
Oral Manifestations of Crohn’s Disease
Dental providers can facilitate early diagnosis by recognizing the oral signs of this gastrointestinal condition.
Dental providers can facilitate early diagnosis by recognizing the oral signs of this gastrointestinal condition
This course was published in the May 2016 issue and expires 05/31/19. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Identify the criteria for diagnosing Crohn’s disease.
- List the oral signs and symptoms of this gastrointestinal condition.
- Explain treatment strategies for Crohn’s disease.
- Discuss oral health care considerations when treating these patients.
Each year, nearly 70 million Americans experience gastrointestinal conditions, such as inflammatory bowel disease (IBD).1 In order to facilitate early diagnosis and provide appropriate care to this patient population, dental professionals should look for the oral manifestations of these disorders — as well as side effects of the medications used to treat them.
Crohn’s disease and ulcerative colitis are chronic gastrointestinal conditions that fall under the IBD category. They affect nearly 2 million Americans, with approximately 70,000 new cases of IBD diagnosed each year.2 It can occur at any age, and is most prevalent in the northern regions of North America and Europe.3–8 While no specific food or diet has been pinpointed as the cause of IBD, a Western diet (i.e., low consumption of vegetables, and high intake of sugar, processed foods and industrial animal products) may play a role.3–8
Environmental, behavioral and genetic factors may contribute to the development of IBD. Using tobacco at a young age and gastroenteritis have been implicated independently as risk factors for IBD.8 New evidence suggests that individuals who were prescribed high levels of antibiotics in early childhood, and those with low vitamin D levels are at increased risk for IBD, particularly Crohn’s disease.9,10
This article will focus on the diagnostic signs and symptoms of Crohn’s disease, as well as considerations for treatment of patients with this gastrointestinal disorder.1
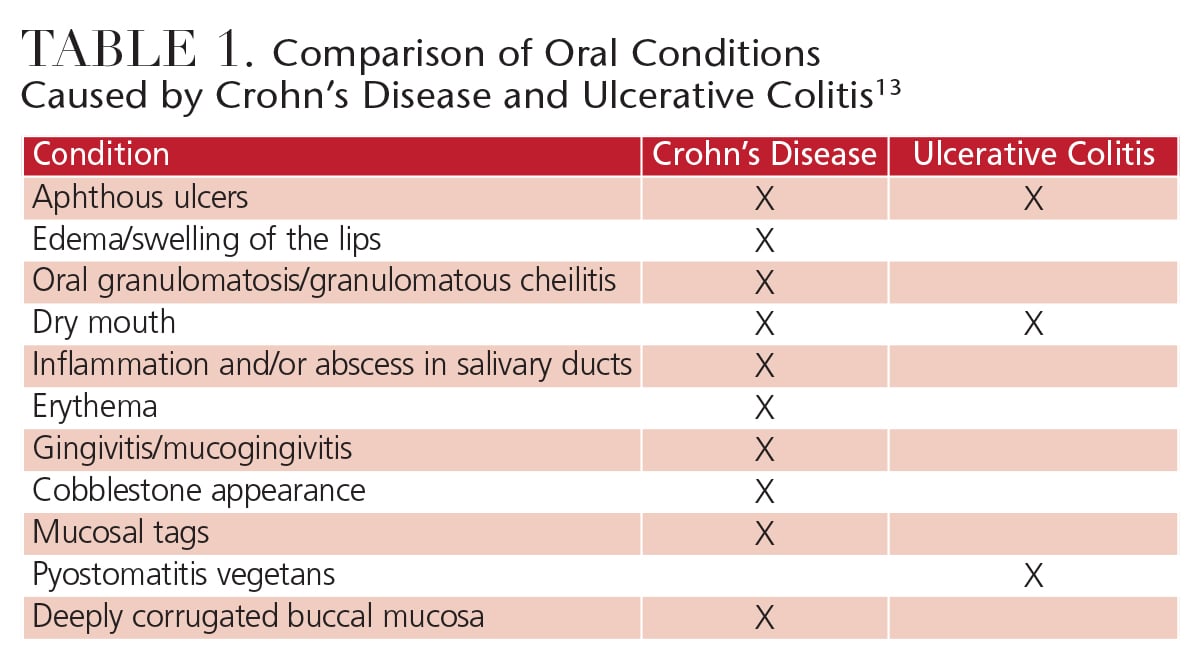
Both Crohn’s disease and ulcerative colitis are autoimmune disorders with similar signs, and the symptoms can range from mild to severe. They also exhibit periods of activity and remission.8 Symptoms include abdominal cramping, diarrhea and areas of ulceration within the intestinal tract that can cause intestinal bleeding.2,7 Patients with both variations of IBD may experience malnutrition and anemia due to impaired absorption of vitamins B, D, folic acid, iron and other critical nutrients. Malnutrition and anemia can cause serious oral health problems, including erythema, edema, angular cheilitis, glossitis, burning mouth syndrome, candidiasis, leukoplakic patches and gingivitis.2,7,11,12 In addition, ulcerative colitis can cause pyostomatitis vegetans, an uncommon oral manifestation that results in yellow, pus-filled lesions that frequently present with “snail track” patterns. Table 1 provides a comparison of the oral manifestations of Crohn’s disease and ulcerative colitis.13
REACHING A DEFINITIVE DIAGNOSIS
