

Managing Sudden Cardiac Arrest in the Dental Office
Teams that are properly trained and equipped will be able to quickly respond to sudden cardiac arrest in dental patients.
Teams that are properly trained and equipped will be able to quickly respond to sudden cardiac arrest in dental patients
PURCHASE COURSE
This course was published in the December 2018 issue and expires December 2021. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
As oral health professionals, being prepared can spell the difference between life and death for patients experiencing a cardiac emergency in the dental office. More than 383,000 people experience sudden cardiac arrest each year in the United States, and less than 12% survive.1 This is one of the most frequently seen medical emergencies in the dental office, and clinicians and bystanders have less than five minutes to act before the victim develops permanent neurological damage.2 Ensuring staff members are well trained in cardiopulmonary resuscitation (CPR) and defibrillator use — along with having immediate access to emergency equipment — are imperative for prompt intervention.
This course was published in the December 2018 issue and expires December 2021. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain the prevalence of sudden cardiac arrest, as well as suggestions and requirements that dental settings be equipped with automatic external defibrillators (AEDs).
- Describe various pathologies for sudden cardiac arrest, and the importance of AEDs when responding to these events.
- Discuss clinical manifestations of cardiac arrest, and appropriate management strategies for the dental team.
The general populations’ increasing overall age (and subsequent medical involvement) raise the probability of encountering sudden cardiac arrest in oral health care settings.2 Once the heartbeat becomes arrhythmic, defibrillation is the only resolution.2 An automated external defibrillator (AED) is an essential tool in every dental office to manage these situations.2 As Rosenberg3 notes, “Early defibrillation with these easy-to-operate devices will convert two of the most common lethal cardiac dysrhythmias, ventricular fibrillation and ventricular tachycardia, into a normal sinus rhythm and restore oxygen perfusion to vital organs.” Survival rates decline by 7% to 10% with each passing minute an affected individual goes without defibrillation.1
Sudden cardiac arrest and sudden cardiac death (SCA/SCD) involve the rapid arrest or death of an individual due to cardiovascular-related issues. The heart’s electrical rhythm becomes chaotic — either through ischemic provocation or another arrhythmic trigger — and ultimately stops beating. Congestive heart disease is the most common underlying pathology for sudden cardiac arrest in adults over the age of 35.4 Risk factors for congestive heart disease, including diabetes mellitus, obesity, hypertension and high cholesterol, have a direct relationship with these events.4 Diabetes plays a role in the development of cardiovascular disease by increasing the amount of blood and workload placed on the heart. Its chambers are damaged through excessive dilation and hypertrophic enlargement, making each pump strenuous. Obesity increases the incidence of lethal arrhythmia and atrial fibrillation by structurally damaging the heart. When obesity and hypertension coexist, the heart grows even larger as its chamber volume is filled beyond capacity.5 Sudden cardiac death in young people, who may be affected by congenital cardiac structural abnormalities, is typically associated with high cholesterol.4
Though anxiety may not be instinctually associated with SCA/SCD, patients may experience apprehension at the dental office that can emanate from the glimpse of a sharp instrument or panicking over an anesthetic injection. Phobic anxiety and mental stress add strain to the heart muscles and contribute to cardiac symptoms, including tachycardia and hypertension.6,7
Despite evidence that links these risk factors to sudden cardiac arrest, more than half of SCA/SCD patients had not been diagnosed with cardiovascular conditions prior to their events.2,4 Because early recognition through risk factor assessment is not always possible, emergency preparation is essential to successful event management and patient survival.2 Dental teams should be able to recognize the physical manifestation of cardiac arrest or clinical death, including loss of consciousness, sudden collapse, or a lack of pulse and breathing.8 Making certain that staff members hold current Basic Life Support (BLS) for Healthcare Providers certification, and equipping all dental facilities with an AED, emergency kit and monitoring equipment — as well as developing and rehearsing an emergency action plan — will provide these patients with the best chance of survival.9
