

Noncarious Cervical Lesions and the Abfractive Process
The use of correct bio-dental engineering terms can help explain the cause-and-effect relationships for noncarious cervical lesions and abfractions.
The use of correct bio-dental engineering terms can help explain the cause-and-effect relationships for noncarious cervical lesions and abfractions
Caries lesions are the most common cause of enamel and dentin breakdown, and are promoted as bacterial in origin. However, not all breakdowns primarily involve bacteria.1 One condition that is not a result of bacterial manifestation is what has commonly been termed noncarious cervical lesions, frequently referred to as abfractions.2 Characterized by a loss of hard dental tissue, these lesions (Figure 1) are most commonly found near the cementoenamel junction (CEJ). Notably, noncarious cervical lesions have defined internal and external angles. They most often occur on the facial surfaces of the teeth and are typically wedge- or V-shaped (Figure 2 and Figure 3).3 This article explores historic and current thoughts regarding noncarious cervical lesion etiologies, explains abfraction, presents modern bio-dental engineering terms, and offers treatment recommendations based on the existing evidence.

The term abfraction means to “break away” and is a manifestation of the flexion mechanism from stress. Contemporary understanding is the etiology of abfractive lesions — a form of noncarious cervical lesions — is due to occlusal-load forces.2 Current conceptual understanding continues to investigate the etiology, however. Research indicates the cause of noncarious cervical lesions is not occlusal factors alone, but, rather, multifactorial — especially involving biocorrosion in combination with cervical stress stemming from hyperfunctional or parafunctional occlusal forces. Biocorrosion has been defined as endogenous or exogenous chemical, biochemical or electrochemical effects to teeth, as well as agents producing proteolysis.4 This article highlights various considerations for the causes of abfractions and noncarious cervical lesions. It also addresses the reasons that restoration of these lesions should be carefully considered before providing treatment of any kind.4
These presentations are not uncommon in clinical practice. Research shows that of more than 1300 subjects, 63% was diagnosed with noncarious cervical lesions. The proportion of subjects (or teeth) with lesions increased dramatically with advanced age. Premolars were the most commonly affected in earlier years, but lesions were not limited to these teeth.5,6
MULTIFACTORIAL ETIOLOGY
The concepts of abfraction, abrasion and biocorrosion are not well understood by the dental profession. For example, in the defining abfraction, some textbooks state it is a discrete clinical entity, although there is general agreement that the etiology is multifactorial.5,7 For this article, Summitt’s Fundamentals of Operative Dentistry will be used to define various terms, but some may come from the publications of Grippo or Grippo and colleagues. Abrasion is a mechanical process that involves wearing away of a substance or structure through friction. Examples of friction are dental abrasion owing to aggressive toothbrushing or occlusal surface wear due to attrition. Biocorrosion includes the progressive loss of tooth structure through chemical processes that could also involve bacterial action. Abfraction is thought to be a noncarious cervical lesion caused by occlusally produced tooth flexure.4

In 1907, Miller8 discussed the origin of what we now refer to as noncarious cervical lesions. He studied experiments and observations on the wear of teeth described as abrasion, chemical abrasion, chemical denudation, erosion and others. It was not until the late 1970s the concept evolved that occlusal loading could cause stress at the CEJ, resulting in loss of tooth structure. Subsequently, Rees9 used an in vitro computer model termed finite element analysis to make a case that excessive occlusal stresses at the CEJ existed.9 The data from this study, as well as research from Sarode and Sarode,10 indicate it was produced by occlusal forces, but could not show that it caused noncarious cervical lesions. The primary etiology of these lesions is considered to be occlusal forces causing tooth crowns to flex, shearing the enamel and dentin away from the tooth at the CEJ, in combination with the mechanism defined as biocorrosion (which replaces the dental term erosion).11 After considerable effort to demonstrate these occlusal forces are a cause of noncarious cervical lesions, the etiology remained poorly understood and controversial.12–14

Grippo2 coined the term abfraction in 1991. Clinical investigations confirming a positive association between excessive occlusal loading and abfractive lesions approach this topic differently. In 1977, Xhonga15 reported a relationship between the extent of occlusal wear, bruxism, and the presence of what later would be termed abfractions. Coleman et al16,17 found a high degree of association between cervical dentin hypersensitivity (CDH) and abfractions by location and distribution. Although the authors did not so state in their 2000 and 2003 publications, occlusal therapy resolved CDH for noncarious cervical lesions produced by stress, not necessarily the more recently specified designation of abfractions.16,17 Sawlani et al18 used more modern terminology in their investigation, and reported that heavy occlusal forces played a significant role in the development of noncarious cervical lesions. They also dismissed abrasion as a less-than-major factor in their development.
