
 ROSSHELEN / ISTOCK / GETTY IMAGES PLUS
ROSSHELEN / ISTOCK / GETTY IMAGES PLUS
Motivational Interviewing: Dentists’ Role in Patient Behavior Change
Applying the principles of motivational interviewing can help guide improvements in patients’ oral health.
PURCHASE COURSE
This course was published in the April 2022 issue and expires April 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the April 2022 issue and expires April 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the use of motivational interviewing as a tool for affecting behavioral changes designed to improve patients’ oral and systemic health.
- Explain the strategies, stages and challenges involved in positive behavior change.
- Discuss the application and benefits of motivational interviewing techniques in the dental setting.
Effective communication is a key aspect to improve patient outcomes and satisfaction in oral healthcare. Dentists have the communication skills and training to clearly explain the diagnosis, treatment plan, and expected outcome of therapy. Additionally, appropriate patient education can help reduce the risk of oral disease. In these efforts, patient education using evidence-based models to support behavior change is critical because oral diseases can be prevented or reduced through lifestyle or behavioral changes. However, there is a complex relationship between a patient’s lifestyle and the behavior change process. The clinical need to help affect positive behavioral changes led to the development of the motivational interviewing (MI) technique.
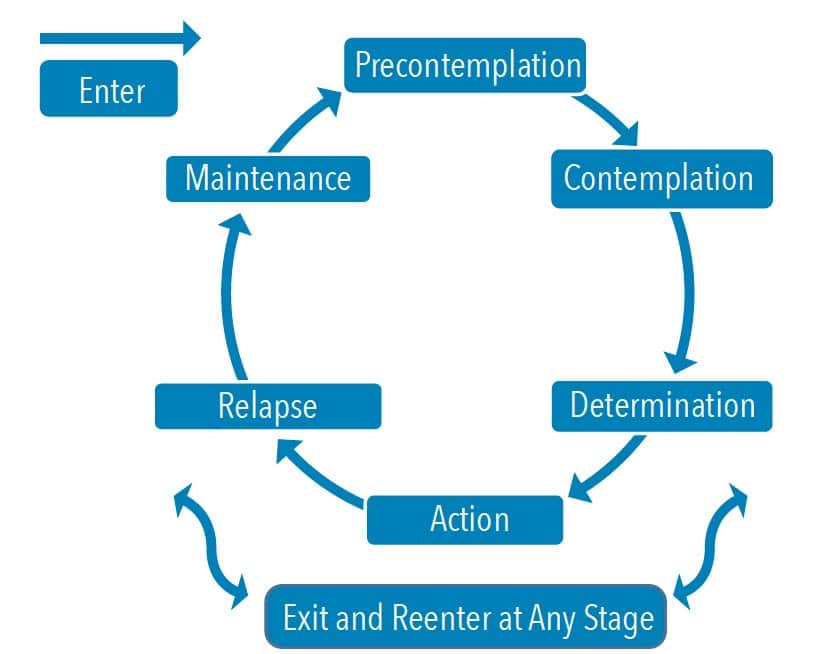
The complexity of individual behavior change and the decision-making process are described by the transtheoretical model, also known as the stages of change.1 This model acknowledges that most individuals are indecisive about changing their behavior, and when they decide to make a change, it does not occur quickly.1 Behavior change is a process involving six stages: precontemplation, contemplation, determination, action, relapse, and maintenance (Figure 1).
During the precontemplation stage, patients neither believe their behavior has an impact on health, nor are they planning to change a behavior.1 The contemplation stage is when patients have some awareness that behavior has consequences on their health. During this stage, an individual has ambivalence to change, which means he or she is debating the advantages and disadvantages of the behavior change.1 The determination stage is when the individual has made a commitment to make a positive change.1 The action stage occurs when the individual believes he or she has the ability to change, and is taking actions to change a behavior that impacts health.1 Some individuals may relapse by resorting to prior behaviors. The relapse stage may be part of the process for some, but not all. Individuals who do not relapse will move into the next phase of maintenance.1 In this phase, an individual is able to resist temptations of prior poor behaviors that had a negative impact on health and well-being.1 These individuals also appreciate the actions taken to get this far. After all, a lifelong behavior change takes time and work.