A diagnosis of Crohn’s disease is made via integrative interpretation of clinical, radiographic and laboratory analyses.11 Colonoscopy, ileoscopy and relevant biopsies are essential to making an accurate diagnosis at the junction of the ileum and colon. Endoscopic findings include skip lesions (alternating areas of ulceration and healthy tissue), cobblestoning (uneven projections of unaffected mucosa surrounded by ulcers that can cause longitudinal or circumferential fissures), and strictures.14–16 While these are considered as the gold standard for the diagnosis of Crohn’s disease, subjective assessments based on physical exams and patients’ descriptions of symtomology can also be considered.7,8 Definitive symptomatology includes the presence of nonnecrotizing granulomatous inflammation within the submucosal connective tissue of bowel or oral tissues.17
Crohn’s disease most frequently occurs in the distal portions of the small intestine, where the ileum approaches the large intestine. One third of cases occur in the colon itself.7 In addition to the location of intestinal lesions, patients are phenotyped using the Montreal classification, which considers age at diagnosis, disease site modifiers, and whether other autoimmune diseases are present.7 Once a definitive diagnosis is reached, treatment is determined based on the location and severity of the disease.
SIGNS AND SYMPTOMS

Common extraintestinal manifestations of Crohn’s disease include osteoporosis, asthma, changes to the skin (such as psoriasis), and the presence of other autoimmune conditions, including kidney stones or polyarticular arthritis.7 Crohn’s disease can also cause sensory impairments, such as hearing loss and eye problems, including uveitis.8
Chronic inflammatory disorders that overlap with Crohn’s disease may increase the risk for other systemic conditions, including autoimmune thrombocytopenia, autoimmune pancreatitis (resulting in type 1 diabetes), autoimmune hepatitis, psoriasis and gangrene.7 Patients with Crohn’s disease are also at increased risk of cancer and, compared to healthy individuals, are three times more likely to develop life-threatening blood clots.2

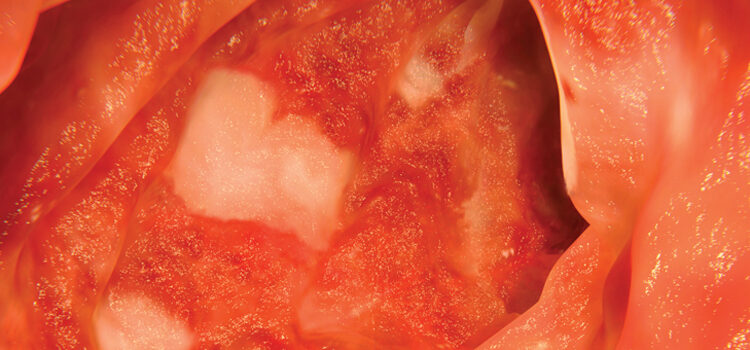
Oral manifestations of Crohn’s disease are not uncommon — especially in pediatric populations — and may be the first signs of the disease.9 Visible oral manifestations are similar to those found in the intestine, including cobblestone appearance of the mucosa, deep linear ulcerations, and mucosal tags. Oral manifestations may also include swelling of the lips, angular cheilitis, hyperplasia of erythematous gingiva,14 and recurrent ulcerations (Figure 1).11,12 Orofacial granulomatosis, or swelling of the orofacial area (Figure 2), is suggestive of Crohn’s disease, and typically appears without accompanying intestinal symptoms.18–21 Recent literature notes that orofacial granulomatosis manifests in almost half of children, and 20% to 50% of adults with Crohn’s disease.22 Whether orofacial granulomatosis is an oral manifestation of Crohn’s disease or a separate inflammatory condition remains unclear. Because it may be an early indicator of Crohn’s disease, children who present with this condition should be evaluated to facilitate early diagnosis.22
Esophageal involvement is also common,23 and symptoms may include dysphagia and heartburn or acid reflux caused by esophageal damage or lesions, including lichen planus. Patients should therefore be evaluated for signs of upper gastrointestinal symptoms.23 Knowledgeable oral health professionals can be instrumental in recognizing relevant signs and symptoms, and referring patients to their physicians for further examination and diagnosis.