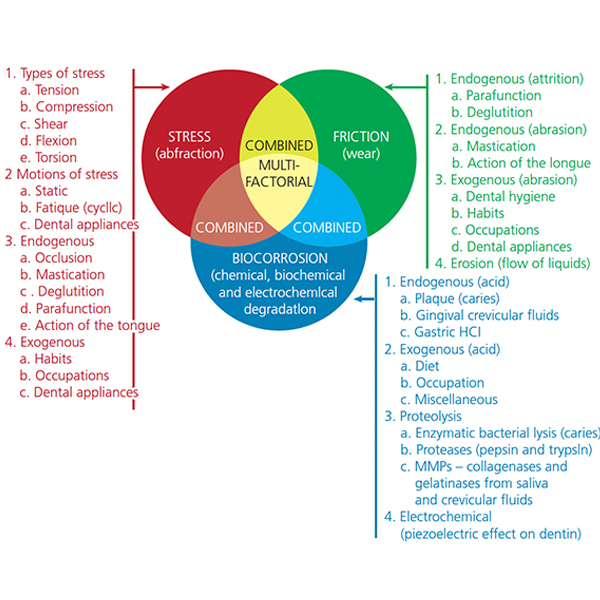
Today, the term biocorrosion better defines the chemical, biochemical and electrochemical mechanism of noncarious cervical lesions; it replaces former terms corrosion, erosion and others relating to hard tissue degradation. Biocorrosion encompasses endogenous and exogenous acidic and proteolytic chemical degradation of enamel and dentin, as well as the piezoelectric electrochemical action on the collagen of dentin. Aaron12 proposed it is incorrect to designate only one mechanism to be the cause of these lesions. Figure 4 shows the schema of pathodynamic mechanisms of tooth surface loss introduced by Grippo et al19 as an amended version of its initial appearance in an earlier publication. Figure 4 illustrates the complex cofactorial nature of bio-dental engineering mechanisms of stress, biocorrosion and friction, as they apply to dental hard tissue degradation. It is frequently difficult to identify any of these three mechanisms as the major etiologic cofactor in noncarious cervical lesion formation or progression.
CASE REPORT
A 62-year-old male presented to the University of Arkansas, Fort Smith Dental Hygiene School for evaluation and routine oral hygiene treatment. He reported an esthetic concern for the upper right first premolar (Figure 5A). This buccal noncarious cervical lesion on tooth #5, as well as the wear pattern on the lingual surface of what appeared as an adjacent deciduous cuspid, prompted a thorough dental history, clinical evaluation and radiographic analysis.
There was no evidence of prior restorative treatment for tooth #5. Although not shown in the Figure 5 series, a panorex film disclosed a high horizontal impaction of tooth #6. An abfraction was found on the contralateral buccal aspect of tooth #21 (Figure 5B). No other noncarious cervical lesions existed for this patient. Figure 5C shows partial maximal intercuspal position closure, whereas Figure 5D illustrates more complete interarch tooth contacts. Upon report by the patient, no evidence of bruxing was active. Clinical interpretation did not uncover evidence of either endogenous or exogenous excessive biocorrosion or pathology by friction related to toothbrush/dentifrice abrasion. The passive supereruption of tooth # 5 and lack of a rapid cuspid-rise for the right lateral excursion seemed likely responsible for development of noncarious cervical lesions for teeth #5 and #21.

Summarily, this patient was referred to a general dentist for diagnosis and treatment. Familiarity with the Grippo and Oh Venn schema (Figure 4) is deemed useful for clinical interpretation of causative factors for noncarious cervical lesions.