Historically, patient education encompasses information given by the oral healthcare professional in the form of “tell-show-do.” However, evidence-based behavioral science research indicates advice-giving methods do not support a behavior change, and may hinder the behavior change process.2,3 In fact, patients are more likely to change a behavior that negatively impacts their health when they are intrinsically motivated to make a change.2,4 The evidence in the literature is shifting from traditional patient education to the delivery of patient-centered counseling.2–8
As a collaborative, patient-centered counseling approach, MI supports positive behavior change.2 The role of the clinician is to evoke the patient’s intrinsic motivation for a positive behavior change, and initiate change conversations.2,9 An entire MI-trained team that applies this technique’s principles, rules and guiding strategies will provide consistent educational messaging in the clinic.
INTEGRATED COMPONENTS
Practicing MI during patient care encompasses a philosophy known as the “spirit of MI.” This has four integrated components designed to build rapport and trust to support patient autonomy. These include collaboration, compassion, acceptance and evocation.2 For a clinician to demonstrate this philosophy, there must be a collaborative partnership with the patient, and the demonstration of compassion from the clinician to actively promote the patient’s well-being and give priority to the individual’s needs.2,9 In addition, the provider will have an attitude of acceptance. This does not mean the operator must agree with the patient’s choices, but the clinician cannot judge the patient for their choices.2,9 Lastly, evocation is drawing out the patient’s own thoughts or ideas, rather than the clinician imposing his or her own goals or expectations.2,9
Behavior change therapy has been used in medicine for almost 40 years, including, but not limited to, addiction therapy, weight loss management for diabetes, and tobacco cessation.10–13 As a communication approach for supporting behavior change, MI has been used in dentistry over the last decade.3,5,6,8,14–16 In the dental setting, MI has been successful in reducing behaviors that increase the risk for caries, periodontal disease and oral cancers.3,5,6,17 However, time constraints are often cited in the literature as a barrier to implementing the MI technique.7,8,14,16
Due to limited time during a dental appointment, a derivative of MI — brief MI (BMI) — has been successful for clinicians with limited time (5 to 10 minutes) to support a patient’s behavior change.9,18,19 Essentially, BMI encompasses the spirit of MI to identify the patient’s readiness to change, assess motives, and help overcome ambivalence to change.9,18,19
