
 RDONAR/ISTOCK/GETTY IMAGES PLUS
RDONAR/ISTOCK/GETTY IMAGES PLUS
Managing Skeletal Problems in Pediatric Malocclusion
In cases of pediatric malocclusion, taking advantage of growth potential can sometimes eliminate or modify skeletal anomalies and promote normal dental and skeletal growth
Part 2 of a two-part series: This is the concluding installment of a two-part series. Appearing in January 2020, Part 1 (available at decisionsindentistry.com) offers an overview of the pediatric and general dentist’s role in early intervention in malocclusion involving issues with space management and posterior crossbite.
The most important reason to initiate early orthodontic treatment in children is to correct or reduce the severity of malocclusion and skeletal discrepancy, and allow normal maxillofacial growth and development. The maxillofacial skeleton in growing children is adaptable to change from both internal and external forces. Thus, taking advantage of growth potential can sometimes eliminate or modify skeletal anomalies and promote normal dental and skeletal growth. While the first article in this series, “Management of Malocclusion in Children and Adolescents” (available at decisionsindentistry.com), covered space management and posterior crossbite correction, this concluding installment will focus on common skeletal Class II and Class III malocclusion management.
One-third of the United States population aged 6 to 17 have Class II occlusion.1 Among these individuals, 15% have an anterior overjet greater than 4 mm, and 38% range between 3 and 4 mm. Class II occlusion cannot self-correct and, in some cases, can worsen with age.2 It is mainly perceived as a sagittal discrepancy, with the majority of cases due to mandibular retrognathism (Figure 1).

The transverse development is often overlooked. Most Class II malocclusions are normally transverse in centric occlusion (CO), but when the mandible moves forward, it shows maxillary constriction. Research has shown Class II Division 1 cases with posteriorly transverse interarch discrepancy (PTID) can present with a mandible that is posterior displaced by a functional shift, which accentuates the severity of the Class II occlusion.3 It is important to check for the presence of PTID in diagnosing a true retrognathic mandible. In Class II cases with PTID, mandibular size is normal and the retrusion is associated with posterior displacement by functional shift. In Class II cases without PTID, mandibular retrusion is due to a true micrognathic mandible, and early expansion can enhance forward growth of the mandible.1 Sagittal problems aside, evaluating transverse development of each Class II malocclusion case is crucial in treatment planning.
MANAGING SKELETAL CLASS II MALOCCLUSION
In a growing patient, the best way to correct Class II malocclusion is through growth modification. Common treatment uses headgear to restrain the maxillary forward growth if there is excess maxillary growth, or a functional appliance to advance the mandible if there is a retrusive lower jaw. In severe Class II cases, these appliances can be combined. The effectiveness of headgear has been well documented; for example, such appliances can restrict maxillary sagittal growth and retract upper anterior teeth to achieve Class I occlusion (Figures 2A and 2B). A systematic review and meta-analysis showed that compared to a control group, patients using headgear had a resulting change of -1.41 degrees per year of sella, nasion, A point (SNA), -1.42 degree per year of A point, nasion, B point (ANB), and -1.31 mm per year of anterior overjet.4 The study concludes that headgear treatment is effective in restricting maxillary growth and reducing overjet in the short term. A long-term study on the stability of early headgear treatment, however, showed no significant difference between the headgear and control groups in a 13-year follow-up.5
headgear (B).
Most Class II malocclusions have a component of mandibular deficiency.6 The use of functional appliances (FA) has been advocated since the 1930s to aid in mandibular growth. By positioning the mandible forward and transferring muscle forces from the maxillary and mandibular teeth onto the periosteum and bone, these appliances produce a restraining effect on the forward growth of the maxilla and stimulate mandibular growth. The design of an FA can be removable or fixed, tooth-borne or tissue-borne, and passive or active (Figures 3A and 3B). Several systematic reviews conclude FAs can reduce overjet, correct molar relationships, and reduce the severity of Class II malocclusion. Most of these corrections are due to dentoalveolar changes and a small amount of a favorable mandibular growth.7

One randomized prospective clinical trial demonstrated that use of either headgear or an FA in early treatment of Class II malocclusion can reduce the severity of a Class II skeletal pattern by 75% in the short term.8 Early orthodontic treatment can effectively correct Class II malocclusion, but it often will require a second phase of treatment at a later age. Several randomized controlled trials concluded that in moderate-to-severe Class II cases, two-phase treatment does not produce a major difference in jaw relationship or final occlusion compared to one-phase treatment at a late stage of growth. Phase I treatment of Class II occlusion is effective, but not efficient. It does, however, offer the additional benefits of reducing maxillary incisor trauma and promoting patient self-esteem.9 The early treatment of Class II malocclusion has become a point of controversy in orthodontics, with providers disagreeing over the value of Phase I treatment for Class II malocclusions due to its likely need for a second phase of orthodontics.