ANCIENT VERSUS MODERN ENVIRONMENTS
In an effort to evaluate occlusal forces as a cause, a thesis by Aaron12 on noncarious cervical lesions revealed that when comparing occlusal wear to the number of abfractions in a study of modern versus ancient human skulls, the ancient skulls had no noncarious cervical lesions. The reason ancient skulls were evaluated was to rule out the presence of a toothbrush abrasion cofactor. The use of toothbrushes by modern humans and chewsticks in ancient humans could not explain why ancient skulls had no such lesions.12 Based on this finding, oral hygiene technique, type of toothbrush, and abrasive index of dentifrices have been evaluated (and modified when needed) before lesions are treated. In addition, medication use or behavioral activities that produce xerostomia20,21 strongly influence biocorrosive actions on teeth (Figure 6). The 74-year-old male in Figure 6 was mainly affected by stress and biocorrosion conditions; it is unlikely friction from a toothbrush or dentifrice acted as a major factor for his noncarious cervical lesions.4,22,23 However, the lifespan of ancient populations was shorter than modern individuals and current diets have much greater content of exogenous biocorrosive agents.24
Careful diagnosis is the key to understanding noncarious cervical lesions and it begins with a thorough medical history. Since abrasion and, specifically, biocorrosion may be part of the multifactorial cause of these lesions, gastrointestinal reflux conditions, eating disorders, regurgitation, and diets containing acidic foods must be evaluated.25 Although bulimia mainly effects the lingual surfaces of teeth, it also provides many of the essential acids and proteolytic agents that contribute to endogenous biocorrosion.26

Modern lifestyle may also contribute to lesion formation. Diets high in acids or sweeteners can cause hypomineralization and lead to exogenous biocorrosive effects on the enamel, thereby causing white opacities in otherwise clear enamel. Research strongly implicates biocorrosive effects, as well as occlusal forces (such as bruxism or other forms of parafunction), in the formation of noncarious cervical lesions.5,27 Not all individuals who clench or brux develop lesions, however. When an attempt was made to associate bruxing with noncarious cervical lesions, it was concluded that dentin demineralization promotes lesion formation from an early stage. Although occlusal stress is an etiologic factor that contributes to the initiation and progression of lesions, biocorrosive cofactors cannot be controlled or removed in vivo. As noted earlier, the role of biocorrosion appears to be part of the multifactorial event that may not necessarily follow the classic stress-related abfractive process. Because noncarious cervical lesion formation cannot exist without biocorrosive influences, the effectiveness of occlusal adjustment alone as a preventive modality is not supported by current evidence.28
In a study of precontemporary Australian aborigines, a high prevalence of occlusal wear faceting was found. Given the presence of heavy occlusal loading in these individuals, one might expect to discover abfractions, yet no lesions were found. To what extent diet played in their occlusal wear was not determined.29
Abrasion from toothbrush use and cleaning habits must also be considered.20 Overzealous toothbrushing or improper brushing technique may very well be a contributing cofactor in hard tissue loss. Yet presumption that oral hygiene and dentifrice are strongly related to the etiological presence of noncarious cervical lesions is lacking adequate foundation.23 Toothbrushing in the presence of acid can contribute to a more rapid development of these lesions. The most noted etiologic factors are acidic biocorrosion and stress conditions. Preventive measures to reduce acid challenges on the teeth are essential to managing these patients.30 Occlusal parafunction is a possible involvement, as are oral habits.31 As more evidence comes to light, a multifactorial etiology becomes more and more complex.