PRINCIPLES BEHIND THE TECHNIQUE
The four main principles of MI include empathy, discrepancy, roll with resistance, and support self-efficacy. These four principles promote patient autonomy during the behavior change process. Empathy focuses on a clinician’s ability to show interest in understanding the patient’s perception.9 The discrepancy principle focuses on distinguishing between the patient’s values and behaviors that are inconsistent with behavior change goals.9 Rolling with resistance, which may also be referred to as avoiding conflict, may minimize a patient’s ambivalence and provide valuable insight into the patient’s internal challenges.9 Self-efficacy is offering encouragement and praise to build confidence in the patient’s ability to change a behavior.9 The principles of MI can be especially useful for patients in the precontemplation stage, when they have no belief their current behaviors are negatively impacting oral and/or systemic health. They are also fundamental for patients in the contemplation stage to assist in overcoming their ambivalence of change. 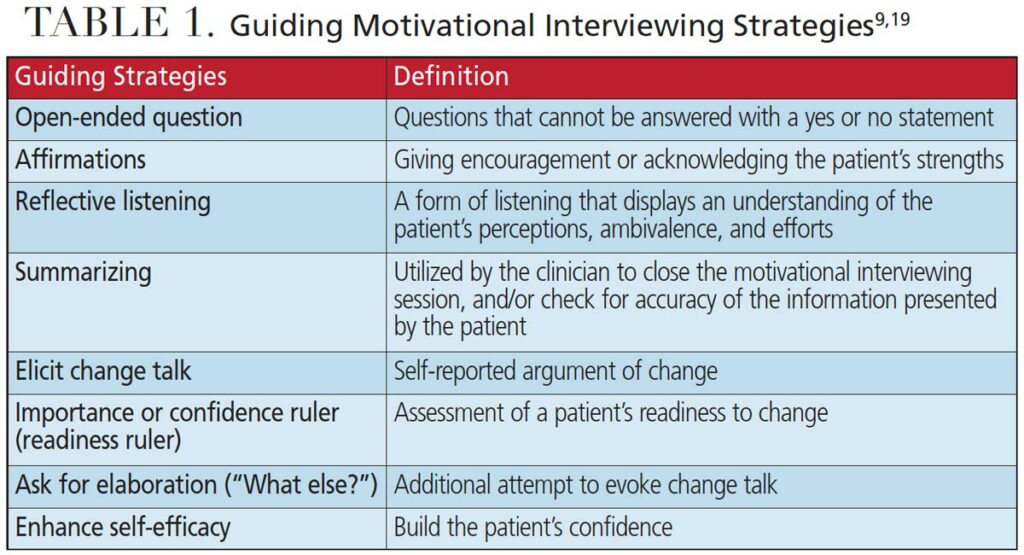
GUIDING STRATEGIES
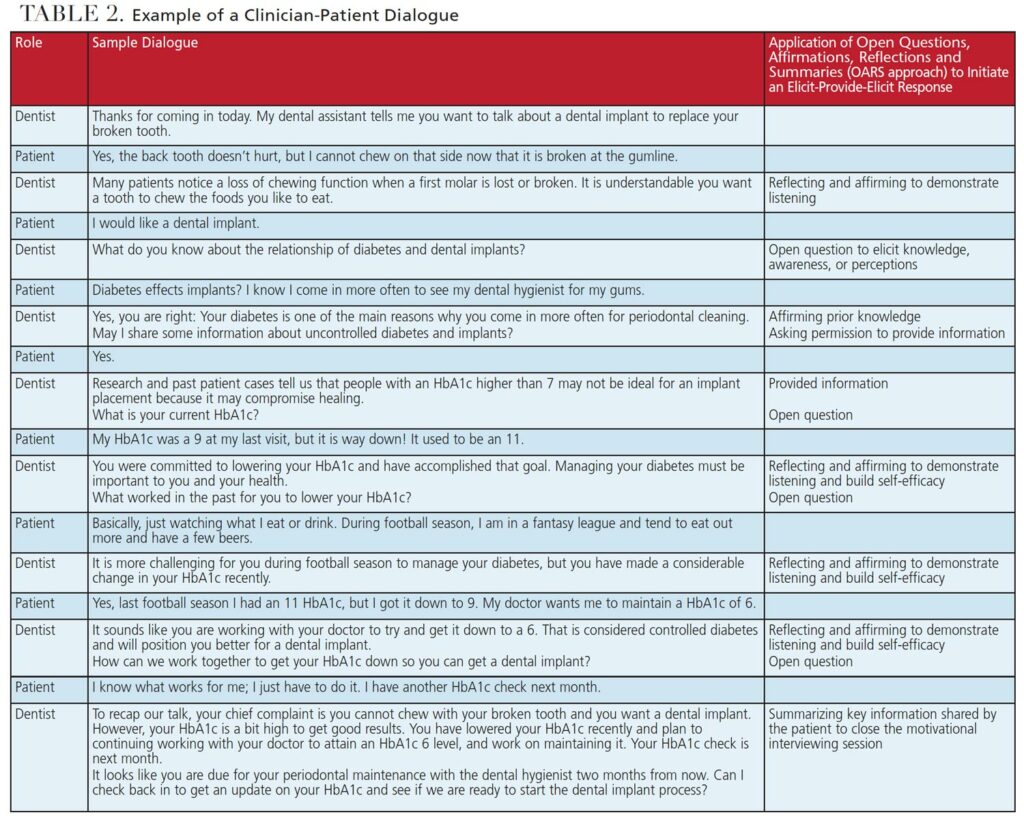
There are eight MI strategies to evoke a positive behavior change and enhance the clinician’s ability to support patient autonomy (Table 1).2,9 Of these guiding strategies, dentists who are beginning to apply BMI during patient-centered counseling may want to focus on OARS — an acronym that represents open questions, affirmations, reflections and summaries.4,18 Open-ended questions are those that cannot be answered with a “yes or no” statement. Posing questions that provide an opportunity to craft a response will allow the clinician to understand the patient’s perception. Affirmations are achieved by offering encouragement and acknowledgment of the patient’s strengths.2,9 Reflections allow a clinician to display an understanding of the patient’s perceptions, ambivalence and efforts.2,9 Reflections also help accomplish two goals:
- The patient can hear his or her own statements of thoughts and feelings, as paraphrased by the clinician
- It gives the patient an opportunity to make corrections if the clinician does not demonstrate an accurate understanding of the patient’s perceptions, ambivalence and efforts
The purpose of summaries is to close the MI session by ensuring the clinician understands the patient’s perspective and connects the information provided.2,9 Although all eight MI strategies are useful, practicing BMI with the application of OARS is helpful for clinicians with limited time to support positive behavior change.
