. Standard postoperative instructions were given, and pain medications and chlorhexidine prescribed.
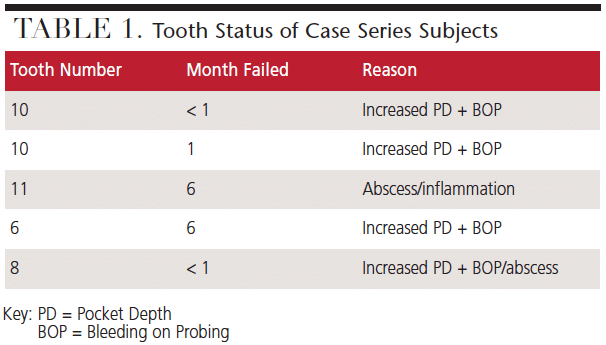
The teeth were examined at 1-week (for suture removal) and reprobed at the 1-, 3- and 6-month recall appointments. All teeth failed during this period and required extraction due to recurrent periodontal abscess, increased probing depth, inflammation and patient discomfort (Table 1).
DISCUSSION
The properties of resin-ionomers that make them useful in dental settings include being insoluble in oral fluids, adherence to tooth structure, low core shrinkage rates, low coefficients of thermal expansion, dual-cure capability, radiopacity, fluoride release and biocompatibility. Repair of VRFs does not ensure reattachment of soft tissue to the tooth, creating the possibility of continued pocket formation, plaque deposition and bacterial infection. Such activity can lead to wider involvement of the periodontium and alveolar bone, and potentially compromise adjacent teeth. Resin cements have also been shown subgingivally to serve as a structural matrix for microflora attachment and resulting biofilm.2

Some of the causes of VRF proposed over the years include physical trauma, occlusal trauma, repetitive heavy and stressful chewing, iatrogenic dental treatment,11 the direction of impact loading, and aggressive endodontic treatment21–26 — although studies have stated that an increased amount of dentin removal is not necessarily associated with increased risk of fracture.27 Mostly, the reports maintain that significant loss of tooth structure during endodontic treatment, along with instrumentation and excessive pressure during obturation, are the most likely causes of VRF.21,28–30 All of the cases reported here were previously treated endodontically. An association with bruxism has also been proposed as a possible cause of VRF,6,23 and in a demographic study, Cohen et al1 found this to be a factor in 35% of the cases examined.
Contradictory to general belief, radiographic findings alone are often not enough to diagnose VRF, mainly due to the fact that the emitted X-rays have to be in the same plane as the fracture line for the VRF to be observable. In addition, detection of the VRF varies with time after fracture and the degree to which the fragments have separated.1,8 Today, with the use of cone beam computed tomography or other enhanced imaging, such as the dental endoscope, clinicians have better diagnostic resources to evaluate teeth. In turn, this can help prevent unnecessary treatment.31 None of the cases presented in this paper had radiographic (specifically, vertical periapical radiographs) evidence of VRF.
Pulp vitality has proven to be somewhat useful in predicting the presence of VRF, and Cohen et al1 found that only 12.28% of cases of VRF were vital, while nonvital teeth were found in 39.04% of the cases studied. In the case of vital teeth, root fractures in nonendodontically treated teeth are commonly found to be apical extensions of coronal fractures.32,33 Clinical signs of odontogenic pathology are varied and not limited to VRF. These include pain on percussion, palpation or mastication, which were present in 60% to 70% of the cases of VRF — yet one-third of VRF cases in the study by Cohen et al1 were asymptomatic. In addition, tooth mobility was noted in 40% of the teeth examined, sinus tracts were reported in 20%, and deep periodontal pockets in 40%, but VRF was not a significant finding.1
CONCLUSION
Based on the outcomes of these cases that demonstrated 100% failure, clinicians should be cautious in deciding to attempt repair of a VRF by using resin-ionomer cements, as described in this limited case series. If such a technique is utilized, it is essential to have frequent recall in order to detect potential patterns of continued bone loss, progression of chronic infection at the fracture site, and possible case failure.
KEY TAKEAWAYS
- Vertical root fracture (VRF) has been recognized to be either a complete or an incomplete disruption of the tooth structure, and can involve one or both sides of the root.
- Detection of VRFs varies with time after fracture and the degree to which the fragments have separated.1,8
- Despite promising new imaging technologies, direct visualization by retraction of a full mucoperiosteal flap is still the most effective way to confirm most VRFs.
- Little data is available to suggest that vertical fractures of the root can be repaired for long-term preservation of the tooth.
- This limited case series documenting treatment of VRFs using a resin-ionomer — as proposed in prior papers — is presented to provide guidance to clinicians who face the decision to recommend repair or extraction of a VRFaffected tooth.
- Repair of VRFs does not ensure reattachment of soft tissue to the tooth, creating the possibility of continued pocket formation, plaque deposition and bacterial infection.
- Such activity can lead to wider involvement of the periodontium and alveolar bone, and potentially compromise adjacent teeth.
REFERENCES
- Cohen S, Berman LH, Blanco L, Bakland L, Kim JS. A demographic analysis of vertical root fractures. J Endod. 2006;32:1160–1163.
- Kawai K, Masaka N. Vertical root fracture treated by bonding fragments and rotational replantation. Dent Traumatol. 2002;18:42–45.