MANAGEMENT OF ANTERIOR CROSSBITE AND CLASS III MALOCCLUSION
Class III malocclusion can range from a simple anterior crossbite to severe skeletal discrepancy. This problem can be seen as early as the primary dentition and is easily identifiable by clinicians and parents/caregivers. Often, it is the parent/caregiver who requests this “underbite” be corrected, regardless of the child’s age. Early correction of anterior crossbite can improve esthetics, resolve a functional shift to prevent structural damage, and prevent possible adverse effects on future dental and skeletal growth.
SIMPLE ANTERIOR DENTAL CROSSBITE
With prevalence ranging between 3% and 12%, simple anterior crossbite is a common problem in both the primary and early mixed dentition.10 Clinical examination shows one or more maxillary incisors tipped lingually, with a normal ANB angle, normal profile, usually mild to no crowding, and no functional shift. The key principle in these cases is to open the bite and procline the lingually tipped tooth. Common appliances used in primary dentition are an incline plane or a fixed sliding upper lingual arch, with occlusal composite resin for disocclusion. A removable plate with a finger spring is effective in mixed dentition, but is not recommended in primary teeth due to lack of retention of the appliance, as well as young children’s limited compliance with removable appliances.
PSEUDO CLASS III
Pseudo Class III cases are often referred to by other names, including functional Class III, postural Class III, or pseudoprognathism. They can occur in primary, mixed and permanent dentitions. One article reported 60% to 70% of anterior crossbites in the Chinese population aged 8 to 12 were pseudo Class III.11 To diagnose these cases, the practitioner must check the centric relation (CR) and CO, as there is always a functional shift from CR to CO in pseudo Class III cases. Facial profile is normal at CR and concave at CO, and molar relationship is Class I in CR and Class III in CO. The upper incisors are retroclined, and lower incisors may be proclined and show tissue damage. Appliances that can effectively correct the problem and lead to stable results include a biteplate with finger springs, sliding lingual arch, partial fixed 2×4 orthodontic brackets with bite open bloc, and other Class III FAs (Figures 4A through 4C). Major benefits to correcting anterior crossbites with functional shift are releasing the maxilla from interference to normalize its growth; preventing asymmetric muscular strain and condylar displacement by functional shift; and gaining arch length by incisor proclination (within the limits allowed by the alveolar housing).

SKELETAL CLASS III MALOCCLUSION
Skeletal Class III malocclusion can be due to maxillary deficiency with a normal mandible, normal maxilla with mandibular prognathism, or a combination of maxillary deficiency and mandibular prognathism. At 10% to 19%, the Asian population has a higher prevalence of skeletal Class III malocclusion than the Caucasian population (< 5%).11 The etiology is mainly genetic, although environmental factors, such as mouth breathing, may also play a role. Clinical signs include a concave profile, midface retrusion, prominent mandible, narrowed upper arch, and negative anterior overjet. Class III malocclusion skeletal disproportions are established early and tend to worsen with subsequent growth. Additionally, Reyes et al12 report the Class III group demonstrated more postpubertal mandibular length growth than the control group.
