

Oral Care for Patients With Alzheimer’s Disease
With special strategies and simple appointment modifications, individuals with this common form of dementia can be successfully treated in traditional dental settings.
PURCHASE COURSE
This course was published in the April 2023 issue and expires April 2026. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the April 2023 issue and expires April 2026. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 750
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify oral diseases commonly found in those with Alzheimer’s disease (AD).
- Discuss oral hygiene strategies for individuals with AD.
- Implement appropriate modifications to support successful dental appointments for this patient population.
PART 2 of a two-part series: This is the concluding installment of a short series exploring oral health considerations for patients with Alzheimer’s disease. Part 1, which covered the risks, signs and progression of Alzheimer’s disease, appeared in the March issue and is available at here.
Alzheimer’s disease (AD) is the most common type of dementia, and more than 6 million Americans live with this progressive condition.1 Given these numbers, oral health professionals should be prepared to provide safe and effective care. Implementing special strategies and techniques may help increase the likelihood of successful dental visits for this patient population, which is subject to a number of common oral diseases.
For example, individuals with dementia frequently present with hyposalivation, which may increase biofilm accumulation, as well as the risk for oral diseases.2 Xerostomia is a common side effect of medications used to manage symptoms of mild to severe AD, including donepezil, galantamine and memantine.3,4 Medications used to treat the comorbidities of AD, such as antidepressants, antipsychotics and sedatives, may also cause dry mouth.5
Xerostomia leads to a host of oral health issues, including tenacious biofilm formation, caries, candidiasis, dysphagia, and difficulty retaining dentures.6
Older adults with dementia often experience poor oral health, and biofilm accumulation is frequently the root cause.7 Research shows that individuals living with dementia have high levels of biofilm in the oral cavity.2 Compared to patients without dementia, a 2018 systematic review and meta-analysis reported that those with dementia have higher plaque indices, more bleeding on probing, higher gingival bleeding indices, higher probing depths, and more clinical attachment loss.8
Moreover, coronal and root caries are more common among those with dementia than older adults without dementia.7 As dementia progresses, the risk for gingival disease and caries rises due to xerostomia, forgetting to brush the teeth (or forgetting how to brush), or not wanting to brush due to the sensation.2
An analysis of the effects on oral health based on where an individual with dementia resides has shown that living situation appears to have little impact. A cross-sectional study with 552 participants concluded that individuals with dementia have poor oral health no matter if they live in a long-term care facility or at home.9 The rate of caries and retained roots of those living in nursing home facilities was similar to the rate of those who lived at home.9 While nursing homes are federally mandated to evaluate residents’ oral health needs and facilitate access to dental care, compliance in the past has been low,10 and no recent data have been published. Another consideration is that nursing home staff may lack awareness of the health benefits of proper oral hygiene, and such facilities can experience high turnover rates.10 Additionally, no matter their place of residence, individuals with dementia may resist a care partner assisting them with oral care, leading to poor oral health.10
ORAL CARE ASSISTANCE
patients with Alzheimer’s disease.
People with AD will eventually need assistance with activities of daily living.3 In the early stages of AD, the individual is encouraged to be self-sufficient. As the disease progresses, more assistance from a care partner is needed.
A patient with dementia may forget what to do with toothpaste or how to rinse without swallowing.11 Object recognition and purpose become less familiar for people living with dementia.12 Individuals in the mild to late stages of AD should avoid using mouthrinse, because it can easily be mistaken for a beverage, leading to nausea or vomiting if swallowed. The shape of a toothpaste tube might also look like another product, such as an ointment or cream. This could cause confusion. Dental products may need to be labeled with a simple phrase so individuals with dementia recognize them. Mistakenly rubbing toothpaste on the skin when thinking it is a pain-relieving joint cream is not problematic, but brushing teeth with a pain-relieving joint cream could be of concern.
During the mid to late stages of AD, many individuals experience increasing levels of agitation and resistance, which may make oral care more difficult.11 One reason for resistance may be intolerance of the way something feels in the mouth. Sensation in the mouth, lips and tongue may be heightened during these stages of dementia, which could lead to exaggerated responses.12
Due to language deficits, the individual with dementia may not understand what the care partner is saying, hindering cooperation. Comprehension deficits occur during the moderate and late dementia stages due to a decline in the ability to create sentences and diminished working memory.13 Care partners may need to use short, simple instructions during oral care; for example, by saying: “Hold the toothbrush. Squeeze the paste. Brush your teeth.”11
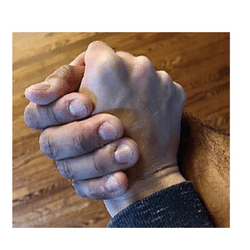
Another strategy to encourage cooperation when providing oral care assistance is using hand-under-hand guidance (Figure 1 and Figure 2).14 This technique enables individuals with AD to feel like they are performing the task, too, instead of someone performing the task for them. In hand-under-hand guidance, care partners use their own skill fingers (thumb, index and middle fingers) to complete the task while the patient’s hand is on top. Figure 2 demonstrates this with the toothbrush being held by the care partner. A short video on using hand-under-hand guidance for toothbrushing is available at youtube.com/watch?v=6gLrH8mioCw. The video was created by Snow, who founded Positive Approach to Care (teepasnow.com), an organization whose mission is to enhance life and the relationships of those living with brain change by fostering an inclusive global community.
