

Maxillary Sinusitis of Endodontic Origin
Endodontic infections can spread into the maxillary sinuses, causing pathology and radiographic presentations that are often unrecognized in clinical practice. Here are insights into diagnosing and managing these cases.
Endodontic infections can spread into the maxillary sinuses, causing pathology and radiographic presentations that are often unrecognized in clinical practice. Here are insights into diagnosing and managing these cases
Endodontic disease is characterized by pulpal bacterial infection and subsequent inflammatory response in the adjacent periapical tissues. Throughout the dentition, the root apices are typically surrounded by alveolar bone, and classical study of endodontic inflammatory processes thus focuses on the clinical, radiographic and histopathologic effects of endodontic disease on osseous tissues. In the maxillary posterior dentition, however, the dental root apices are often directly adjacent to the maxillary sinus floor and respiratory mucosa. Endodontic infections that develop in these teeth can easily spread into the maxillary sinuses, causing unique pathological effects and radiographic appearances that are often unrecognized in clinical practice. Failure to diagnose or properly manage endodontic infections in this region can lead to unresolved chronic sinus disease and impairment for these patients.
First referred to in 1943 as maxillary sinusitis of dental origin,1 the relationship between dental infections and sinus disease is well documented in the dental and medical literature. Numerous investigators since have discovered this condition, also termed odontogenic sinusitis, is a common disease process,2–14 with sinus mucosal inflammation seen in 60% to 80% of patients with infections originating in the maxillary posterior teeth.2–4 The literature also indicates that more than 40% of maxillary sinusitis cases have an odontogenic etiology,5–8 increasing to more than 70% when maxillary sinus infections are unilateral.9,10
Despite its prevalence, odontogenic sinusitis is frequently unrecognized by dentists, radiologists and ear, nose and throat (ENT) specialists, with its sequelae often misdiagnosed as sinogenic sinusitis.7,11,13 Studies show that during routine general examinations, dentists using periapical radiographs failed to diagnose odontogenic sinusitis in up to 86% of cases.9,11
Maxillary sinusitis of dental origin (or odontogenic sinusitis) is a broad term used to describe any degree of sinus infection and symptoms caused by multiple dental etiologies, including periodontal or endodontic disease, root fractures, dental implants, extractions, oralantral fistulae, and iatrogenic causes, such as extruded dental materials, displaced teeth or foreign bodies.2,12,14,15 While these can all be odontogenic sources for sinusitis, it is important to distinguish these etiologies from maxillary sinusitis of endodontic origin (MSEO), as they have a different pathogenesis and require markedly different treatment. Clinically, MSEO refers specifically to sinusitis caused by endodontic infection, excluding sinusitis secondary to other dental etiologies.
Being able to recognize MSEO is important, as failure to identify and properly manage the endodontic source pathology will result in the persistence of sinus disease and failure of medical sinus therapies. If left undiagnosed, patients often experience chronic sinus infections, ineffectual antibiotic regimens, and may even undergo multiple sinus surgeries — never realizing that an endodontic infection is the source. This condition also has the potential to advance to more serious or even life-threatening craniofacial infections. In these severe and rare cases, dental infection can spread via the maxillary sinus, causing orbital cellulitis, blindness, meningitis, subdural empyema, brain abscess and life-threatening cavernous sinus thrombosis.4,16,17
DIAGNOSIS
Patient Symptoms: Diagnosing MSEO can be challenging because patients with this condition experience a wide variation of dental and sinonasal symptoms (including no symptoms). Typical endodontic symptoms are often not present with MSEO. For example, thermal pain is usually absent because source teeth for MSEO are most often necrotic or have failing endodontic therapy. Percussion tenderness is typically absent in MSEO because periapical infection is essentially draining into the sinus, eliminating pressure. For this same reason, swelling or intraoral sinus tracts rarely form.