RELEVANCE IN DENTAL SETTINGS
There is an epidemiological transition in today’s society toward noncommunicable diseases, meaning that people are dying more from cardiovascular disease and diabetes than transferable infections.4 As medicine continues to advance, the general population is living longer, but typically has more medical needs. Compared to other groups, elderly, medically compromised patients are more likely to experience sudden cardiac arrest outside of a hospital, but less likely to survive the event before emergency medical care can be provided.2 Ensuring that dental offices are equipped with an AED should be a priority, as should regular staff training and establishing emergency office protocols.9
The American Dental Association (ADA) recommends that all dentists and dental hygienists be certified in BLS that encompasses competency in CPR and the proper use of an AED.6 While the ADA suggests defibrillators be part of every emergency kit, its Guidelines for the Use of Sedation and General Anesthesia by Dentists call for a unit to be immediately available in practices that perform deep sedation or general anesthesia.6 Health care providers cannot be certain how a patient will react to local anesthesia or dental materials. Although immediate activation of emergency medical services (EMS), along with prompt CPR, may buy an affected patient time, there is no other means by which to reactivate the heartbeat without the electrical stimulation of a defibrillator. The key to survival is early recognition and immediate action.2
By way of example, in 2011 a Texas dentist lost a patient during a routine root canal procedure when the clinician “fell below the minimum standard of care” by failing to recognize and appropriately manage a medical emergency. The provider did not institute correct protocols by:
- Administering appropriate medications
- Using advanced airway equipment
- Documenting an EKG and positive pressure ventilation
- Performing defibrillation
The 39-year-old patient went into sudden cardiac arrest. The dentist was issued a lengthy license suspension and significant fine, along with a time-sensitive requirement to complete specific continuing education courses.10
In 2015, a Minnesota dentist faced similar charges after his 17-year-old patient went into sudden cardiac arrest during a third molar extraction. Several preventable errors contributed to this incident, including:
- Dental assistants who were not properly trained in monitoring sedated patients
- Improper use of respiratory and blood pressure monitoring equipment
- Incorrect anesthesia administration
- Having a weak emergency plan
- Failure to inform the patient’s parents of the risks of general anesthesia
- Making a feeble attempt to respond to the patient’s emergency
The paramedics spent 20 minutes trying to stabilize the patient before transferring her to a hospital, where she died due to hypoxia to the brain.11
In contrast to these cases, in 2018 a dental team in Louisiana set the bar for what it means to be prepared. The 53-year-old patient came in to have two restorations placed. During the procedure, the dentist noticed the patient had become unresponsive and he immediately set the office emergency plan into action. All steps were well executed, with each staff member working with competence in managing the emergency. The dentist had made sure the office was equipped for a medical emergency by having an AED onsite (which is not required by law in Louisiana), and providing annual training exercises. Before EMS personnel arrived, the dental team had the patient stabilized, breathing and alert.12 Patients should be able to expect this standard of care when being treated at any dental office.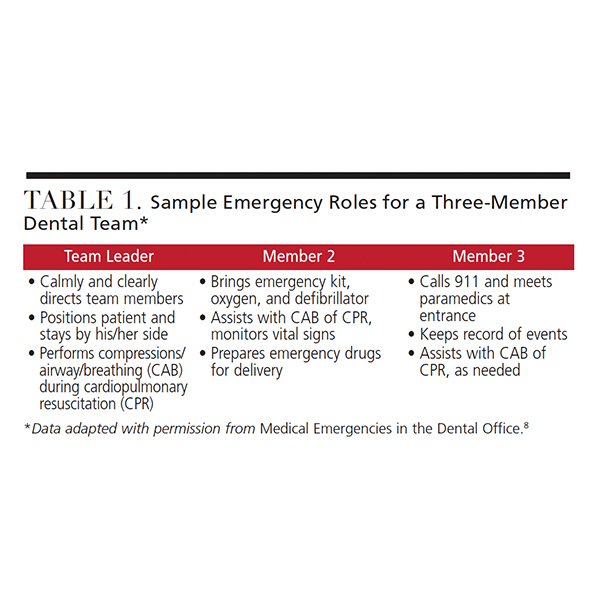
IMPLEMENT AN EMERGENCY PROTOCOL
As noted, along with ensuring the office has the proper equipment, dental teams should also establish an emergency protocol. Management strategies include a source of oxygen, basic emergency drugs, and training in BLS and use of emergency equipment.1 As part of efforts to be prepared, the team should practice their emergency plan regularly, making adjustments when necessary. Table 1 illustrates sample assignments for a three-member dental team in the event of a cardiac emergency.8 For any size office, there should be a team leader who takes control of the situation and directs other staffers. Typically, the leader is either the dentist or staff member with the patient at the time of the incident. Throughout the emergency, the team leader should remain calm, in control, and clearly delegate tasks — including directing someone to contact EMS immediately.
