

Managing Complications in Gingival Recession
Tips to address acellular dermal matrix graft complications in root coverage treatment.
PURCHASE COURSE
This course was published in the January/February 2025 issue and expires February 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the January/February 2025 issue and expires February 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 490
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify the factors contributing to gingival recession progression and the clinical indications for early intervention.
- Describe the application, benefits, and limitations of acellular dermal matrix (ADM) grafting in root coverage procedures.
- Outline strategies for managing ADM graft-related complications and improving clinical outcomes through corrective surgery techniques.
More than 90% of Americans older than age 30 have gingival recession.1 Although the need to treat nonsymptomatic gingival recession defects remains controversial, a systematic review indicated that a considerable percentage of untreated gingival recession defects exhibited notable progression, even with the subject’s adherence to effective plaque control measures.2 This finding justifies early intervention, especially when unfavorable local anatomic factors exist, such as teeth with inadequate keratinized tissue width (KTW), thin tissue phenotype, aberrant frenum attachment, tooth malposition, poor oral hygiene, and intrasulcular restorative margin.3 When these are present, the patient should be informed of the elevated disease risk as well as treatment options.
Root coverage procedures have been studied for decades to optimize efficacy in the treatment of gingival recession defects.4 Although subepithelial connective tissue graft (CTG) in conjunction with a coronally advanced flap (CAF) remains the gold standard for the treatment of gingival recession, nonautogenous graft substitutes have emerged that offer advantages.5,6
Acellular dermal matrix (ADM) is a graft obtained from the dermal tissue of a cadaver that has undergone chemical treatment to remove antigenic components.7 In soft tissue regeneration, ADM functions as a tissue scaffold for the ingrowth of host cells with a relatively low immune response.8
Clinical indications for using ADM for root coverage treatment include long-span multiple gingival recession defects and the patient’s resistance to the use of autogenous tissue. The smooth surface and uniform thickness of ADM provide ideal handling for the tunneling technique. However, ADM has limited efficacy in increasing KTW and maintaining long-term stability. A clinical study showed significant relapse from 65% to 89% mean root coverage at 12-year follow up in ADM-treated recession.9 To increase the predictability of ADM grafting, increased caution is required, as ADM must be completely submerged under the flap, otherwise, the uncovered portion may cause complications.
Even though ADM graft-exposed-related complications are not uncommon, the literature focusing on ADM-related complications is scarce. Thus, this case report presents the management of a complication that arose after ADM grafting and the subsequent corrective surgery.