Patients with MSEO will often experience common sinonasal symptoms, which include congestion, rhinorrhea, retrorhinorrhea, facial pain and foul odor.18,19 Individuals with sinonasal symptoms and without localized dental pain will typically seek care initially from a primary care physician or ENT specialist, who may misdiagnose and treat MSEO as a primary sinus infection because a dental source is often overlooked during routine ENT examinations.7,11,19 In addition, current ENT clinical guidelines for the medical management of rhinosinusitis offer no guidance in this area, and do not mention dental infections as a potential cause of sinusitis.20 The American Association of Endodontists (AAE) recently published a position statement on MSEO to raise awareness of this condition in the dental and medical communities.21 Dentists should keep sinonasal disease in mind when examining any dental infection in the posterior maxilla and rely on their local endodontists, who work closely with ENT specialists to diagnose MSEO and distinguish it from sinogenic sinusitis.
Radiographic Examination: While periapical radiographs are the most widely used imaging modality in endodontics, the posterior maxilla presents significant and unique interpretation challenges when using conventional two-dimensional imaging. Anatomic structures — such as the zygoma, palatal process, maxillary sinus and buccal cortical plate — are often superimposed onto the dental roots, obscuring or concealing periapical infection. Conventional periapical radiographs also do not consistently reveal mucosal thickening or fluid in sinuses, which are of important diagnostic value in MSEO.
Limited-field cone beam computed tomography (CBCT) imaging has been shown to significantly improve the ability to detect odontogenic sources for sinusitis. In a study by Low et al,22 CBCT revealed 34% more lesions than periapical radiography, as well as significantly more expansion of lesions into the maxillary sinus, mucosal thickening, and untreated canals. Mucosal changes associated with dental infections were reported to have a 77% prevalence, compared to the 19% detected using conventional radiographs. Throughout the dentition, endodontic disease typically manifests radiographically as distinct periradicular radiolucent lesions or thickening of the periodontal ligament. The radiographic appearance of endodontic disease on sinus tissues, however, is markedly different.23,24 Two unique radiographic findings associated with periradicular inflammation of the sinus mucoperiosteum are periapical osteoperiostitis (PAO) and periapical mucositis (PAM). Further progression of the disease process can cause a partial or total sinus obstruction.
PERIAPICAL OSTEOPERIOSTITIS
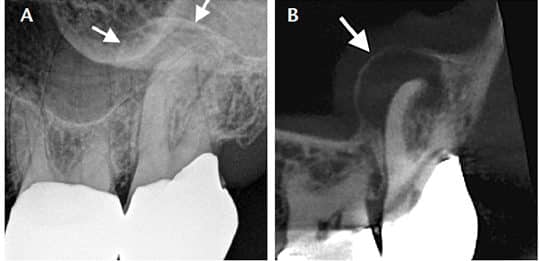
The presence of apical periodontitis adjacent to the maxillary sinus cortical floor will often expand the sinus periosteum, displacing it upward into the sinus, and subsequently inducing a periosteal reaction that continues to deposit a thin layer of new bone on the inner periphery of the periosteum. This reactive osteogenesis (i.e., PAO) forms a thin, hard-tissue dome on the sinus floor and presents on conventional radiographs and CBCT imaging as a radiopaque “halo” appearance (Figures 1A and 1B).24 The lesions may or may not be symptomatic, and may be accompanied by varying degrees of adjacent mucosal edema and sinus fluid levels.
PERIAPICAL MUCOSITIS
Symptomatic or asymptomatic apical periodontitis near or in direct contact with antral mucosa will typically produce a localized mucosal tissue edema (i.e., PAM), which appears radiographically as a mucosal thickening or dome-shaped soft tissue expansion in the floor of the sinus (Figures 2A through 2D). Often no evident osseous destruction or PAO halo occurs, making PAM more difficult to recognize radiographically as having an endodontic source. Mucosal edema on the sinus floor, and particularly dome-shaped mucosal swellings directly over dental root apices, should raise the suspicion of a dental etiology. Clinicians should be mindful, however, that PAM may have a similar appearance to mucous retention cysts, antral polyps, mucosal thickening caused by periodontal disease, and sinogenic mucosal thickening. As with all endodontic diagnoses, a determination of etiology cannot be made based on radiographic examination alone. Careful endodontic clinical examination of pulpal status is imperative to distinguish PAM from other mucosal abnormalities.