RULES OF MOTIVATIONAL INTERVIEWING
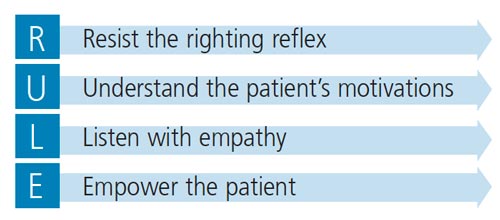
There are also rules to follow that align with MI principles (Figure 2). For example, resisting the righting reflex means clinicians do not “fix” or “change” the behavior impacting the patient’s health and well-being.2,9 The role of the clinician is to evoke and initiate change conversations that prompt the patient to take ownership of his or her health. The clinician also needs to understand the patient’s motivations, perceptions of change, or perceptions of the challenges to change.2,9 When the provider has a better understanding of what motivates the patient, the clinician is more likely to provide support and demonstrate acceptance for the patient’s challenges. Listen with empathy is the next rule. This aligns with the spirit of MI to demonstrate compassion for the patient.2,9 The goal is to empower the patient to build self-efficacy for change. Individuals are more likely to be motivated by their own ideas than a clinician telling them what to do; in this context, following the MI rules is essential.
DEVELOPING TRUST AND RAPPORT
The MI process comes full circle when there is trust and rapport between the patient and clinician. The process includes engaging, focusing, evoking and planning.2,9 Engaging the patient means focusing on a specific behavior by evoking the individual’s intrinsic motivation, and then supporting plans to change the negative behavior that is impacting health.2,9 Engaging and focusing will evoke a patient’s motivation to move from the contemplation to determination stage, as this will elicit the individual’s internal motivation to change. The last step is planning, which occurs when the patient has reached the level of readiness to change a behavior and is in the determination stage.2,9 This requires a commitment and an action plan that may need to be revisited multiple times as the behavior change evolves, or if the patient relapses.
ELICIT-PROVIDE-ELICIT
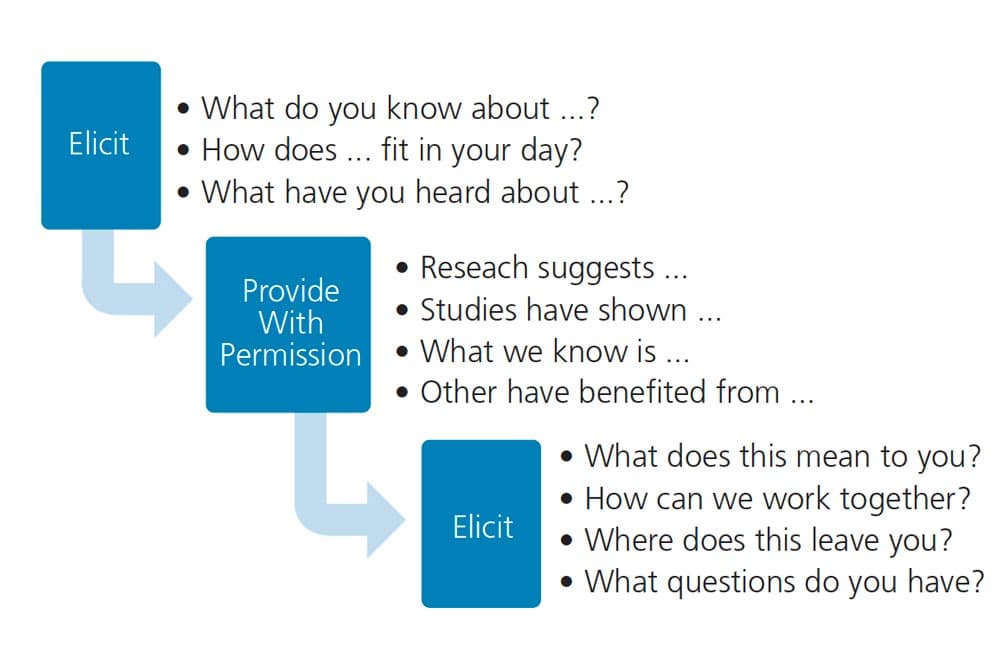
The elicit-provide-elicit (E-P-E) approach enhances the clinician’s ability to understand the patient’s awareness of behavioral impacts on health, provide information, and elicit the individual’s motivation and readiness for change.2,20,21 The first step is to elicit what the patient already knows by asking evocative, open-ended questions.2,20,21 The patient’s response to an open-ended question allows the clinician to understand the patient’s awareness and knowledge. The next step is to ask permission to provide information. The last step is to elicit a second time by posing another open-ended question to explore the patient’s reactions, questions, or next steps on how change will fit into the patient’s life.20,21
When faced with time constraints, the E-P-E technique is extremely useful for providing information, filling in gaps, or correcting misconceptions. This is a time-saving strategy that validates patient knowledge, supports patient autonomy, and allows time to address barriers. Clinicians should be aware they are unlikely to move a patient through the stages of change in one dental appointment. The E-P-E approach allows dentists to apply the spirit of MI to develop a partnership that supports the patient through the stages of change. Figure 3 provides examples of open-ended questions to elicit patient awareness, statements to provide information, and open-ended questions to assess the individual’s reaction or next steps.