Oral care for those living with dementia should follow the standard of care. The American Dental Association recommends biofilm removal by brushing teeth twice daily for two minutes.15 A manual toothbrush made for individuals with limited dexterity may be helpful. One example includes a toothbrush with bristles on three surfaces, which allows simultaneous brushing of the occlusal, lingual and buccal surfaces. The unique design of the bristles facilitates removal of biofilm from all surfaces of the teeth with a simple brushing stroke that can be performed by most individuals. Timers can be set to ensure users are brushing for at least two minutes.

A dentifrice with ingredients that control biofilm growth, such as stannous fluoride, may prevent caries and periodontal inflammation. Stannous fluoride inhibits biofilm growth and modifies the composition of organisms in the biofilm.16 Other methods of biofilm removal include use of a tongue scraper and interdental devices. The mouth is highly sensitive and oral care can trigger a negative response among those with AD.12 If one dental product is not tolerated, a different one should be tried until cooperation is gained.
Effectively removing biofilm daily may impact more than the mouth. Oral bacteria can be aspirated into the lungs, increasing the risk for aspiration pneumonia, which is the most common cause of death in those with late-stage AD.17,18
APPOINTMENT MODIFICATIONS
Prior to beginning the appointment, clinicians should determine if the patient is capable of providing consent. In the early stages of AD, the individual may have no issues giving consent. Those with mild AD may still be driving to the appointment alone. As the disease progresses, consent for treatment should be obtained from the legal guardian. Medical history forms may not ask about cognitive disorders and their presence may not be obvious. Thus, dental teams may need to ask more questions after reviewing the completed forms to determine if the patient is capable of providing consent.
When caring for this patient population, appointment planning should consider the length of time needed for the visit, as shorter appointments may reduce stress experienced at the dental office.
More appointment modifications will be needed as AD progresses. While still cooperative, individuals with mild AD should be seen for a comprehensive examination, radiographs, creation of a treatment plan, and dental hygiene services.19
In the mid-stage of AD, maintenance procedures should continue. If treatment was not rendered before the patient reached the mid-stage, extensive treatment may be necessary.19 Oral sedation may be helpful at this point. Minimally invasive restorative options, such as the application of silver diamine fluoride, may be well tolerated because the treatment is completed quickly.19
When appropriate, teeth at risk for future problems should be extracted while in the mid-stage of AD.19 Once the late stage of AD is reached, treatment in the dental setting becomes more challenging. Use of deep sedation or general anesthesia may facilitate care for these patients.19
The shrinking volume of the brain of an individual with AD eventually impacts most bodily functions.20 This requires providers to change their approach to make dental appointments successful for all involved.
POSITIVE PHYSICAL APPROACH
A part of Snow’s Positive Approach to Care program, the Positive Physical Approach prevents the individual with AD from being startled and allows for welcomed interaction. The approach begins by knowing the two zones of interaction. Public space is six feet away from the individual. In this zone, the clinician can greet patients and gain their attention while in their narrowed field of vision.
A helpful way to gain eye contact is to place an open hand near the face, smile, and greet the individual by name. Next, try to move into the patient’s personal zone by extending a hand to shake. If the individual accepts by extending his or her hand, this is an invitation into the personal zone and the handshake can proceed. The handshake can now shift into the hand-under-hand grasp, as seen in Figure 1, and the provider moves to the patient’s side, which is called a supportive stance, as opposed to a confrontational stance (i.e., standing directly in front of the individual). Using a supportive stance may prevent feelings of blocking the individual’s escape path.21 Maintain this stance while walking the patient to the dental chair.
Before initiating movement toward the operatory, a positive and personal connection — obtained by methods such as complimenting the individual or identifying an unmet need or want — should be established.21
After connecting with the individual, clinicians can also incorporate positive action starters. These starter phrases should be short and easy to understand, which helps give the individual with AD a sense of choice and autonomy. These may include holding up an item and asking if it is OK to try it; asking the person to help with a task (such as turning the head to the right); offering choices on which flavor prophy paste to use; and providing single-step directions to complete a task.21
Avoid asking the individual if he or she is ready or wants to do something, as this results in a yes or no answer. If the answer is no and the task needs to be completed during an appointment, it may create conflict.
Verbal, visual and physical connection with the patient may assist with engagement and compliance during the appointment. As hearing is not affected by AD, verbal connection should be a starting point.12 It could lead to a visual connection to gain the individual’s attention, while physical touch maintains that connection.
ENCOURAGING COOPERATION
Dental professionals should be cheerful and kind to facilitate cooperation during the appointment. Remaining calm, being patient, and using simple language with short verbal commands may be key to this cooperation. Consider the field of vision when interacting and approach the individual from the middle of the field to avoid startling the patient.12
In practice, providers frequently enter a patient’s field of vision from the side or from the top of the head, which might feel like a sudden threat since peripheral vision is lost.12 Establish eye contact to maintain focus on what is being said. Attention can also be gained through a physical connection, such as gently squeezing the patient’s hand if already in a hand-under-hand grasp.