TREATMENT AND MANAGEMENT STRATEGIES
Crohn’s disease symptoms recur without a clear pattern, and can be mild, moderate or severe. Treatment of Crohn’s disease is determined by disease location, activity and severity. These factors, when combined with the Crohn’s phenotype and imaging from endoscopic examination, are key in predicting the disease sequelae and potential complications.7
Traditional treatments for Crohn’s disease include pharmacotherapy and surgery. Medication regimens consist of five main pharmacological approaches: anti-inflammatory medications (e.g., sulfasalazine and mesalamine), steroidal therapies (prednisone), antibiotics (metronidazole, ciprofloxacin), immunomodulators (methotrexate, azathioprine), and biologic therapies (infliximab, adalimumab).2,7 Almost 75% of individuals with the disease will eventually require surgical therapy, such as strictureplasty, colectomy, proctocolectomy, or conservative surgical resection of the diseased bowel.2,24 Patients may also require other dietary interventions, including enteral nutrition.
Optimal treatment for Crohn’s disease remains controversial. Currently, two principal strategies are used: a traditional step-up approach, and a top-down approach. In the step-up approach, corticosteroids or mesalamine products are introduced, with subsequent advancement to immunomodulators or anti-tumor necrosis factor (anti-TNF) agents, depending on disease severity. In the top-down approach, treatment begins with anti-TNF agents.14 Although earlier reports suggested exclusion of specific food types as a possible treatment,19 a Cochrane Database review concluded that corticosteroid therapy is more effective than enteral nutrition for inducing remission of active Crohn’s disease.25
CONSIDERATIONS FOR ORAL CARE
Patients with mild manifestations of Crohn’s disease may receive dental care without complications. Oral manifestations of the disease are not typically problematic, and may not need specific oral treatment; in fact, most often, they will resolve over time without intervention.19 But for patients who exhibit the recurrent aphthous ulcerations that occur in 10% of affected individuals, topical steroids may reduce healing time of ulcers and help alleviate pain.26,27 In a recent study of pediatric patients with Crohn’s disease, a multidrug treatment that included azathioprine appeared to help mitigate oral manifestations.21 Some patients with Crohn’s disease, however, may present with large oral ulcers that require treatment with biologics (specific proteins, as opposed to chemical medications) to manage these lesions.27
Many of the medications prescribed for Crohn’s disease are immunosuppressants and biologics that may cause myriad oral and systemic side effects. For example, patients with Crohn’s disease who are taking biologics are at increased risk for infections, such as tuberculosis and hepatitis. These patients should be encouraged to remain up to date on their vaccinations, including influenza, pneumococcal, hepatitis A, hepatitis B, tetanus, diphtheria, human papillomavirus, pertussis and polio. Patients who are immunocompromised should receive immunizations that do not contain viable microbes.7
Other commonly prescribed Crohn’s medications include corticosteroids, which help reduce the inflammatory process of the disease and promote healing. Patients who take corticosteroids for long periods often require careful monitoring of blood pressure and blood glucose levels.8 To ensure safe treatment, oral health professionals should note in the patient’s chart to monitor blood pressure and blood glucose levels at each visit. Treatment alterations, such as scheduling short morning appointments, may be necessary.
As noted, tobacco use is a risk factor for Crohn’s disease. In fact, smokers are two times more likely to develop the disease than nonsmokers.2 Smoking is also a risk factor for Crohn’s-related complications, increasing the occurrence of fistulas and intestinal strictures. Additionally, smoking can prolong flare-ups and interfere with prescribed pharmacotherapies and other treatments.7 As with all patients, dental professionals should encourage patients with Crohn’s disease to stop using tobacco products.