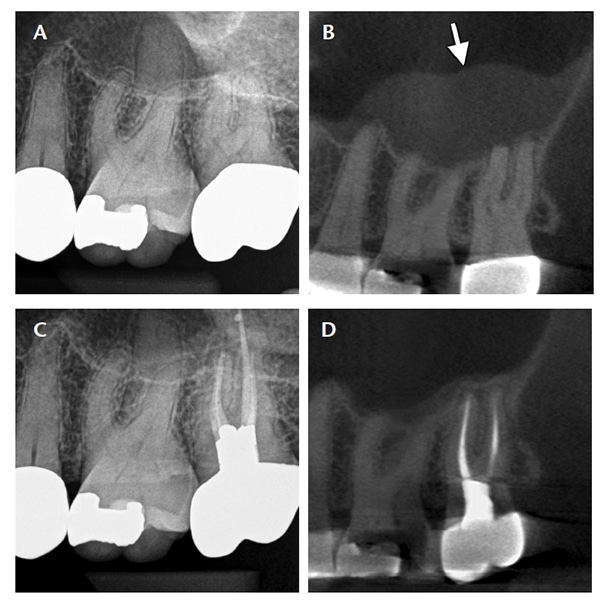
following endodontic treatment of the second molar (C). A six-month postoperative CBCT image shows resolution of the mucositis and reestablishment of the sinus cortical floor (D).
SINUS OBSTRUCTION
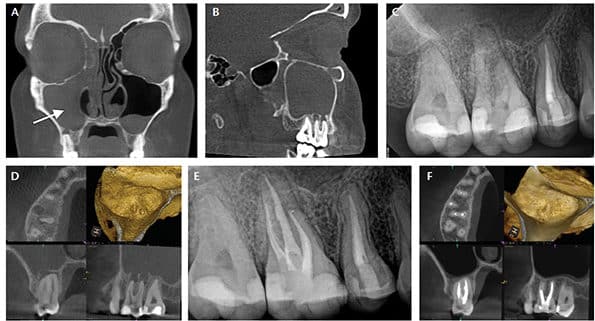
Mucosal edema caused by periapical infection may progress and occlude the entire maxillary sinus or advance further to involve other paranasal sinuses. Sinus obstructions cannot be determined with periapical radiographs, but are easily seen on large-field sinus CBCT imaging (Figures 3A through 3F). Even with three-dimensional radiography, however, sinus obstructions may be difficult to recognize as having an endodontic etiology. Careful radiographic examination for evidence of PAO is helpful in making this determination — but, as seen with PAM lesions, periapical radiolucencies or osseous changes do not always exist. A history of unilateral sinus obstruction, particularly if recurrent and/or associated with a patent ostium, is a strong indicator for possible MSEO.
CLINICAL EXAMINATION
A thorough clinical endodontic examination is essential for diagnosing or ruling out a potential endodontic source.13 When diagnosing a possible endodontic etiology in patients with sinusitis, the clinician must look carefully for any teeth with pulpal necrosis, and evaluate all prior endodontic treatments for possible failure in the suspected quadrant. Because MSEO is a bacterial disease, typically only teeth with an infected necrotic pulp or failing endodontic treatment will cause significant sinonasal disease or sinonasal symptoms. When examining maxillary posterior teeth with existing root canal treatment, providers must carefully look for any untreated or suboptimally filled canals, inadequate core restorations, or leaking coronal restorations that may provide evidence of endodontic failure and a bacterial source for MSEO.25
TREATMENT
The objectives for treating MSEO are removal of pathogenic microorganisms, their by-products, and pulpal debris from the infected root canal system that are responsible for the sinus infection. Appropriate treatment options include nonsurgical root canal therapy, periradicular surgery (when indicated), intentional replantation, or extraction of the infected tooth. Patients should be informed of all treatment options and the prognosis of each, including the risks of no treatment.