MANAGING SKELETAL CLASS III PROBLEMS IN CHILDREN
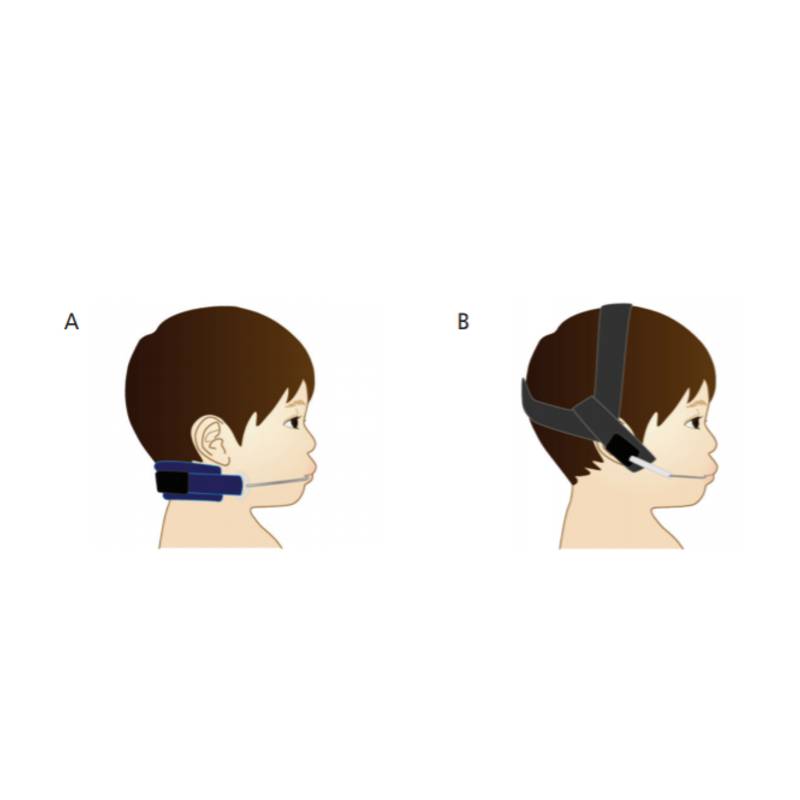
Inasmuch as Class III cases have been attributed to mandibular prognathism, a reasonable appliance to consider for restraining mandibular growth is the chin cap (Figure 5). The objective of chin cap treatment is inhibiting or posteriorly directing mandibular growth. There are two types: occipital pull, for mandibular excess growth with normal to short anterior facial height; and vertical pull, for a high mandibular plane angle with long anterior facial height. Patients are instructed to wear the chin cap 12 to 14 hours per day, during which it applies a force of 300 to 500 grams per side. While the chin cap’s inhibitive effect on mandibular growth is well documented,13,14 recent studies have shown chin caps cannot stop growth or reduce mandibular length. In the short term, these devices redirect mandibular growth downward and backward during therapy; but, after discontinuation of treatment, the mandible usually returns to the original growth pattern and the treatment effect is lost.15 These devices can have lasting effects, however, when used in appropriate cases. The clinical indication for a chin cap is to start in the deciduous or early mixed dentition for skeletal Class III patients with a large mandible and normal maxilla, mild to moderate skeletal discrepancy, normal cranial base angle, normal or short anterior facial height, and no evidence of temporomandibular joint disorder.

FACE MASK PROTRACTION FOR MAXILLARY HYPOPLASIA
More than 40% of Class III cases show maxillary retrusion with either a normal or prognathic mandible.16 Since the 1970s, the protraction of maxilla with rapid maxillary expansion (RME) has gained popularity.17–19 The treatment protocol is RME plus face mask (FM) protraction (Figures 6A and 6B). The treatment starts with RME, two turns (0.5 mm) per day for seven to 10 days, followed by FM with a force of 300 to 600 grams per side, 30 degrees to occlusal plane pull, with the patient wearing the FM 10 to 12 hours per day. Normally, the maxilla can be advanced 2 to 4 mm in 12 to 15 months. The effectiveness of Class III correction is the result of forward maxillary movement (31%), backward rotation of the mandible (21%), proclination of the maxillary incisors (28%), and retroclination of the mandibular incisors (20%).20

The main objective of early RME plus FM protraction is to take advantage of open, smooth and broad circummaxillary sutures in young patients to enhance skeletal advancement of the maxilla and reduce dentoalveolar compensation. Proffit et al21 suggested initiating forward repositioning of the maxilla before age 8 to gain skeletal change. After age 8, dentoalveolar change outpaces skeletal change.21 The optimal time for treatment is in the primary or early mixed dentition. Research has demonstrated no difference in treatment results with the use of RME plus FM when initiated after age 8, even in early permanent dentition.22 Long-term stability of protraction is 67% on average following RME plus FM treatment.23 For about one-third of patients, relapse showed the mandible outgrew the maxilla by four times, and the stable group had only two times greater growth compared to the control Class I group. Patients who are unstable after RME plus FM protraction may need additional treatment with orthognathic surgery at a later stage.
UNWANTED SIDE EFFECTS
Although RME plus FM therapy has proven effective, the limitations and side effects have driven orthodontists to seek alternative treatments. Side effects include loosening of the tooth-borne anchorage, maxillary incisor proclination, extrusion and mesial tipping of upper molars, and occlusal plane rotation downward and backward, as well as similar changes in the mandibular plane that result in increased dentoalveolar compensation. These complications make RME plus FM unsuitable for patients with missing posterior teeth or cases involving high mandibular angles, as well as older children.