Clinical Presentation
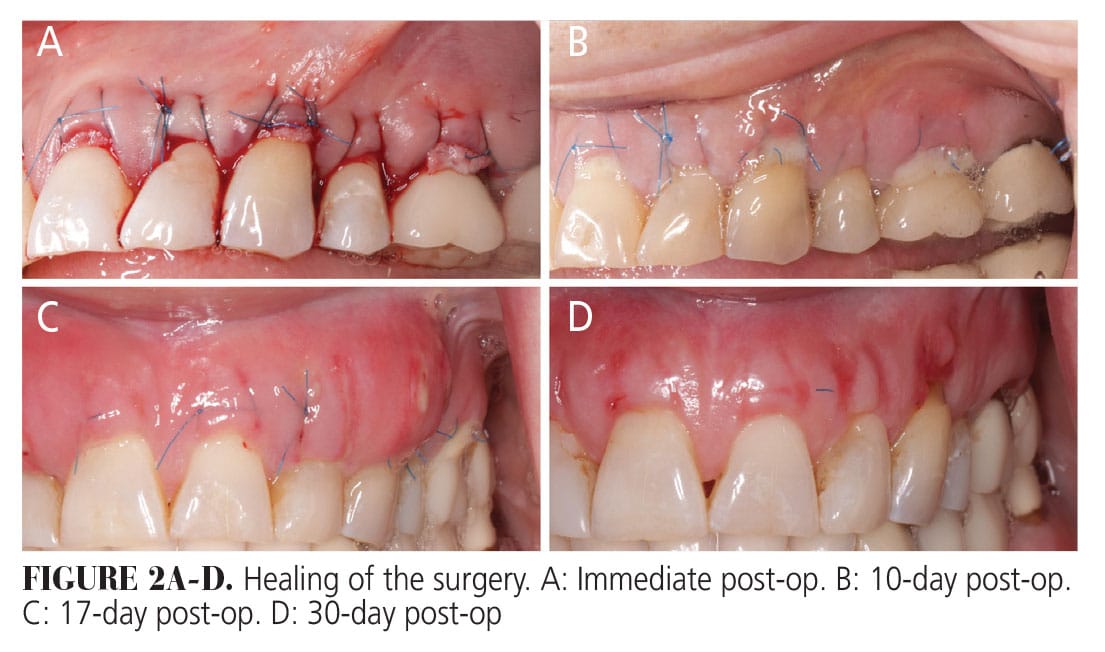
A 54-year-old nonsmoking, ASA II, woman presented to a post-graduate dental clinic complaining of recession-related sensitivity. The patient reported a history of orthodontic treatment. Clinical examination revealed generalized 1-4 mm buccal recession type (RT) 1 with noncarious cervical lesions. At baseline (Figure 1), gingival phenotype was thick and scalloped. KTW was greater than 2 mm except for the canine site. Periodontal diagnosis was gingival health on a reduced periodontium of a nonperiodontitis patient. Previous orthodontic treatment and traumatic brushing forces were possible etiologies. Treatment options were presented and the patient selected ADM as the graft material. The root coverage procedure was performed using the subperiosteal tunneling technique in conjunction with ADM. However, graft exposure and infection occurred post-operatively (Figures 2A-D).
Part 1. Complications
No infection was noticed at the 1-week post-op. At 10-day post-op (Figure 2B), the patient reported increased pain and swelling, accompanied by foul odor. Moderate swelling and suppuration were observed. An extended 7-day course of 300 mg clindamycin TID was prescribed due to penicillin allergy. At 17-day post-op (Figure 2C), the size of graft exposure enlarged on #14 and an abscess formed on #11. The exposed sloughing graft was meticulously trimmed with a 15 c scalpel. The 300 mg clindamycin TID was refilled for another 3 days. The 10% povidone-iodine (PvI) solution was dispensed. At 30-day post-op (Figure 2D), swelling and infection symptoms were resolved. The surgical outcome was re-evaluated at 5-month follow-up, and partial coverage was observed with 1 to 3 mm residual defects (Figure 3). The patient expressed dissatisfaction and requested a corrective surgery.

Part 2. Corrective Procedure
Six months after the first procedure, a corrective surgery was performed with the gold standard treatment modality: CAF + connective tissue graft (CTG). Following local anesthesia using 4% articaine with 1/100,000 epinephrine, the incisions were made following the envelope-CAF10 (Figure 4A). The buccal partial-full-partial thickness flap was elevated (Figure 4B). Superficial and deep dissection was prepared at the vestibular level until the adequate passivity of the flap was achieved (Figure 4C).
Anatomical papillae were de-epithelialized. The unattached root surface was debrided and planed with a back-action chisel. The root surface was conditioned with 17% ethylenediaminetetraacetic acid gel for 2 minutes. A free gingival graft (FGG) was harvested from the premolar-molar area and de-epithelialized extraorally11 (Figure 4D-E). De-epithelialized CTG was sectioned into two pieces and sutured to #11 and #14 with a 6-0 polycaprolactone copolymer suture in a single interrupted manner (Figure 4F). The buccal flap was coronally repositioned and sutured with a sling suture using 6-0 polypropylene (Figure 4G).