Clinicians performing endodontic treatment in the posterior maxillary dentition should have extensive knowledge of maxillary root canal anatomy, the necessary armamentarium (including magnification), and requisite clinical skill considering the anatomic complexities and challenges in this region. Maxillary molars typically have the most complex anatomy in the dentition, and inadequate root canal treatment, particularly missed mesiobuccal canal systems, is a common cause of endodontic failure in maxillary molars.26–28 The close anatomic proximity of maxillary molar root apices to the floor of the maxillary sinus can lead to persistent MSEO if canals are left untreated or root canal failure occurs in these teeth. Endodontists are specialists in managing complex root canal systems and should be heavily relied upon for root canal treatment of maxillary molars.
Use of systemic antibiotics to manage MSEO should follow the guidelines set forth in the AAE Guidance on the Use of Systemic Antibiotics in Endodontics.29 Apart from spreading infections, antibiotic therapy is unwarranted in the treatment of MSEO and ineffective as a definitive solution. While antibiotic therapy may offer temporary relief of symptoms by improving sinus clearing, its sole use is inappropriate without definitive debridement and disinfection of the root canal system.
Similarly, surgical intervention of the maxillary sinus that is strictly focused on removing diseased sinus tissue and establishing drainage is inadequate if the endodontic component is neglected. Although these procedures are performed with the goal of reestablishing sinus aeration and drainage — and may provide relief of some symptoms — it is well documented that neglecting the dental etiology and focusing only on medical and surgical therapies of the ostiomeatal complex will not resolve MSEO.7,30–32
The dental literature provides numerous case reports showing full resolution of MSEO following endodontic treatment.2,11,33–38 It should be noted, however, that endodontic treatment alone may not resolve all cases of MSEO, therefore, clinical and radiological follow-up is essential, as concomitant management of the associated rhinosinusitis by an ENT specialist may be necessary.7,19,36,37,39–41
CONCLUSION
Fundamentally an endodontic infection manifesting in the maxillary sinus, MSEO is a common, yet underappreciated disease process. Symptoms and radiographic signs often mimic sinogenic sinusitis, leading patients to initially seek treatment from their primary care physician or ENT specialist — whose treatment will not resolve MSEO if the endodontic source is overlooked. This condition is also frequently overlooked in general dental practice due to a lack of dental symptoms and an obscured or atypical radiographic presentation. The increased availability of in-office CBCT imaging has increased clinicians’ ability to recognize and diagnose MSEO. Clinical endodontic examination, however, remains essential to an accurate diagnosis.
Endodontists are uniquely trained and equipped to diagnose endodontic disease that manifests in the maxillary sinus, as well as treat the complex canal anatomy commonly found in maxillary molars. Improved communication and referral relationships between general dentists, endodontic specialists and ENT surgeons are essential to appropriate patient care when managing MSEO.
KEY TAKEAWAYS
- Maxillary sinusitis of endodontic origin (MSEO) refers specifically to sinusitis caused by endodontic infection, excluding sinusitis secondary to other dental etiologies.
- This is a common disease process,2–14 yet despite its prevalence, MSEO is frequently unrecognized by dentists, radiologists and ear, nose and throat (ENT) specialists, with its sequelae often misdiagnosed as sinogenic sinusitis.7,11,13
- Limited-field cone beam computed tomography has been shown to significantly improve the ability to detect odontogenic sources for sinusitis.
- The objectives for treating MSEO are removal of pathogenic microorganisms, their by-products, and pulpal debris from the infected root canal system that are responsible for the sinus infection.
- Appropriate treatment options include nonsurgical root canal therapy, periradicular surgery (when indicated), intentional replantation, or extraction of the infected tooth.
- A collaborative effort and open referral relationship between general dentists, endodontists and ENT specialists are essential to achieve the best outcomes for patients diagnosed with MSEO.
A version of this article originally appeared in ENDODONTICS: Colleagues for Excellence, Fall 2018. Reused with permission from the American Association of Endodontists, ©2018. The AAE clinical newsletter is available at aae.org/colleagues
REFERENCES
- Bauer WH. Maxillary sinusitis of dental origin. Am J Orthod Oral Surg. 1943;29:133–151.
