

Early Detection Is Key to Preserving Tooth Structure
Understanding the diagnosis, treatment, and prevention of dental cracks and fractures can help clinicians improve outcomes and enhance patients’ long-term oral health.
PURCHASE COURSE
This course was published in the January/February 2025 issue and expires February 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the January/February 2025 issue and expires February 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 070
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Differentiate between craze lines, cracked teeth, fractured cusps, split teeth, and vertical root fractures based on their clinical and radiographic characteristics.
- Identify effective diagnostic tools and techniques to accurately detect and assess the extent of cracks and fractures.
- Discuss evidence-based treatment plans tailored to the severity and prognosis of cracks and fractures, while educating patients on prevention and long-term maintenance strategies.
Since the onset of the COVID-19 pandemic, the incidence of dental cracks and fractures has increased.1 Early detection and intervention of these cracks and fractures may help preserve natural tooth structure, avoid infections, and maintain overall oral health. By addressing these issues promptly, dental professionals can help prevent the need for more extensive and costly procedures, thereby improving outcomes and overall patient satisfaction.
Effective treatment aids in restoring functionality and esthetics and enhancing quality of life. Further, educating patients about the etiologies and prevention of cracks can help minimize complications, lead to better long-term oral health, and improve economic efficiency.
Craze lines involve the enamel only. Cracks are partial discontinuities in both enamel and dentin with variable depth and extension. Conversely, fractures are complete discontinuities of enamel, cementum, and/or dentin and can arise in individual tooth cusps, crowns, and/or roots. In early stages, teeth with cracks and fractures generally have vague and intermittent signs and symptoms and therefore may go undiagnosed or misdiagnosed. In later stages, cracks and fractures are more easily identified; however, at this point the condition may have progressed and require more aggressive treatment.
Craze Lines
Craze lines are superficial disruptions in the enamel only, and do not present with any symptoms or radiographic manifestations (Figure 1). Thermocycling and excessive occlusal forces have been theorized to contribute to craze line formation.2 In anterior teeth, craze lines often present in a vertical direction, while in posterior teeth, they may be seen crossing the marginal ridge or extending along buccal and lingual surfaces.3 Craze lines can be differentiated from actual cracks and fractures through transillumination, which involves shining a light through the tooth. If both segments of the tooth are illuminated, as opposed to just one segment, this is a craze line. Craze lines are not likely to progress into the dentin, and therefore do not require any treatment.2

Fractured Cusps
Fractured cusps are discontinuities of both the enamel and dentin of a single cusp of a tooth that may or may not involve the pulp. These are often characterized by sharp pain upon mastication and/or a cold stimulus due to the resulting fluid movement within the dentinal tubules.4 Most often, the pain is felt upon release rather than from biting down. Although fractured cusps typically do not extend into the pulp, they may cause reversible pulpitis symptoms, characterized by an exaggerated sensitivity to cold without lingering. The patient is usually unable to identify which cusp is affected and will only report intermittent pain in the area.5 For cuspal cracks and fractures that are more difficult to visualize, using a plastic wedged bite stick can help identify the affected cusp by having the patient “squeeze and release” on each individual cusp tip (Figure 2).