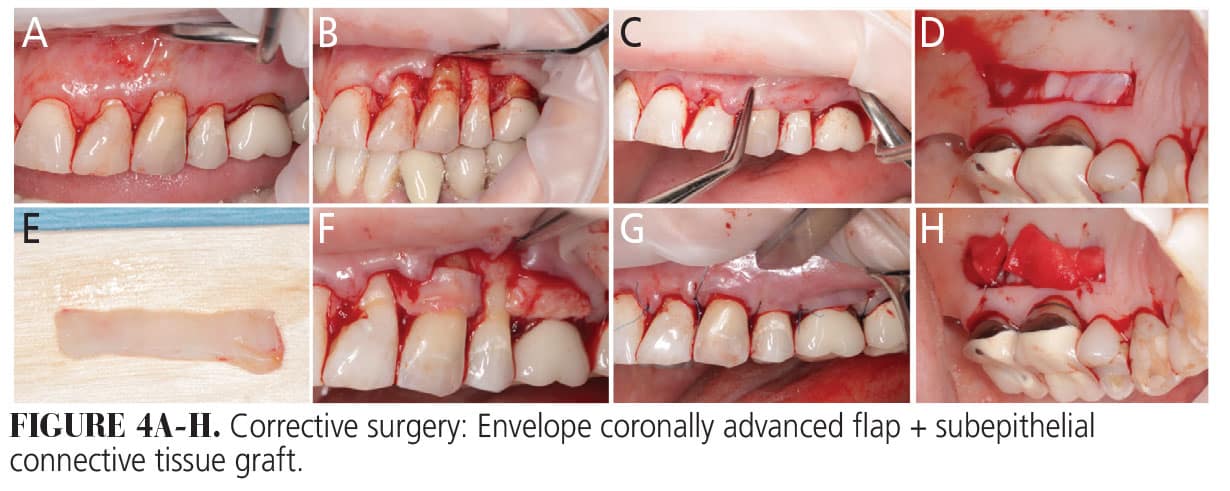
Hemostasis of the donor site was achieved with collagen matrix and compressive sutures (Figure 4H). Post-operative instruction included the use of chlorhexidine gluconate (CHX) mouthrinse, methylprednisolone dose pack, 300 mg clindamycin, and ibuprofen 600 mg for 7 days. The patient was instructed to refrain from mechanical cleaning in the surgical area. The patient was recalled at 3 weeks, 8 weeks, and 6 months.
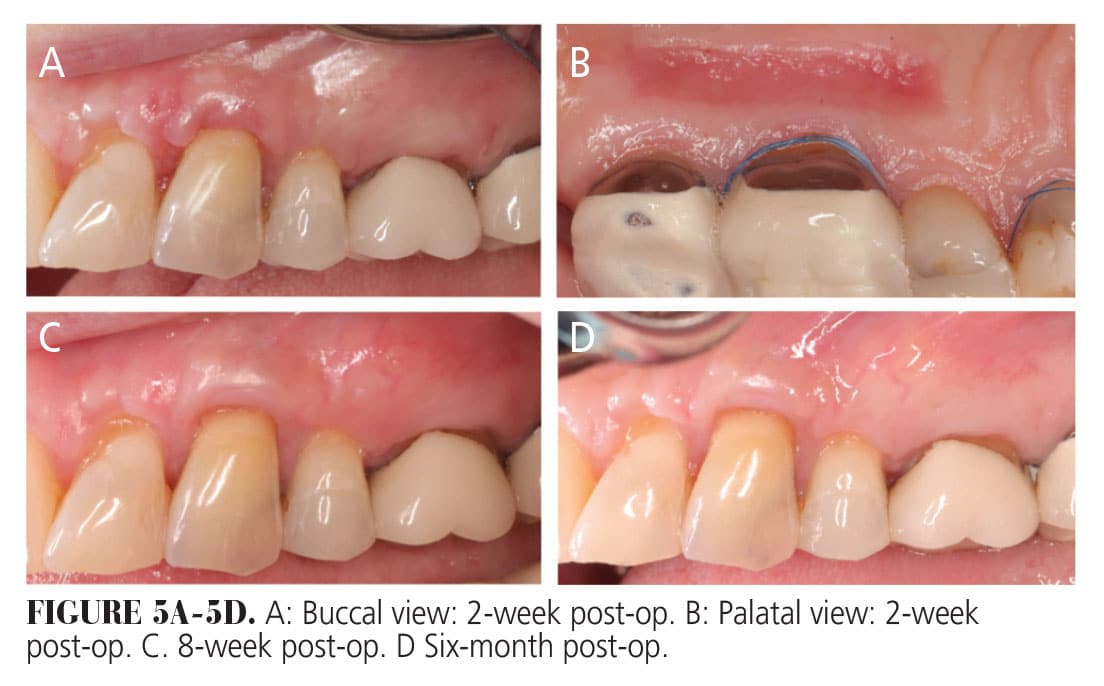
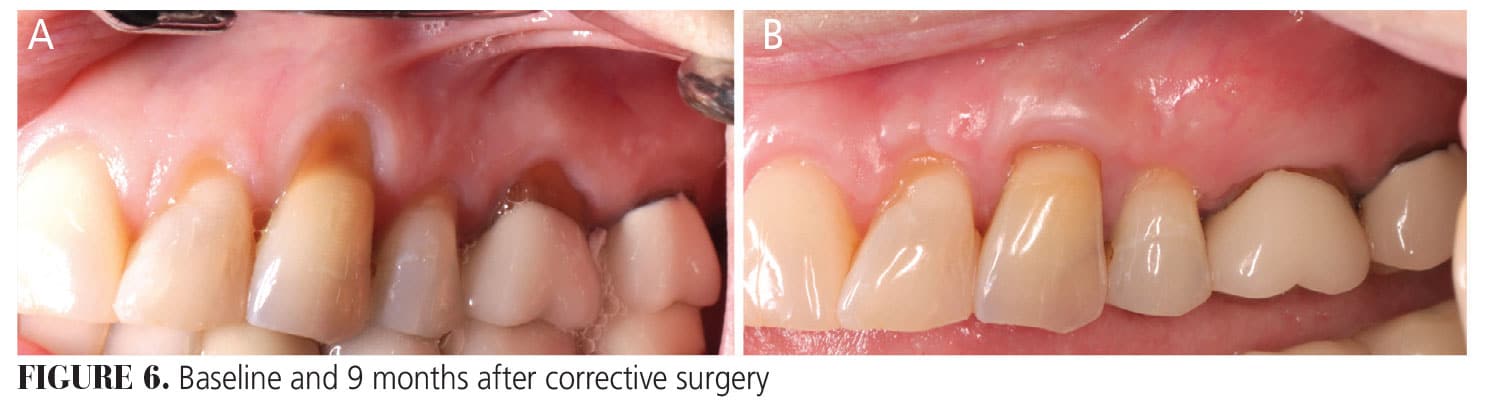
The healing was uneventful at both the recipient site and the donor site at 2 weeks (Figure 5A-B) Minimal discomfort and a significant reduction in sensitivity were reported at 8 weeks (Figure 5C). Complete root coverage was achieved on tooth #11, and the residual defect on #14 was less than 1 mm. All teeth presented with adequate KTW and thick gingival phenotype after 6 months post-surgery (Figure 5D). Treatment outcome remained stable at the 9-month follow-up (Figure 6). The patient was satisfied with the result.