Recent developments in bone anchorage allow FMs to be anchored to the bone and alleviate some of the side effects of dentition anchored FMs. Bone anchorage options to be used with FM therapy include mini-plate, hybrid hyrax, palatal plate, micro-implant assisted RPE (MARPE), and bone anchor maxillary protraction (Figures 7A through 7C).24–28 Common findings of bone anchored treatment include predictable disruption of the circummaxillary suture, more maxillary forward displacement, reduced adverse effects from tooth-borne expansion, less clockwise mandibular plane rotation, and application for postpuberty or mature patients.29–31

REMOVABLE INTRAORAL APPLIANCES
Additional options for treating Class III malocclusion include removable appliances, such as a mandibular retractor, reverse twin-block, Frankel III, double plates, and the tandem traction bow (Figure 8). Because these produce mainly dentoalveolar (as opposed to skeletal change), these approaches are a less favorable therapeutic option.

SUMMARY OF TREATMENT OPTIONS
Here is an overview of management options for treating pediatric skeletal Class III cases:
Ages 5 to 10
• Mild to moderate Class III: RME plus FM for maxillary deficiency
• Chin cap for mandibular prognathism with low mandibular angle, and no temporomandibular joint disorder
Ages 10 to 12
• Bone anchor maxillary protraction with Class III elastics
• Mini-plate plus FM, hybrid hyrax plus FM, palatal plate plus FM, MARPE plus FM
Postpuberty
• Orthodontic camouflage treatment
Mature
• Orthodontic and orthognathic surgery
CONCLUDING THOUGHTS
With effective intervention, many early dental and skeletal anomalies can be corrected or reduced in severity in the primary or early mixed dentition. Although controversy surrounds the efficacy of early intervention in Class II malocclusion, this approach has been shown to be effective. It can also promote a child’s self-esteem and prevent potential incisor trauma.
It is also important to realize that whether dental or skeletal in origin, Class III malocclusion may cause soft tissue, dental and/or skeletal damage. Consequently, early intervention (as detailed in this paper) is recommended; in addition, the selective use of bone anchorage devices can produce good results in older children.
KEY TAKEAWAYS
- The most important reason to initiate early orthodontic treatment in children is to correct or reduce the severity of malocclusion and skeletal discrepancy, and allow normal maxillofacial growth and development.
- An effective way to correct Class II malocclusion in a growing patient is through growth modification.
- Common treatment modalities use headgear to restrain the maxillary forward growth if there is excess maxillary growth, or a functional appliance to advance the mandible if there is a retrusive lower jaw. In severe Class II cases, these appliances can be combined.
- Class III malocclusion can range from a simple anterior dental crossbite to severe skeletal discrepancy; this problem can be seen as early as the primary dentition.
- Skeletal Class III malocclusion can be due to maxillary deficiency with a normal mandible, normal maxilla with mandibular prognathism, or a combination of maxillary deficiency and mandibular prognathism.
- With effective intervention, many early dental and skeletal anomalies can be corrected or reduced in severity in the primary or early mixed dentition.
REFERENCES
- McLain J, Proffitt W. Oral health status in the United States: Prevalence of malocclusion. J Dent Educ. 1986;49:386–396.
- Stahl F, Baccetti T, Franchi L. McNamara J. Longitudinal growth changes in untreated subjects with Class II Division 1 malocclusion. Am J Orthod Dentofacial Orthop. 2008;134:125–137.
- Tollaro I, Baccetti T, Franchi L, Tanasescu C. Role of posterior transverse interarch discrepancy in Class II, Division 1 malocclusion during the mixed dentition phase. Am J Ortho Dentofac Orthop. 1996;110:417–422.
- Papageorgiou S, Kutschera E, Memmert S, et al. Effectiveness of early orthopaedic treatment with headgear: a systematic review and meta-analysis. Euro J Orthod. 2017;39:176–187.
- Krusinskiene V, Kiuttu P, Julku J, et al. A randomized controlled study of early headgear treatment on occlusal stability — a 13 year follow-up. Euro J Orthod. 2008;30:418–424.
- McNamara J. Components of Class II malocclusion in children 8–10 years of age. Angle Orthod. 1981;51:177–202.
- O’Brien K. Is early treatment for Class II malocclusion effective? Results from a randomized controlled trial. Am J Ortho Dentofacial Orthop. 2006;129(Suppl 4):S64–S65.
- Tulloch JF, Phillips C, Koch G, Proffitt WR. The effect of early intervention on skeletal pattern in Class II malocclusion: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 1997;111:391–400.
- Thiruvenkatachari B, Harrison J, Worthington H, O’Brien K. Early orthodontic treatment for Class II malocclusion reduces the chance of incisor trauma: results of a Cochrane system review. Am J Orthod Dentofacial Orthop. 2015;148:47–59.