WHERE DO DENTISTS START?
Seeking continuing education on MI is a starting point for dentists and their teams. The Motivational Interviewing Network of Trainers is a helpful resource for those interested in incorporating MI into practice.22 Dentists can find a list of training events in-person and online. The network offers continuing education, resources, publications, and practice opportunities for healthcare professionals.22
Additionally, online resources are available through Rollnick23 and Psychwire.24 On his website, Rollnick — a cofounder of MI — offers online courses, webinars, consulting, mentoring and books.23 Psychwire provides courses from the founders of MI (Miller and Rollnick) and other experts.24 There are also free short videos that dentists and their allied oral health professional team can view. These video clips provide helpful information on MI, the process, the righting reflex, change talk, and ambivalence.25 It is important for dentists to realize that training is essential in order to effectively implement BMI into practice. The combination of MI knowledge and clinical application training (that includes coaching, role-playing and feedback) supports the effective use of this technique.7,8,10,14
CONCLUSION
When properly utilized, both MI and BMI can be effective communication tools for dental teams to motivate patients and improve their oral health by encouraging healthy behavioral changes. These techniques cultivate a safe environment for patients to discuss their concerns and ambivalence about changing current behaviors. Although MI has proven beneficial in patient management, due to time constraints in practice, BMI — with the application of OARS delivered via E-P-E — is an optimal approach to support positive behavior change.
Incorporating MI into everyday practice is an easy, supportive and meaningful way to involve patients in treatment decisions and motivate them to make healthier decisions to improve oral and systemic health.
BONUS WEB CONTENT
REFERENCES
- Prochaska JO, DiClemente CC. Transtheoretical therapy: Toward a more integrative model of change. Psychol Psychother. 1982;19:276–288.
- Miller RW, Rollnick S. Motivational Interviewing Helps People Change. 3rd ed. New York: Guilford Press; 2013:484.
- Brand VS, Bray KK, MacNeill S, Catley D, Williams K. Impact of single-session motivational interviewing on clinical outcomes following periodontal maintenance therapy. Int J Dent Hyg. 2013;11:134–141.
- Rollnick S, Mason P, Butler C. Health Behavior Change: A Guide for Practitioners. Edinburgh: Churchill Livingstone; 1999:225.
- Hirsch GB, Edelstein BL, Frosh M, Anselmo T. A simulation model for designing effective interventions in early childhood caries. Prev Chronic Dis. 2012;9:E66.