DISCUSSION
This case report presents how infected ADM complications can be effectively managed with systemic antibiotics, local antiseptics, and corrective surgery. ADM’s therapeutic applications include phenotype modification, root coverage, and peri-implant soft tissue augmentation. ADM can be exposed as a FGG to increase the width of the attached gingiva and provide a more natural appearance.12 However, when ADM is used in a bilaminar technique for root coverage, it requires submerged healing to optimize healing and reduce infection risk.13
ADM’s healing process exhibits slower vascularization, less keratinization, and a longer inflammation period.14 Therefore, the uncovered portion of ADM is rarely taken, conversely, the porous surface of ADM is susceptible to bacterial colonization and infection. In contrast, CTG may be left partially exposed. The rate of complete root coverage will be favorable if the submerged-to-exposed ratio of the CTG is greater than 11:1.15
A retrospective study reported an infection rate of 3.66% in patients who had subepithelial tissue graft surgery.16 Pre- and post-operative CHX rinses can significantly reduce the intraoral bacterial load and infection rate.17
In this case, the patient was instructed to perform 10% PvI swabbing when the clinical infection signs were noticed. PvI is a good alternative to CHX, exhibiting a comparable wide-spectrum antiseptic effect to CHX with minimal cytotoxicity and less bacterial resistance.18 Local topical application was preferred to avoid stain formation. Acute infection following soft tissue grafting can be controlled by systemic antibiotic therapy, given that soft tissue grafts are more resistant to microbial challenge.19
Incomplete root coverage or worsening of the recession defect commonly occurs after complications of mucogingival surgery. When the patient is dissatisfied with the outcome, corrective surgery is indicated to correct the recession defect. The second attempt is usually more challenging, given that the scar tissue can limit the mobility of the flap.19 Any attempt to optimize the predictability of retreatment should be made, and the gold standard CAF + CTG should be prioritized. The envelope-CAF flap design was selected for second surgery in the present case because it provides better access for tension release than the tunneling technique. In this case, the de-epithelialized FGG (De-FGG) technique was applied to obtain the CTG. A randomized clinical trial demonstrated that post-operative morbidity for patients undergoing De-FGG harvesting was not significantly different from conventional CTG harvesting.20 Furthermore, De-FGG is associated with a higher mean root coverage rate compared to conventional CTG.21 In instances where autologous tissue is not an option, the combination therapy, allograft, or xenograft in conjunction with biologics can be an ideal alternative, biologics reduce pos-operative complications and enhance healing, particularly in complex recession defects and retreatment sites. Commonly used biologics for root coverage include enamel matrix derivatives (EMD), platelet-rich fibrin (PRF), and recombinant human platelet-derived growth factor-BB (rh-PDGF-BB).
Since the late 2000s, xenogeneic collagen matrices (XCM) have been tested as an alternative to autogenous grafts. Several studies have demonstrated the safety and efficacy of this new material, although the results are still inferior to autologous tissue. Researchers attribute this inferiority to its volume instability.22 Thus, volume-stable collagen matrix (VCMX) emerged, offering reliable short-term outcomes in gingival augmentation and aiding secondary healing and root coverage.23 The learning curve of manipulating VCMX can be challenging because of its fragile texture. VCMX is often used with rh-PDGF-BB. It serves as a carrier for rh-PDGF-BB due to its porous structure, thereby enhancing the substantivity of growth factors release.24
A growth factor, rh-PDGF-BB upregulates angiogenesis, chemotaxis, and mitogenesis, promoting periodontal and bone regeneration. Given its substantial regenerative potential, rh-PDGF-BB is used to manage challenging intrabony defects and severe ridge deficiency.25 Recently, it has also been applied in mucogingival surgery. Multiple trials showed promising short-term results when used with collagen matrix to treat complex gingival recession defects and multiple adjacent gingival recessions.26
EMD is a mixture of porcine-origin molecules, containing mainly amelogenin. EMD provides the benefits of chemotaxis, angiogenesis, and soft tissue thickening for root coverage. According to systematic reviews, when EMD was used as an adjunct to the coronally advanced flap, the root coverage outcome was comparable to CTG + CAF.27,28 EMD not only can be used alone as a graft substitute but also can be added to other graft materials to promote healing.