Crohn’s disease frequently interferes with the absorption of nutrients, leading to malnutrition. Clinicians should be aware of oral signs of malnutrition, and the resultant deficiencies in vitamins and minerals that can cause a variety of oral complications. Anemia can increase the risk of periodontal disease, while other nutrient deficiencies can cause candidiasis and angular cheilitis.
Patients with Crohn’s disease may find it difficult to digest some foods. Whole grain and high-fiber foods can exacerbate symptoms of cramping and diarrhea. Small, frequent meals that are soft in consistency, have minimal fiber, and are low in carbohydrates may be recommended to ease digestion. This type of diet, however, may increase caries risk. As such, oral health professionals should carefully assess caries risk, provide appropriate patient education, implement caries risk management plans, and offer nutritional counseling, as necessary.
Pharmacotherapy regimens, extraintestinal manifestations and/or concurrent autoimmune conditions are important considerations for clinicians treating patients with Crohn’s disease. Osteoporosis and asthma are also common conditions that may be seen in individuals with Crohn’s disease. Past or ongoing bisphosphonate therapy for the treatment of osteoporosis can have implications for more invasive dental procedures, such as extractions. Generally, patients who have taken oral bisphosphonate for less than four years and have no clinical risk factors do not require any alteration or delay in the provision of routine dental care.28 On the other hand, patients who need invasive dental procedures should be carefully evaluated for the risk of osteonecrosis of the jaw.
Because asthma is often seen in patients with Crohn’s disease, the use of ultrasonic scalers may be inadvisable.29 Additionally, many asthma medications can cause oral side effects, such as xerostomia and increased caries risk. Patients should be educated about possible side effects and increased caries risk, as well as the importance of self-care that can mitigate risks — such as rinsing the mouth immediately after using an inhaler.
Blood thinners are prescribed to some patients with Crohn’s disease to limit the risk of blood clotting. Several of these medications require patients to regularly undergo coagulation testing, with the international normalized ratio (INR) most often used as the standard. The ideal INR values for patients taking blood thinners is 2.0 to 3.0.
Adults, adolescents and children with Crohn’s disease are more likely to experience severe oral disease than their healthy counterparts. Studies have shown an increased prevalence of periodontal disease and caries among individuals with Crohn’s disease.30,31 Despite showing minimal biofilm accumulation, these patients tend to have high decayed, missing or filled teeth scores. They are also likely to have bleeding on probing, and display a tendency toward deep periodontal pockets.28 Thus, clinicians should execute careful, regular monitoring of caries and periodontal risks to help patients with Crohn’s disease maintain optimal oral health.
CONCLUSION
Oral health professionals will most likely encounter patients with Crohn’s disease in the dental setting. Their treatment commonly will require a collaborative effort that includes dental providers and primary care physicians/gastroenterologists. Because manifestations of Crohn’s disease may appear in the oral cavity before intestinal signs are noted, dental professionals should be aware of the disease’s signs and symptoms, so a referral for definitive diagnosis can be made.
While some patients with Crohn’s disease may present with minimal or no complications, others may experience problems that significantly impact the provision of oral health care. A careful review of patients’ medical histories, medication regimens, and dietary habits is necessary to create personalized and safe oral treatment plans.
References
- Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology. 2012;143:1179–1187.
- Crohn’s and Colitis Foundation of America. The Facts About Inflammatory Bowel Diseases. Available at: ccfa.org/ assets/pdfs/ibdfactbook.pdf. Accessed April 15, 2016.
- Loftus EV. Clinical epidemiology of inflammatory bowel diseases: Incidence, prevalence and environmental influences. Gastroenterology. 2004;126:1504–1517.
- Hou JK, Abraham B, El-Serag H. Dietary intake and risk of developing inflammatory bowel disease: A systematic review of the literature. Am J Gastroenterol. 2011;106:563–573.
- Ko Y, Butcher, R, Leong RW. Epidemiological studies of migration and environmental risk factors in the inflammatory bowel diseases. World J Gastroenterol. 2014;20:1238–1247.
- Kappelman MD, Moore KR, Allen JK, Cook SF. Recent trends in the prevalence of Crohn’s disease and ulcerative colitis in a commercially insured U.S. population. Dig Dis Sci. 2011;58:519–525.
- Baumgart DC, Sandborn WJ. Crohn’s disease. Lancet. 2012;380:1590–1605.