- Gao X, Lo ECM, Kot SCC, Chan KCW. Motivational interviewing in improving oral health: a systematic review of randomized controlled trials. J Periodontol. 2014;85:426–437.
- Croffoot C, Krust Bray K, Black MA, Koerber A. Evaluating the effects of coaching to improve motivational interviewing skills of dental hygiene students. J Dent Hyg. 2010;84:57–64.
- Arnett M, Korte D, Richards P, et al. Effect of faculty development activities on dental hygiene faculty perceptions of and teaching about motivational interviewing: a pilot study. J Dent Educ. 2017;81:969–977.
- Catley D, Goggin K, Lynam I. Motivational interviewing (MI) and its basic tools. In: Ramseier CA, Suvan JE, eds. Health Behavior Change in the Dental Practice. Ames, Iowa: Wiley-Blackwell; 2010:59–92.
- Miller WR, Yahne CE, Moyers TB, Martinez J, Pirritano M. A randomized trial of methods to help clinicians learn motivational interviewing. J Consult Clin Psychol. 2004;72:1050–1062.
- Edwards EJ, Stapleton P, Williams K, Ball L. Building skills, knowledge, and confidence in eating and exercise behavior change: Brief motivational interviewing training for healthcare providers. Patient Educ Couns. 2015;98:674–676.
- Ekong G, Kavookjian J. Motivational interviewing and outcomes in adults with type 2 diabetes: A systematic review. Patient Educ Couns. 2016;99:944–952.
- Poirier MK, Clark MM, Cerhan JH, et al. Teaching motivational interviewing to first-year medical students to improve counseling skills in health behavior change. Mayo Clin Proc. 2004;79:327–331.
- Mills A, Kerschbaum WE, Richards PS, Czarnecki GA, Kinney JS, Gwozdek AE. Dental hygiene students’ perceptions of importance and confidence in applying motivational interviewing during patient care. J Dent Hyg. 2017;91:15–23.
- Bray KK, Bennett K, Catley D. Fidelity of motivational interviewing training for dental hygiene students. J Dent Educ. 2021;85:287–292.
- Bray KK, Catley D, Voelker MA, Liston R, Williams KB. Motivational interviewing in dental hygiene education: curriculum modification and evaluation. J Dent Educ. 2013;77:1662–1669.
- Walker KK, Jackson RD, Sommariva S, Neelamegam M, Desch J. USA dental health providers’ role in HPV vaccine communication and HPV-OPC protection: a systematic review. Hum Vaccin Immunother. 2019;15:1863–1869.
- Gillam DG, Yusuf H. Brief motivational interviewing in dental practice. Dent J (Basel). 2019;7:51.
- Koeber A. Brief interventions in promoting health behavior change. In: Ramseier CA, Suvan JE, eds. Health Behavior Change in Dental Practice. Ames, Iowa: Wiley-Blackwell; 2010:93–112.
- Wyatt J, Singer A. Clinical Conversations About Cannabis: Using Elicit-Provide-Elicit. Available at: https://attcnetwork.org/centers/ attc-network-coordinating-office/attc-messenger-june-2015-clinical-conversations-about. Accessed March 9, 2022.
- Suvan J, Fundak A, Gobat N. Implementaion of health behavior change principles in dental practice. In: Ramseier CA, Suvan JE, eds. Health Behavior Change in Dental Practice. Ames, Iowa: Wiley-Blackwell; 2010:113–144.
- About MINT: Motivational Interviewing Network of Trainers. Available at: https://motivationalinterviewing.org/about_mint. Accessed March 9, 2022.
- Stephen Rollnick Trainer Consultant Author and Co-Founder of Motivational Interviewing. Available at: https://www.stephenrollnick.com/. Accessed March 9, 2022.
- Psychwire. William Miller, Stephen Rollnick and Theresa Moyers Teach Motivational Interviewing. Available at: https://psychwire.com/motivational-interviewing. Accessed March 9, 2022.
- Psychwire. Resources Motivational Interviewing. Available at: https://psychwire.com/motivational-interviewing/resources. Accessed March 9, 2022.
From Decisions in Dentistry. April 2022;8(4)40-43.