PRF is a second generation platelet concentrate with a prolonged release profile of growth factors.29 It provides accelerated soft tissue healing, reduced patient morbidity, and improved root coverage in root-coverage procedures.30 However, the efficacy of PRF reported in the literature should be interpreted cautiously, with the quality of PRF varying significantly based on the donor’s systemic health and centrifuge protocol. Different types of PRF can be produced to meet different clinical scenarios. For example, fluid-type PRF can be mixed with bone graft to create sticky bone for better handling. Fibrin-type PRF can be used as a membrane to increase wound stability.
In conclusion, complications caused by exposed ADM can be effectively managed through systematic antibiotics and local PvI application. Envelope-CAF + CTF successfully eliminated the residual recession.
References
- Romandini M, Soldini MC, Montero E, Sanz M. Epidemiology of mid-buccal gingival recessions in NHANES according to the 2018 World Workshop Classification System. J Clin Periodontol. 2020;47:1180-1190.
- Chambrone L, Tatakis DN. Long-Term Outcomes of Untreated Buccal Gingival Recessions: A Systematic Review and Meta-Analysis. J Periodontol. 2016;87:796-808.
- Cairo F, Nieri M, Pagliaro U. Efficacy of periodontal plastic surgery procedures in the treatment of localized facial gingival recessions. A systematic review. J Clin Periodontol. 2014;41 Suppl 15:S44-S62.
- Cortellini P, Bissada NF. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J Periodontol. 2018;89 Suppl 1:S204-S213.
- Chambrone L, Botelho J, Machado V, Mascarenhas P, Mendes JJ, Avila-Ortiz G. Does the subepithelial connective tissue graft in conjunction with a coronally advanced flap remain as the gold standard therapy for the treatment of single gingival recession defects? A systematic review and network meta-analysis. J Periodontol. 2022;93:1336-1352.
- McGuire MK, Janakievski J, Scheyer ET, et al. Efficacy of a harvest graft substitute for recession coverage and soft tissue volume augmentation: A randomized controlled trial. J Periodontol. 2022;93:333-342.
- Lu W, Qi G, Ding Z, Li X, Qi W, He F. Clinical efficacy of acellular dermal matrix for plastic periodontal and implant surgery: a systematic review. Int J Oral Maxillofac Surg. 2020;49:1057-1066.
- Chambrone L, Salinas Ortega MA, Sukekava F, et al. Root coverage procedures for treating localised and multiple recession-type defects. Cochrane Database Syst Rev. 2018;10:CD007161.
- Tavelli L, Barootchi S, Di Gianfilippo R, et al. Acellular dermal matrix and coronally advanced flap or tunnel technique in the treatment of multiple adjacent gingival recessions. A 12-year follow-up from a randomized clinical trial. J Clin Periodontol. 2019;46:937-948.
- Zucchelli G, De Sanctis M. Treatment of multiple recession-type defects in patients with esthetic demands. J Periodontol. 2000;71:1506-1514.
- Zucchelli G, Mele M, Stefanini M, et al. Patient morbidity and root coverage outcome after subepithelial connective tissue and de-epithelialized grafts: a comparative randomized-controlled clinical trial. J Clin Periodontol. 2010;37:728-738.
- Wei PC, Laurell L, Geivelis M, Lingen MW, Maddalozzo D. Acellular dermal matrix allografts to achieve increased attached gingiva. Part 1. A clinical study. J Periodontol. 2000;71:1297-1305.
- Tal H, Moses O, Zohar R, Meir H, Nemcovsky C. Root coverage of advanced gingival recession: a comparative study between acellular dermal matrix allograft and subepithelial connective tissue grafts. J Periodontol. 2002;73:1405-1411.
- Wei PC, Laurell L, Lingen MW, Geivelis M. Acellular dermal matrix allografts to achieve increased attached gingiva. Part 2. A histological comparative study. J Periodontol. 2002;73:257-265.
- Yotnuengnit P, Promsudthi A, Teparat T, Laohapand P, Yuwaprecha W. Relative connective tissue graft size affects root coverage treatment outcome in the envelope procedure. J Periodontol. 2004;75:886-892.