Clinicians should also be aware of habits to avoid during the visit. Refrain from questioning the patient with phrases such as, “Don’t you remember me? I treated you last time.” Avoid disagreeing when inaccurate information is shared. Practice patience when the individual completes tasks slowly; do not take over and complete tasks for a patient with AD.
A shorter recare interval may offer the most benefit for patients with AD, as biofilm can be controlled with supragingival and subgingival debridement. As AD progresses, a shorter recare interval may aid in caries prevention.19
CONCLUSION
While the oral issues that accompany AD pose challenges, dental teams can assist those with AD and their care partners by implementing strategies for prevention and treatment. Knowing the most effective ways to interact with individuals with AD may facilitate cooperation and increase the likelihood of successful treatment and a positive experience at the dental office.
References
- Alzheimer’s Association. What is Dementia? Available at: https://www.alz.org/alzheimers-dementia/what-is-dementia. Accessed February 27, 2023.
- Delwel S, Binnekade T, Perez R, Hertogh C, Scherder E, Lobbezoo F. Oral hygiene and oral health in older people with dementia: a comprehensive review with focus on oral soft tissues. Clin Oral Investig. 2018;22:93–108.
- Alzheimer’s Association. 2022 Alzheimer’s Disease Facts and Figures. Available at: http://alz.org/media/ Documents/Alzheimers-facts-and-figures.pdf. Accessed February 27, 2023.
- Medications for Alzheimer’s Disease. Available at: https://www.drugs.com/ condition/alzheimer-s-disease.html. Accessed February 27, 2023.
- Cockburn N, Pradhan A, Taing MW, Kisely S, Ford PJ. Oral health impacts of medications used to treat mental illness. J Affect Disord. 2017;223:184–193.
- American Dental Association. Xerostomia (dry mouth). Available at: https://www.ada.org/resources/research/science-and-research-institute/oral-health-topics/xerostomia. February 27, 2023.
- Lauritano D, Moreo G, Della Vella F, et al. Oral health status and need for oral care in an aging population: a systematic review. Int J Environ Res Public Health. 2019;16:4558.
- Maldonado A, Laugisch O, Bürgin W, Sculean A, Eick S. Clinical periodontal variables in patients with and without dementia — a systematic review and meta-analysis. Clin Oral Investig. 2018;22:2463–2474.
- Chen X, Clark JJ, Naorungroj S. Oral health in older adults with dementia living in different environments: a propensity analysis. Spec Care Dentist. 2013;33:239–247.
- Sifuentes AMF, Lapane KL. Oral health in nursing homes; what we know and what we need to know. J Nurs Home Res Sci. 2020;6:1–5.
- Alzheimer’s Association. Dental Care. Available at: https://www.alz.org/help-support/caregiving/daily-care/dental-care. Accessed February 27, 2023.
- Snow T. Workshop A: normal aging vs. not normal aging. Available at: learn.teepasnow.com/trainer-post-certification-tools/. Accessed February 27, 2023.
- Liu X, Wang W, Wang H, Sun Y. Sentence comprehension in patients with dementia of the Alzheimer’s type. Peer J. 2019;7:e8181.
- Batchelor-Aselage M, Amella EJ, Rose SB, Bales CW. Dementia-related mealtime difficulties: Assessment and management in the long-term-care setting. In: Bales CW, Locher JL, Saltzman E, eds. Handbook of Clinical Nutrition and Aging. New York: Springer; 2015:287–301.
- American Dental Association. Toothbrushes. Available at: https://www. ada.org/resources/research/science-and-research-institute/oral-health-topics/toothbrushes. Accessed February 27, 2023.
- Xingqun C, Jinman L, Jiyao L, et al. Comparative effect of a stannous fluoride toothpaste and a sodium fluoride toothpaste on a multispecies biofilm. Arch Oral Biol. 2017;74:5–11.
- Alzheimer’s Association. Late-Stage Caregiving. Available at: https://www. alz.org/help-support/caregiving/stages-behaviors/late-stage. Accessed February 27, 2023.
- Kalia M. Dysphagia and aspiration pneumonia in patients with Alzheimer’s disease. Metabolism. 2003;52(10 Suppl 2):36–38.
- Marchini L, Ettinger R, Caprio T, Jucan A. Oral health care for patients with Alzheimer’s disease: an update. Spec Care Dentist. 2019;39:262–273.
- Alzheimer’s Association. Inside the Brain — A Tour of How the Mind Works. Available at: https://www.alz.org/ alzheimers-dementia/what-is-alzheimers/brain_tour. Accessed February 27, 2023.
- Positive Approach to Care. PPA Resource Card 25-pack. Available at: shop.teepasnow.com/product/ppa-cheat-sheet-25-pack. Accessed February 27, 2023.
From Decisions in Dentistry. April 2023;9(4):30-33.