OCCLUSAL CONSIDERATIONS
If there are occlusal considerations, clinicians should discuss splint therapy, bite guards, or determine force and timing values with their patients.32 An objective digital occlusal analysis alteration with the T-scan system to produce immediate complete anterior guidance development can be a useful methodology for producing objective physiologic force contacts and timing values of teeth, especially during horizontal movements of the mandible.32,33
A comprehensive treatment plan for noncarious cervical lesions in the esthetic zone should consider consultation with a periodontist to discuss the need for soft tissue grafting or coronally positioned flaps. In line with referral, the dentist should consider the type of restorative materials available to determine if they are tissue biocompatible. This is important because the periodontist will ultimately be covering the restorations with gingival soft tissue. In the case of caries, the use of restorations should be straightforward to avoid noncompatible materials. Based on abfractive consequences for an etiology of noncarious cervical lesions, restoration of these lesions has typically been with tooth-colored materials and nonobjectively measured occlusal adjustment. These lesions have undergone vigorous in vivo and in vitro research in an attempt to identify the most successful biocompatible restoration protocol.34,35
If all of the etiologic factors are not identified or considered when deciding how best to treat noncarious cervical lesions, continued progression will occur and the restorations will fail prematurely.36 Since there is no clinical evidence that restorative treatment alone is effective in impeding further development of lesions, restorations alone cannot be used as a preventive measure to stop their progression.
TREATMENT SUGGESTIONS
Allen and Winter37 and then Nascimento et al25 reiterated that restorative treatment of abfractive lesions (i.e., noncarious cervical lesions) should only be considered when one or more of the following conditions are present:
- Active, cavitated caries lesions in association with abfractive lesions; caries risk assessment must be conducted
- Cervical margins or all lesion margins are located subgingivally and preclude plaque control
- Extensive tooth structure loss or the defect is in close proximity to the pulp
- Persistent CDH or dentinal hypersensitivity
- When the tooth will be acting as a prosthetic abutment
- Esthetic requirements at the patient’s request
Both studies support an interdisciplinary approach whenever gingival recession is involved. A bottom-line approach was to attempt to achieve maximum esthetics, tooth form and function for vital pulp conditions.
Nearly all of the research on the relationship of occlusal forces (e.g., bruxing) to cervical lesions shows that teeth do indeed flex in the cervical region under excessive force loads, but no studies seem to cite actual damage caused by this deformation without an abrasive or biocorrosive component applied as well. Nevertheless, the abfractive consequences argument asserts that bruxing forces alone can cause the loss of cervical hard tissue of tooth structure. It is postulated that abfraction is responsible for chronic sensitivity of teeth to cold foods and liquids. This biomechanical theory implies that noncarious cervical lesions would tend to prematurely degrade after restoration, or result in additional occlusal disease due to constant deformation caused by occlusal parafunction or biocorrosion.5,16
Challenges in restoring noncarious cervical lesions include difficulties in obtaining moisture control, gaining access to subgingival margins, and high failure rates. Rubber dam clamps, gingival retraction cord and periodontal surgery are methods that can be used to control gingival tissue moisture and facilitate access. Other reasons for restoration failure include lack of retention, secondary caries, and marginal defects at the time of initial placement. Potential negative consequences include discoloration and prolonged tooth sensitivity.
There is also considerable evidence that amalgam and gold have little use in the modern-day restoration of noncarious cervical lesions. Clinical studies have shown that restoration of abfractive lesions has a high percentage of failure in the cervical margin region. Glass ionomer cement (GIC), resin-modified glass ionomer (RMGI), GIC/RMGI liner/base laminated with a resin composite, and resin composites in combination with a dentin bonding agent are all possible restorative options. A restorative material such as a self-adhering resin ionomer can be ideal for restoring lesions because of its high tissue compatibility. It must be noted that microfilled composites demonstrate greater elasticity than hybrid composites that can allow comparable flexure to dentin or enamel under applied stress from abfraction.
SUMMARY
In conclusion, inasmuch as the treatment of periodontal disease often requires a multifaceted approach, current evidence supports a multifactorial etiologic determination for these lesions. An understanding that abfractive effects to hard tissue from stress is only one factor in the development of lesions is crucial. The etiology of noncarious cervical lesions often remains misunderstood, and more research is needed to fully understand this fascinating and frequently encountered condition.
Anthropological, epidemiological, theoretical, experimental and clinical studies suggest noncarious cervical lesions should not be considered a manifestation of stress alone, but, rather, result from a combination of mechanisms. If occlusal forces are considered to be a dominant factor in the etiology, occlusal diagnosis and modification should be considered.38 Dentists should turn to the scientific evidence to determine the best options for treatment and arresting further progression. All evidence points to a multifactorial etiology, with emphasis related just not to occlusal factors, but also the effects of biocorrosion and friction.5,23
KEY TAKEAWAYS
- Careful diagnosis is the key to understanding noncarious cervical lesions and it begins with a thorough medical history.