- Oliet S. Treating vertical fractures. J Endod. 1984;10:391–396.
- Arakawa S, Cobb CM, Rapley JW, Kilroy WJ, Spencer P. Treatment of root fracture by CO2 and ND:YAG lasers: an in vitro study. J Endod. 1996:22:662–667.
- Schwartz R. Mineral trioxide aggregate: a new material for endodontics. J Am Dent Assoc. 1999;130:967–975.
- Berman LH, Hartwell G. Diagnosis. In: Cohen S, Hargreaves KM, eds. Pathways of the Pulp. 9th ed. St. Louis: Mosby; 2006:2–39.
- Hassan B, Metska ME, Ozok AR, van der Stelt P, Wesselink PR. Detection of vertical root fractures in endodontically treated teeth by a cone beam computed tomography scan. J Endod. 2009;35:719–722.
- Moule AJ, Kahler B. Diagnosis and management of teeth with vertical root fractures. Aust Dent J. 1999;44:75–87.
- Kimura Y, Tanabe M, Amano Y, Kinoshita J, Yamada Y, Masuda Y. Basic study of the use of laser on detection of vertical root fracture. J Dent. 2009;37:909–912.
- Ebrahim AK, Wadachi R, Suda H. Accuracy of three different electronic apex locators in detecting simulated horizontal and vertical root fractures. Aust Endod J. 2006;32:64–69.
- Pitts D,L, Natkin E. Diagnosis and treatment of vertical root fractures. J Endod. 1983;9:338–346.
- Selden HS. Repair of incomplete vertical root fractures in endodontically treated teeth — in vivo trials. J Endod. 1996;22:426–429.
- Masaka N. Long-term observation of fractured tooth roots preserved by adhesion. Adhesive Dent. 1995;13:156–170.
- Miles DA, Anderson RW, Pashley DH. Evaluation of the bond strength of dentin bonding agents used to seal resected root apices. J Endod. 1994;20:538–541.
- Noguchi H, Sugaya T, Kato H. Treatment of vertically fractured root by cohesion, part 1: evaluations of cytotoxicity of adhesive resin cement with cultured periodontal ligament cells. Jpn J Cons Dent. 1997;40:1445–1452.
- Maeda H, Hashiguchi I, Nakamuta H, Toriya Y, Wada N, Akamine A. Histological study of periapical tissue healing in the rat molar after retrofilling with various materials. J Endod. 1999;25:38–42.
- Costa CA, Teixeira HM, do Nascimento AB, Hebling J. Biocompatibility of two current adhesive resins. J Endod. 2000;26:512–516.
- Teixeira HM, do Nascimento AB, Hebling J, De Souza Costa CA. In vivo evaluation of the biocompatibility of three current bonding agents. J Oral Rehabil. 2006;33:542–550.
- Bailey LO, Weir MD, Washburn NR. Quantification of macrophage viability and inflammatory response to dental bonding resins. J Bioactive Compatible Polymers. 2006;21:185–206.
- Saleem M, Ansari SR, Rehman K. Success of dental amalgam as a retrograde filling material — a comparative observational study. Pak Oral Dent J. 2010;30:229–231.
- Cohen S, Blanco L, Berman L. Vertical root fractures: clinical and radiographic diagnosis. J Am Dent Assoc. 2003;134:434–441.
- Zadik Y, Sandler V, Bechor R, Salehrabi R. Analysis of factors related to extraction of endodontically treated teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:31–35.
- Yeh CJ. Fatigue root fracture: a spontaneous root fracture in non-endodontically treated teeth. Br Dent J. 1997;182:261–266.
- Huang HM, Ou KL, Wang WN, Chiu WT, Lin CT, Lee SY. Dynamic finite element analysis of the human maxillary incisor under impact loading in various directions. J Endod. 2005;31:723–727.
- Bender IB, Freedland. Adult root fracture. J Am Dent Assoc. 1983;107:413–419.
- Lam PP, Palamara JE, Messer HH. Fracture strength of tooth roots following canal preparation by hand and rotary instrumentation. J Endod. 2005;31:529–532.
- Sathorn C, Palamara JE, Palamara D, Messer HH. Effect of root canal size and external root surface morphology on fracture susceptibility and pattern: a finite element analysis. J Endod. 2005;31:288–292.
- Dang DA, Walton RE. Vertical root fracture and root distortion: effect of spreader design. J Endod. 1989;15:294–301.
- Tamse A. Iatrogenic vertical root fractures in endodontically treated teeth. Endod Dent Traumatol. 1988;4:190–196.
- Holcomb Q, Pitts DL, Nicholls JI. Further investigation of spreader loads required to cause vertical root fracture during lateral condensation. J Endod. 1987;13:277–284.
- Mandelaris GA, Scheyer ET, Evans M, et al. American Academy of Periodontology best evidence consensus statement on selected oral applications for cone-beam computed tomography. J Periodontol. 2017;88:939–945.
- Cameron CE. Cracked-tooth syndrome. J Am Dent Assoc. 1964;68:405–411.
- Gher ME, Dunlap RM, Anderson MH, Kuhl LV. Clinical survey of fractured teeth. J Am Dent Assoc. 1987;114:174–177.
The authors have no commercial conflicts of interest to disclose.
FEATURED IMAGE: KATARZYNABIALASIEWICZ/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. January 2018;4(1):8-10,12.