- Powell CA, Mealey BL, Deas DE, McDonnell HT, Moritz AJ. Post-surgical infections: prevalence associated with various periodontal surgical procedures. J Periodontol. 2005;76:329-333.
- Johnson NR, Kazoullis A, Bobinskas AM, Jones L, Hutmacher DW, Lynham A. Bacterial comparison of preoperative rinsing and swabbing for oral surgery using 0.2% chlorhexidine. J Investig Clin Dent. 2015;6:193-196.
- da Silveira Teixeira D, de Figueiredo MAZ, Cherubini K, de Oliveira SD, Salum FG. The topical effect of chlorhexidine and povidone-iodine in the repair of oral wounds. A review. Stomatologija. 2019;21:35-41.
- Mazzotti C, Mounssif I, Rendón A, et al. Complications and treatment errors in root coverage procedures. Periodontol 2000. 2023;92:62-89.
- Zucchelli G, Mele M, Stefanini M, et al. Patient morbidity and root coverage outcome after subepithelial connective tissue and de-epithelialized grafts: a comparative randomized-controlled clinical trial. J Clin Periodontol. 2010;37:728-738.
- Tavelli L, Ravidà A, Lin GH, Del Amo FS, Tattan M, Wang HL. Comparison between Subepithelial Connective Tissue Graft and De-epithelialized Gingival Graft: A systematic review and a meta-analysis. J Int Acad Periodontol. 2019;21:82-96.
- Rotundo R, Genzano L, Patel D, D’Aiuto F, Nieri M. Adjunctive benefit of a xenogenic collagen matrix associated with coronally advanced flap for the treatment of multiple gingival recessions: A superiority, assessor-blind, randomized clinical trial. J Clin Periodontol. 2019;46:1013-1023.
- Lee CT, Lange M, Jureidini A, Bittner N, Schulze-Späte U. Clinical and patient-reported outcomes after recession coverage using modified vestibular incision subperiosteal tunnel access with a volume-stable collagen matrix as compared to a coronally advanced flap with a subepithelial connective tissue graft. J Periodontal Implant Sci. 2022;52:466-478.
- Agis H, Collins A, Taut AD, et al. Cell population kinetics of collagen scaffolds in ex vivo oral wound repair. PLoS One. 2014;9:e112680.
- Urban IA, Tattan M, Ravida A, Saleh MH, Tavelli L, Avila-Ortiz G. Simultaneous alveolar ridge augmentation and periodontal regenerative therapy leveraging recombinant human platelet-derived growth factor-bb (rhpdgf-bb): a case report. Int J Periodontics Restorative Dent. 2022;42:577–585.
- Tavelli L, Barootchi S, Rodriguez MV, et al. Recombinant human platelet-derived growth factor improves root coverage of a collagen matrix for multiple adjacent gingival recessions: A triple-blinded, randomized, placebo-controlled trial. J Clin Periodontol. 2022;49:1169-1184.
- Cheng GL, Fu E, Tu YK, et al. Root coverage by coronally advanced flap with connective tissue graft and/or enamel matrix derivative: a meta-analysis. J Periodontal Res. 2015;50:220-230.
- Meza Mauricio J, Furquim CP, Bustillos-Torrez W, et al. Does enamel matrix derivative application provide additional clinical benefits in the treatment of maxillary Miller class I and II gingival recession? A systematic review and meta-analysis. Clin Oral Investig. 2021;25:1613-1626.
- Kobayashi E, Flückiger L, Fujioka-Kobayashi M, et al. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin Oral Investig. 2016;20:2353-2360.
- Chambrone L, Barootchi S, Avila-Ortiz G. Efficacy of biologics in root coverage and gingival augmentation therapy: An American Academy of Periodontology best evidence systematic review and network meta-analysis. J Periodontol. 2022;93:1771-1802.
From Decisions in Dentistry. January/February 2025;11(1):32-35.