- Abrahams JJ, Glassberg RM. Dental disease: a frequently unrecognized cause of maxillary sinus abnormalities? Am J Roentenol. 1996;166:1219–1223.
- Mattila K. Roentgenological investigations of the relationship between periapical lesions and conditions of the mucous membrane of the maxillary sinuses. Acta Odontolog Scand. 1965;23:42–46.
- Obayashi N, Ariji Y, Goto M, et al. Spread of odontogenic infection originating in the maxillary teeth: computerized tomographic assessment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:223–231.
- Maillet M, Bowles WR, McClanahan SL, John MT, Ahman M. Cone-beam computed tomography evaluation of maxillary sinusitis. J Endod. 2011;37:753–757.
- Bomeli SR, Branstetter BF IV, Ferguson BJ. Frequency of a dental source for acute maxillary sinusitis. Laryngoscope. 2009;119:580–584.
- Patel NA, Ferguson BJ. Odontogenic sinusitis: an ancient but under-appreciated cause of maxillary sinusitis. Curr Opin Otoloaryngol Head Neck Surg. 2012;20:24–28.
- Melén I, Lindahl L, Andréasson L, Rundcrantz H. Chronic maxillary sinusitis. Definition, diagnosis and relation to dental infections and nasal polyposis. Acta Otolaryngol. 1986;101:320–327.
- Matsumoto Y, Ikeda T, Yokoi H, Kohno N. Association between odontogenic infections and unilateral sinus opacification. Auris Nasus Larynx. 2015;42:288–293.
- Troeltzsch M, Pache C, Troeltzsch M, et al. Etiology and clinical characteristics of symptomatic unilateral sinusitis: a review of 174 cases. J Craniomaxillofac Surg. 2015;43:1522–1529.
- Longhini AB, Ferguson BJ. Clinical aspects of odontogenic maxillary sinusitis: a case series. Int Forum Allergy Rhinol. 2011;1:409–415.
- Mehra P, Murad H. Maxillary sinus disease of odontogenic origin. Otolarngol Clin North Am. 2004;37:347–364.
- Pokorny A, Tataryn R. Clinical and radiologic findings in a case series of maxillary sinusitis of dental origin. Int Forum Allergy Rhinol. 2013;3:973–979.
- Kretzschmar DP, Kretzschmar JL. Rhinosinusitis: review from a dental perspective. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:128–135.
- Taschieri S, Torretta S, Corbella S, et al. Pathophysiology of sinusitis of odontogenic origin. J Investig Clin Dent. 2015;8:1–7.
- Eufinger H, Machtens E. Purulent pansinusitis, orbital cellulitis and rhinogenic intracranial complications. J Cranio Maxillofac Surg. 2001;29:111–117.
- Gold RS, Sager E. Pansinusitis, orbital cellulitis, and blindness as sequelae of delayed treatment of dental abscess. J Oral Surg. 1974;32:40–43.
- Williams JW Jr, Simel DL, Roberts L, Samsa GP. Clinical evaluation for sinusitis: making the diagnosis by history and physical evaluation. Ann Intern Med. 1992;117:705–710.
- Workman AD, Granquist EJ, Adappa ND. Odontogenic sinusitis: developments in diagnosis, microbiology, and treatment. Curr Opin Otolaryngol Head Neck Surg. 2018;26:27–33.
- Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical practice guideline (update): adult sinusitis executive summary. Otolaryngol Head Neck Surg. 2015;152:598–609.
- Tataryn RW, Lewis MJ, Horalek ML, et al. Maxillary Sinusitis of Endodontic Origin. American Association of Endodontists Position Statement. Available at: aae.org/specialty/wp-content/uploads/sites/2/2018/04/AAE_PositionStatement_MaxillarySinusitis.pdf. Accessed November 26, 2018.
- Low KM, Dula K, Bürgin W, von Arx T. Comparison of periapical radiography and limited cone-beam tomography in posterior maxillary teeth referred for apical surgery. J Endod. 2008;34:557–562.