- Baumgart DC, Sandborn WJ. Inflammatory bowel disease: Clinical aspects and established and evolving therapies. Lancet. 2007;369:1641–1657.
- Schulfer A, Blaser MJ. Risks of antibiotic exposures early in life on the developing microbiome. PLoS Pathogens. 2015;11:1–6.
- Ham M, Longhi MS, Lahiff C, Cheifetz A, Robson S, Moss AC. Vitamin D levels in adults with Crohn’s disease are responsive to disease activity and treatment. Inflamm Bowl Dis. 2014;20:856–860.
- Alawi F. An update on granulomatous diseases of the oral tissues. Dent Clin North Am. 2013; 57:657–671.
- Katsanos KH, Torres J, Roda G, Brygo A, Delaporte E, Colombel JF. Review article: Non-malignant oral manifestations in inflammatory bowel diseases. Aliment Pharmacol Ther. 2015;42:40–60.
- Ormond M, Sanderson JD, Escudier M. Disorders of the mouth. Medicine. 2015;43:187–191.
- Wilkins T, Jarvis K, Patel J. Diagnosis and management of Crohn’s disease. Am Fam Physician. 2011;84:1365–1375.
- Richards CJ. Pathological considerations in Crohn’s disease. In: Rajesh A, Sinha R, eds. Crohn’s Disease: Current Concepts. Cham, Switzerland: Springer International Publishing; 2015:11–21.
- Ye Z, Lin Y, Cao Q, He Y, Xue L. Granulomas as the most useful histopath – ological feature in distinguishing between Crohn’s disease and intestinal tuberculosis in endoscopic biopsy specimens. Medicine (Baltimore). 2015;94:1–9.
- Neville BW. Oral and Maxillofacial Pathology. St. Louis: Elsevier/Saunders; 2009:968.
- Scully C, Cochran KM, Russell RI, et al. Crohn’s disease of the mouth: An indicator of intestinal involvement. Gut. 1982;23:198–201.
- Rowland M, Fleming P, Bourke B. Looking in the mouth for Crohn’s disease. Inflamm Bowel Dis. 2010; 16:332–337.
- Tilakaratne WM, Freysdottir J, Fortune F. Orofacial granulomatosis: Review on aetiology and pathogenesis. J Oral Pathol Med. 2008:37:191–195.
- Ejeil A-L, Thomas A, Mercier S, Moreau N. Unusual gingival swelling in a 4-year-old child. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;118:627–631.
- Lazzarini M, Martelossi S, Cont G, et al. Orofacial granulomatosis in children: Think about Crohn’s disease. Dig Liver Dis. 2015;47:338–341.
- DeFelice KM, Katzka DA, Raffals LE. Crohn’s disease of the esophagus: Clinical features and treatment outcomes in the biologic era. Inflamm Bowel Dis. 2015;21:2106–2113.
- Dignass A, VanAssche G, Lindsay JO, et al. The second European evidencebased consensus on the diagnosis and management of Crohn’s disease: current management. J Crohns Colitis. 2010;4:28–62.
- Zachos M, Tondeur M, Griffiths AM. Enteral nutritional therapy for induction of remission in Crohn’s disease. Cochrane Database Sys Rev. 2007;1:CD000542.
- Quijano D, Rodriguez M. Topical corticosteroids in recurrent aphthous stomatitis. Systematic review. Acta Otorrinolaringol Esp. 2008;59:298–307.
- Beltran B. Extrainitestinal manifestations of inflammatory bowel disease: Do they influence treatment and outcome? World J Gastroenterol. 2011:17:2702–2707.
- Ruggiero SL, Dodson TB, Fantasia J, et al. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw — 2014 update. J Oral Maxillofac Surg. 2014;72:1938–1956.
- Bateman ED, Hurd SS, Barnes PJ, Bousquet J, et al. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2008;31:143–178.
- Koutsochiristou V, Zellos A, Dimakou K, et al. Dental caries and periodontal diseases in children and adults with inflammatory bowel disease: A casecontrol study. Inflamm Bowel Dis. 2015;21;1839–1846.
- Brito F, deBarros FC, Zaltman C, et al. Prevalence of periodontitis and DMFT index in patients with Crohn’s disease and ulcerative colitis. J Clin Periodontol. 2008;35:555–560.


[…] to Decisions In Dentistry, IBD can manifest itself in the oral cavity, particularly in pediatric cases. Some oral signs and […]