- Current understanding is the etiology of abfractions — a form of noncarious cervical lesions — is due to occlusal forces.2
- Research indicates the cause is not occlusal factors alone, but, rather, multifactorial — especially involving biocorrosion in combination with cervical stress stemming from hyperfunctional or parafunctional occlusal forces.
- Biocorrosion includes the progressive loss of tooth structure through chemical processes that could also involve bacterial action. It replaces former terms corrosion, erosion and others relating to hard tissue degradation.
- Because noncarious cervical lesion formation cannot exist without biocorrosive influences, the effectiveness of occlusal adjustment alone as a preventive modality is not supported by current evidence.28
- Since there is no clinical evidence that restorative treatment alone is effective in impeding further development of lesions, restorations alone cannot be used as a preventive measure to stop their progression.
- As additional evidence comes to light, the multifactorial etiology of these lesions becomes more and more complex.
REFERENCES
- Miller N, Penaud J, Ambrosini P, Bisson-Boutelliez C, Briançon S. Analysis of etiologic factors and periodontal conditions involved with 309 abfractions. J Clin Periodontol. 2003;30:828–832.
- Grippo JO. Abfractions: a new classification of hard tissue lesions of teeth. J Esthet Dent. 1991;3:14–19.
- Bartlett DW, Shah P. A critical review of non-carious cervical (wear) lesions and the role of abfraction, erosion, and abrasion. J Dent Res. 2006;85:306–312.
- Grippo JO, Simring M, Coleman TA. Abfraction, abrasion, biocorrosion, and the enigma of noncarious cervical lesions: a 20-year perspective. J Esthet Restor Dent. 2011;24:10–23.
- Yang J, Cai D, Wang F, et al. Non-carious cervical lesions (NCCLs) in a random sampling community population and the association of NCCLs with occlusive wear. J Oral Rehabil. 2016;43:960–966.
- Borcic J, Anic I, Urek MM, Ferreri S. The prevalence of non-carious cervical lesions in permanent dentition. J Oral Rehabil. 2004;31:117–123.
- Terry DA. Cervical dentin hypersensitivity: etiology, diagnosis, and management. Dent Today. 2011;30:61–62,64,68 passim;quiz 70.
- Miller WD. Experiments and observations on the wasting of tooth tissue variously designated as erosion, abrasion, chemical abrasion, denudation, etc. Dent Cosmos. 1907;49:1–23.
- Rees JS. The effect of variation in occlusal loading on the development of abfraction lesions: a finite element study. J Oral Rehabil. 2002;29:188–193.
- Sarode G, Sarode S. Abfraction: a review. J Oral Maxillofac Pathol. 2013;17:222–227.
- Grippo JO. Biocorrosion vs. erosion: the 21st century and a time to change. Compend Contin Educ Dent. 2012;33:e33–e37.
- Aaron GM. The Prevalence of Noncarious Cervical Lesions in Modern and Ancient American Skulls: Lack of Evidence for an Occlusal Etiology. Available at: http://ufdc.ufl.edu/UFE0004872/00001. Accessed October 11, 2018.
- Lee WC, Eakle WS. Possible role of tensile-stress in the etiology of cervical erosive lesions of teeth. J Prosthet Dent. 1984;52:374–380.
- Lussi A, Jaeggi T. Dental Erosion: Diagnosis, Risk Assessment, Prevention, and Treatment. Hanover Park, Illinois: Quintessence Publishing; 2011.
- Xhonga FA. Bruxism and its effect on the teeth. J Oral Rehabil. 1977;4:65–76.
- Coleman TA, Grippo JO, Kinderknecht KE. Cervical dentin hypersensitivity, Part II: associations with abfractive lesions. Quintessence Int. 2000;31:466–473.
- Coleman TA, Grippo JO, Kinderknecht KE. Cervical dentin hypersensitivity. Part III: resolution following occlusal equilibration. Quintessence Int. 2003;34:427–434.