After positioning the patient supine, the team leader may begin CPR in the following steps:13
- Circulation: Check for a pulse on the radial, brachial or carotid arteries. If no pulse is detected, begin chest compressions-to-ventilation at a ratio of 30:2 for adults, children and infants. Once another member is available to aid in CPR, one rescuer will administer compressions while the other delivers ventilation, switching positions when necessary. With two members performing CPR, the ratio of compressions-to-ventilation for infants drops to 15:2.
- Airway: Tilt the patient’s head back and lift the chin.
- Breathing: Look, listen, and feel for chest movements and sounds. If the patient is not breathing, administer two deep breaths, lasting about a second each.13
 The team leader will administer any emergency drugs (if legally qualified), attach the oxygen mask to the patient’s face, and operate the AED to deliver an electrical shock to the patient’s heart.13 Above all, it is important that the leader make decisions aimed at the patient’s well-being.
The team leader will administer any emergency drugs (if legally qualified), attach the oxygen mask to the patient’s face, and operate the AED to deliver an electrical shock to the patient’s heart.13 Above all, it is important that the leader make decisions aimed at the patient’s well-being.
Team Member 2 is in charge of bringing the emergency kit, oxygen tank and AED to the team leader and patient as quickly as possible. This staffer will also prepare emergency drug doses, monitor the patient’s vital signs, and assist with CPR. In addition, this team member should conduct daily checks of the oxygen tank and weekly checks of the emergency drug kit and AED.8
Team Member 3 has the role of immediately contacting 911 and waiting at the office entrance to direct paramedics to the emergency area. This member should also document events, such as what time the patient fell into distress, who began CPR and when, what type of emergency drugs were administered (along with dosage), time of administration, and who administered them.8,9
In reality, the same staffer will not perform the same tasks in every emergency; hence the need for regular drills. Aside from drug administration, each employee should be able to properly carry out the functions of every role in an emergency.8,9
In the event a patient experiences sudden cardiac arrest in the dental office, following an emergency protocol may prove to be lifesaving. While the protocol may vary from office to office, the key point is that it takes approximately six to 12 minutes (or longer) for EMS to arrive with an AED, and the patient’s odds of survival decline by 10% with every passing minute the brain goes without oxygen.1
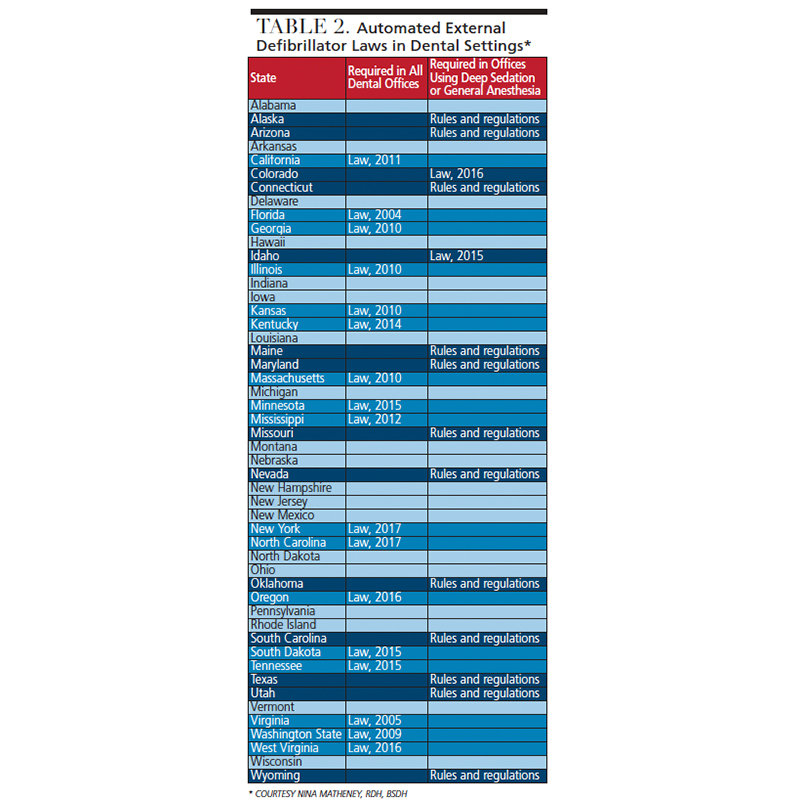
Although the ADA recommends having an AED in all dental settings,6 it is ultimately up to each state and its governing dental board to make this a requirement.10 As shown in Figure 1 and Table 2, a majority of states (two-thirds, in fact) do not mandate AEDs in all dental offices. At present, 17 states require an AED in every dental setting, while 14 states limit their requirements to offices permitted to perform general anesthesia or deep sedation. The remaining 19 states do not have AED requirements beyond the training that is provided during BLS certification (if BLS training is required).14