- Lin JJ. Prevalences of malocclusion in Chinese children age 9–15. Clin Dent. 1985;5:57–65.
- Hardy D, Cubas Y, Orellana M. Prevalence of angle Class III malocclusion: a systemic review and meta-analysis. Open J Epidemiol. 2012;2:75–82.
- Reyes B, Baccetti T, McNamara J. An estimate of craniofacial growth in Class III malocclusion. Angle Orthod. 2006;76:577–584.
- Alarcon J, Bastir M, Rosas A, Molero J. Chincup treatment modifies the mandibular shape in children with prognathism. Am J Orthod Dentofacial Orthop. 2011;140:38–43.
- Liu ZP, Li CJ, Hu HK, Chen JW, Li F, Zou SJ. Efficacy of short-term chincup therapy for mandibular growth retardation in Class III malocclusion: a systemic review. Angle Orthod. 2011;81:162–168.
- Sugawara J, Mitani H. Facial growth of skeletal Class III malocclusion and the effects, limitations, and long-term dentofacial adaptations to chincap therapy. Semin Orthod. 1997;3:244–254.
- Guyer EC, Ellis EE, McNamara JA, Beherents RG. Components of Class III malocclusions in juveniles and adolescents. Angle Orthod. 1986;56:7–30.
- McNamara JA. An orthopedic approach to the treatment of Class III malocclusion in young patients. J Clin Orthod. 1987;9:598–608.
- Ngan P, Wei SH, Hagg U, Yiu CK, Merwin D, Stickel B. Effects of headgear on Class III malocclusion. Quintessence Int. 1992;23:197–207.
- Baccetti T, McGill JS, Franchi L, McNamara JA, Tollaro I. Skeletal effects of early treatment of Class III malocclusion with maxillary expansion and facemask therapy. Am J Orthod Dentofacial Orthop. 1998;113:333–343.
- Ngan P, Hagg U, Yiu C, Wei SH. Treatment response and long-term dento-facial adaptations to maxillary expansion and protraction. Semin Orthod. 1997;3:255–264.
- Proffit WR, Fields HW, Sarver DM. Contemporary Orthodontics. 5th ed. Mosby: Maryland Heights, Mo; 2007.
- Kapust A, Sinclair P, Turley. Cephalometric effects of face/a/k/expansion therapy in Class III children: a comparison of three age groups. Am J Orthod Dentofacial Orthop. 1998;113:204–212.
- Hagg U, Tse A, Bendeus M, Rabie AB. Long-term follow-up of early treatment with reverse headgear. Eur J Orthod. 2003;25:95–102.
- Lee NK, Yang IH, Baek SH. The short-term treatment effects of face mask therapy in Class III patients based on the anchorage device: miniplates vs rapid maxillary expansion. Angle Orthod. 2012;82:846–852.
- Wilmes B, Ngan P, Liou EJ, Franchi L, Drescher D. Early Class III facemask treatment with the hybris hyrax and Alt-RAMCE protocol. J Clin Orthod. 2014;48:84–93.
- Kim KY, Bayome M, Park JH, Kim KB, Mo SS, Kook YA. Displacement and stress distribution of the maxillofacial complex during maxillary protraction with buccal versus palatal plates: finite element analysis. Euro J Orthod. 2015;37:275–283.
- Moon W. Class III treatment by combining facemask (FM) and maxillary skeletal expander (MSE). Semin Orthod. 2018;24:95–107.
- Nguyen T, Cevidanes L, Cornelis M, Heymann G, de Paula LK, De Clerk HD. Three-dimensional assessment of maxillary changes associated with bone anchored maxillary protraction. Am J Orthod Dentofacial Orthop. 2011;140:790–798.
- Major MP, Wong JK, Saltaji H, Major P, Flores-Mir C. Skeletal anchored maxillary protraction for midface deficiency in children and early adolescents with Class III malocclusion: a systemic review and meta-analysis. J World Fed Orthod. 2012;1:e47–e54.
- Cevidanes L, Baccetti T, Franchi L, McNamara J, Clerck HD. Comparison of two protocol for maxillary protraction: bone anchors versus face mask with rapid maxillary expansion. Angle Orthod. 2010;80:799–806.
- Morales-Fernández M, Iglesias-Linares A, Yañez-Vico RM, Mendoza-Mendoza A, Solano-Reina E. Bone-and dentoalveolar-anchored dentofacial orthopedics for Class III malocclusion: new approaches, similar objectives? A systemic review. Angle Orthod. 2013;83:540–552.
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. May 2020;6(5):18, 21–24.