- Sawlani K, Lawson NC, Burgess JO, et al. Factors influencing the progression of noncarious cervical lesions: a 5-year prospective clinical evaluation. J Prosthet Dent. 2016;115:571–577.
- Grippo JO, Coleman TA, Messina AM, Oh DS. A literature review and hypothesis for the etiologies of cervical and root caries. J Esthet Restor Dent. 2018;30:187–192.
- Zero DT. Etiology of dental erosion — extrinsic factors. Eur J Oral Sci. 1996;104:162–177.
- Litonjua LA, Andreana S, Bush PJ, Tobias TS, Cohen RE. Noncarious cervical lesions and abfractions — A re-evaluation. J Am Dent Assoc. 2003;134:845–850.
- Tellefsen G, Liljeborg A, Johannsen A, Johannsen G. The role of the toothbrush in the abrasion process. Int J Dent Hyg. 2011;9:284–290.
- Faye B, Kane AW, Sarr M, Lo C, Ritter AV, Grippo JO. Noncarious cervical lesions among a non-toothbrushing population with Hansen’s disease (leprosy): initial findings. Quintessence Int. 2006;37:613–619.
- Brandini DA, de Sousa AL, Trevisan CL, et al. Noncarious cervical lesions and their association with toothbrushing practices: in vivo evaluation. Oper Dent. 2011;36:581–589.
- Nascimento MM, Dilbone D, Pereira P, Duarte WR, Geraldeli S, Delgado A. Abfraction lesions: etiology, diagnosis, and treatment options. Clin Cosmet Investig Dent. 2016;8:79–87.
- Ranjitkar S, Kaidonis JA, Smales RJ. Gastroesophageal reflux disease and tooth erosion. Int J Dent. 2012;2012:1–10.
- Grippo JO, Simring M, Schreiner S. Attrition, abrasion, corrosion and abfraction revisited. J Am Dent Assoc. 2004;135:1109–1118.
- Wood I, Jawad Z, Paisley C, Brunton P. Non-carious cervical tooth surface loss: a literature review. J Dent. 2008;36:759–766.
- Kaidonis JA, Richards LC, Townsend GC. Nature and frequency of dental wear facets in an Australian Aboriginal population. J Oral Rehabil. 1993;20:333–340.
- Michael JA, Townsend GC, Greenwood LF, Kaidonis JA. Abfraction: separating fact from fiction. Aust Dent J. 2009;54:2–8.
- Piotrowski BT, Gillette WB, Hancock EB. Examining the prevalence and characteristics of abfractionlike cervical lesions in a population of U.S. veterans. J Am Dent Assoc. 2001;132:1694–1701.
- Kerstein RB. Disocclusion time-reduction therapy with immediate complete anterior guidance development to treat chronic myofascial pain-dysfunction syndrome. Quintessence Int. 1992;23:735–747.
- Klein M. A comparison of ICAGD (immediate complete anterior guidance development) to mock ICAGD for symptom reductions in chronic myofascial pain dysfunction patients. Cranio. 1997;15:21–37.
- Perez Cdos R, Gonzalez MR, Prado NA, de Miranda MS, Macêdo Mde A, Fernandes BM. Restoration of noncarious cervical lesions: when, why, and how. Int J Dent. 2012;2012:1–8.
- Peumans M, De Munck J, Van Landuyt KL, et al. Restoring cervical lesions with flexible composites. Dent Mater. 2007;23:749–754.
- Heymann HO, Sturdevant JR, Bayne S, Wilder AD, Sluder TB, Brunson WD. Examining tooth flexure effects on cervical restorations: a two-year clinical study. J Am Dent Assoc. 1991;122:41–47.
- Allen EP, Winter RR. Interdisciplinary treatment of cervical lesions. Compend Contin Educ Dent. 2011;32 Spec No 5:16–20.
- Silva AG, Martins CC, Zina LG, et al. The association between occlusal factors and noncarious cervical lesions: a systematic review. J Dent. 2013;41:9–16.
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. November 2018;4(11):10, 12–14,17.