- Nunes CA, Guedes OA, Alencar AH, et al. Evaluation of periapical lesions and their association with maxillary sinus abnormalities on cone-beam computed tomographic images. J Endod. 2016;42:42–46.
- Worth HM, Stoneman DW. Radiographic interpretation of antral mucosal changes due to localized dental infection. J Can Dent Assoc (Tor). 1972;38:111–116.
- Gomes AC, Nejaim Y, Silva AI, et al. Influence of endodontic treatment and coronal restoration on status of periapical tissues: a cone-beam computed tomographic study. J Endod. 2015;41:1614–1618.
- Wolcott J, Ishley D, Kennedy W, et al. A 5 yr clinical investigation of second mesiobuccal canals in endodontically treated and retreated maxillary molars. J Endod. 2005;31:262–264.
- Verma P, Love RM. A micro CT study of the mesiobuccal root canal morphology of the maxillary first molar tooth. Int Endod J. 2011;44:210–217
- Karabucak B, Bunes A, Chehoud C, Kohli MR, Stzer F. Prevalence of apical periodontitis in endodontically treated premolars and molars with untreated canal: a cone-beam computed tomography study. J Endod. 2016;42:538–541.
- Fouad AF, Byrne BE, Diogenes AR, et al. AAE Guidance on the Use of Systemic Antibiotics in Endodontics. American Association of Endodontists Position Statement. Available at: aae.org/specialty/wp-content/uploads/sites/2/2017/06/aae_systemic-antibiotics.pdf. Accessed November 26, 2018.
- Cartwright S, Hopkins C. Odontogenic sinusitis an underappreciated diagnosis: our experience. Clin Otolaryngol. 2016;41:284–285.
- Kulacz R, Fishman G, Levine H. An unsuccessful sinus surgery caused by dental involvement within the floor of the maxillary sinus. Op Techniques Otolaryngol Head Neck Surg. 2004;15:2–3.
- Longhini AB, Branstetter BF, Ferguson BJ. Unrecognized odontogenic maxillary sinusitis: a cause of endoscopic sinus surgery failure. Am J Rhinol Allergy. 2010;24:296–300.
- Nenzen B, Welander U. The effect of conservative root canal therapy on local mucosal hyperplasia in the maxillary sinus. Odontol Revy. 1967;18:295–302.
- Dodd RB, Dodds RN, Hocomb JB. An endodontically induced maxillary sinusitis. J Endod. 1984;10:504–506.
- Bogaerts P, Hanssens JF, Siquet JP. Healing of maxillary sinusitis of odontogenic origin following conservative endodontic retreatment: case reports. Acta Otorhinolaryngol Belg. 2003;57:91–97.
- Wang KL, Nichols BG, Poetker DM, Loehrl TA. Odontogenic sinusitis: a case series studying diagnosis and management. Int Forum Allergy Rhinol. 2015;5:597–601.
- Tomomatsu N, Uzawa N, Aragaki T, Harada K. Aperture width of the osteomeatal complex as a predictor of successful treatment of odontogenic maxillary sinusitis. Int J Oral Maxillofac Surg. 2014;43:1386–1390.
- Nurbakhsh B, Friedman S, Kulkarni GV, Basrani B, Lam E. Resolution of maxillary sinus mucositis after endodontic treatment of maxillary teeth with apical periodontitis: a cone-beam computed tomographic pilot study. J Endod. 2011;37:1504–1511.
- Simuntis R, Kubilius R, Vaitkus S. Odontogenic maxillary sinusitis: a review. Stomatologija. 2014;16:39–43.
- Saibene AM, Pipolo GC, Lozza P, et al. Redefining boundaries in odontogenic sinusitis: a retrospective evaluation of extramaxillary involvement in 315 patients. Int Forum Allergy Rhinol. 2014;4:1020–1023.
- Mattos JL, Ferguson BJ, Lee S. Predictive factors in patients undergoing endoscopic sinus surgery for odontogenic sinusitis. Int Forum Allergy Rhinol. 2016;6:677–700.
The author has no commercial conflicts of interest to disclose.
Featured image by STEVANOVICIGOR/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. January 2019;5(1):7–9.