Offices that perform general anesthesia or deep sedation, while being more prepared with other safety equipment (including pulse oximeters, continuous EKG, and IV access), are not always required to have an AED present.14 To comply with the standard of care set by the American Heart Association (AHA), dental professionals have an ethical duty to have defibrillators present in the office,15 especially when accounting for factors that include phobic anxiety and local anesthesia allergies.6 The AHA has made early defibrillation an integral part of the BLS chain of survival for the treatment of patients in cardiac arrest.7 Since 1998, the AHA’s BLS for health care providers and CPR courses have included a mandated module on AED use.13 The immediate availability of a defibrillator has been shown to increase the success of early resuscitation in individuals experiencing sudden cardiac arrest, as well as a resulting decrease in sudden cardiac deaths.13
According to Pieren et al,6 the main issue preventing dental professionals from acquiring an AED is cost (devices range from $1000 to $3000),14 which was the prohibitive factor for 50% of the clinicians surveyed. Oral health professionals take an oath to “do no harm,”15 but a lack of foresight or preparation can have substantial consequences. Using a defibrillator can saves lives in a cardiac emergency, but, beyond this paramount goal, clinicians who are not prepared to respond adequately may face monetary losses during office closures for investigations, fines, and possible licensure revocation if found at fault. It is reassuring to know that good Samaritan laws protect those who help in good faith, or, in this case, use an AED in an attempt to save a life.1,16 If the patient cannot be revived, the rescuer will not be charged as “at fault” if he or she made a best effort to provide quality BLS.1,16

dental settings. COURTESY BRIANA GARZA, RDH, BSDH
CONCLUSION
Sudden cardiac arrest is one of the leading causes of death in the United States, claiming a life every two minutes.17 It accounts for more lives lost annually than breast cancer, lung cancer or acquired immunodeficiency syndrome.17 Among affected individuals, 95% of people who experience sudden cardiac arrest die because treatment was not available within minutes.17 Immediate access to an AED can help prevent death or a lifelong mental and/or physical disability.1
Dental professionals are responsible for maintaining a current medical history for each patient, but clinicians should also understand that it might not be all-inclusive. Patients who are silently anxious, have undiagnosed heart conditions, or experience severe allergic reactions to dental materials can quickly develop SCA/SCD. Although AEDs can be found in many offices where dentists are permitted to perform general anesthesia or deep sedation, many practices do not have defibrillators.2 Requiring that an AED be present in all dental settings minimizes the possibility of a seemingly healthy patient experiencing sudden cardiac arrest and dying unnecessarily.
Acknowledgement:
The authors wish to thank Briana Garza, RDH, BSDH, for her contributions in the development of the graphic materials for this article.
REFERENCES
- American Heart Association. Automated External Defibrillator: Implementing an AED Program. Available at: https://cpr.heart.org/idc/groups/heart-public/@wcm/@ecc/documents/downloadable/ucm_480036.pdf. Accessed October 30, 2018.
- Boyd B, Fantuzzo JJ, Votta T. The role of automated external defibrillators in dental practice. N Y State Dent J. 2006;72:20–23.
- Rosenberg M. Preparing for medical emergencies: the essential drugs and equipment for the dental office. J Am Dent Assoc. 2010;141(Suppl 1):S14–S19.
- Hayashi M, Shimizu W, Albert CM. The spectrum of epidemiology underlying sudden cardiac death. Circ Res. 2015;116:1887–1906.
- Anand R, Peters RW, Donahue TP. Obesity and dysrhythmias. J Cardiometab Syndr. 2008;3:149–154.
- Pieren JA, Gadbury-Amyot CC, Kandray DP, Van Ness CJ, Mitchell TV. The attitudes of Ohio dentists and dental hygienists regarding the use of automated external defibrillators in the dental setting — a follow-up study. J Dent Hyg. 2013;87:158–168.
- Albert CM, Chae CU, Rexrode KM, Manson JE, Kawachi I. Phobic anxiety and risk of coronary heart disease and sudden cardiac death among women. Circulation. 2005;111:480–487.
- Malamed, S. Medical Emergencies in the Dental Office. 7th ed. St. Louis, Mo: Elsevier Mosby; 2015:65–67,479.
- Haas DA. Preparing dental office staff members for emergencies. J Am Dent Assoc. 2010;141:S8–S13. 1
- In the Matter of the License of Jayson B. Huneycutt, DDS, Texas Dental License Number 17283. SBDE No. 2012-00069, 1 (Texas State Board Of Dental Examiners 2017).
- Stipulation and Order for Stayed Suspension, Limited and Conditional License. (Minnesota Board of Dentistry 2016).
- Clark M. Why your dentist’s office should have a defibrillator on site. Available at: http://s.nola.com/4efSGIm. Accessed October 30, 2018.
- American Heart Association. Highlights of the 2017 American Heart Association Focused Updates on Adult and Pediatric Basic Life Support and Cardiopulmonary Resuscitation Quality. Available at: https://eccguidelines.heart.org/wp-content/uploads/2017/11/2017-Focused-Updates_Highlights.pdf. Accessed October 30, 2018.
- AED Laws by State. Available at: http://www.aeduniverse.com/AED_Laws_by_State_s/97.htm#Texas. Accessed October 30, 2018.
- American Dental Association. The ADA Principles of Ethics and Code of Conduct. Available at: https://www.ada.org/en/about-the-ada/principles-of-ethics-code-of-professional-conduct. Accessed October 30, 2018.
- American Academy of Orthopaedic Surgeons. Liability under “Good Samaritan” Laws. Available at: https://www.aaos.org/AAOSNow/2014/Jan/managing/managing3/?ssopc=1. Accessed October 30, 2018.
- Heart Rhythm Society. Sudden Cardiac Arrest (SCA) Awareness. Available at: https://www.hrsonline.org/News/Sudden-Cardiac-Arrest-SCA-Awareness. Accessed October 30, 2018.
Featured image by ARICAN/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. December 2018;4(12):26—29.