If a fracture line is supragingival, the cusp may separate from the rest of the tooth due to occlusal forces. If the fracture line extends subgingivally, the gingival and periodontal fibers may cause retention of the fractured cusp. Wedging an explorer into the fracture line will cause a temporary separation of the fragment, making the fracture line more visible. Pain will often subside once the involved cusp fractures off completely.2
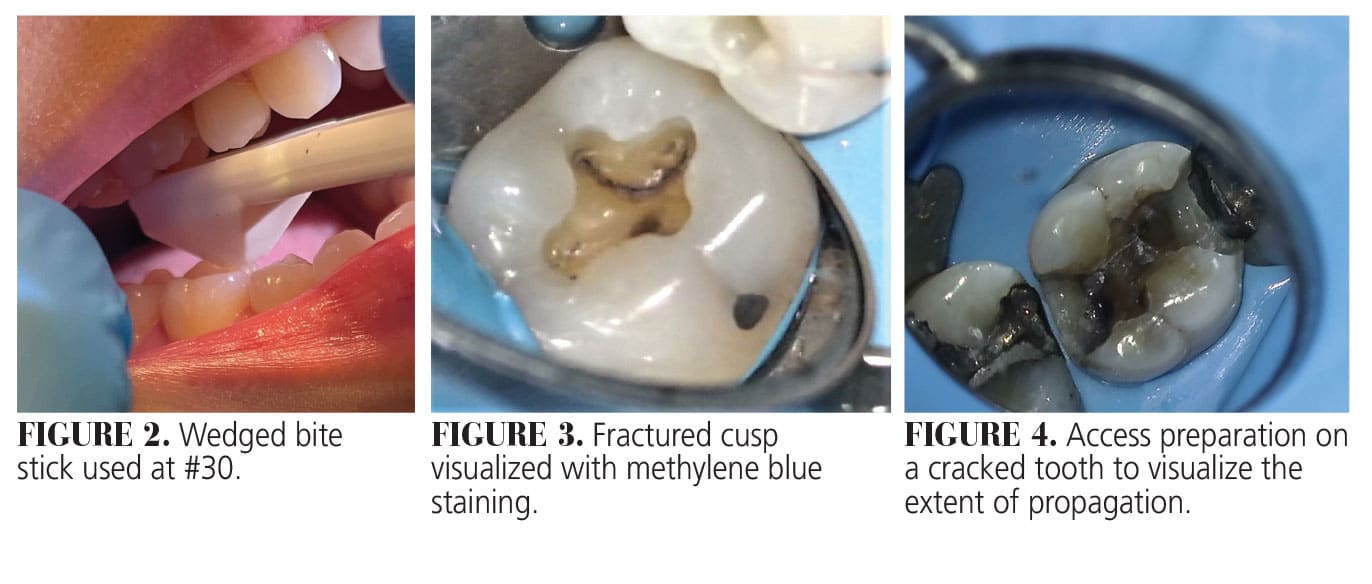
Fractured cusps are not identifiable radiographically and are difficult to visualize clinically. Removal of restorative material at the site of the suspected fracture may allow for better visualization. Transillumination or methylene blue staining with magnification can also aid in detection (Figure 3).2
The treatment for fractured cusps depends on the amount of tooth structure remaining as well as the pulpal and periapical diagnoses.2 If the pulp tests normally and the tooth is restorable, treatment involves placement of a crown.
Cracked Teeth
Cracked teeth have partial discontinuities in enamel and dentin that involve multiple cusps or the entire coronal portion of the tooth. Generally, mandibular molars, maxillary premolars and maxillary first molars are the most likely teeth to be involved.6 The symptoms of a cracked tooth depend on the extent of the crack and the pulpal diagnosis. Cracks that do not extend to or near the pulp will likely be asymptomatic, whereas deeper cracks will often present with acute pain upon mastication and cold stimuli.2
Determining the extent of the crack propagation is essential for assessing the tooth prognosis and treatment options. Transillumination, magnification, and methylene blue staining are effective at visualizing the length and location of the crack. If a restorative material is present at the site, it should be removed for better visualization. If the crack is centered, an access preparation may be required to determine the extent of the propagation (Figure 4). Wedging forces may also reveal if the tooth segments are separable and therefore considered to be a split tooth.2
Compared to a fractured cusp, the fracture line in a cracked tooth is generally more centered, extending in a mesiodistal direction and may involve the marginal ridges and proximal areas. This directionality makes cracks challenging to detect radiographically. However, the bone loss that occurs adjacent to the crack may become visible on the radiograph over time.2
Cracked teeth are often minimally restored or unrestored. Prolonged traumatic occlusal forces from mastication, excessive occlusal wear, and parafunctional habits are significant etiological factors, frequently leading to multiple cracked teeth. These patients should be prescribed an occlusal splint to prevent further damage to their dentition.2,7 Krell and Caplan8 evaluated the success rates of teeth with varying fracture locations and probing depths and found that teeth with a probing depth of greater than or equal to 5 mm and/or teeth with a distal marginal ridge fracture were associated with a poorer prognosis.
Treatment decisions for cracked teeth depend on the extent of crack propagation and the pulpal and periapical diagnoses. On a tooth that is deemed restorable, an endodontic diagnosis of irreversible pulpitis or pulpal necrosis necessitates endodontic treatment and subsequent full-coverage restoration. However, if these teeth present in conjunction with narrow deep periodontal defects, this likely indicates a deeper crack extension and a lowered prognosis.7,8 New technologies are emerging that may help clinicians discern between an intact and a cracked tooth.
Research suggests that cracked teeth with a diagnosis of normal pulp or reversible pulpitis treated with a single-stage direct or indirect restoration — without endodontic treatment — can expect pulp survival rates of 93% over 6 to 7 years of follow up.7 Further, cracked teeth with a pulpal diagnosis of reversible pulpitis treated with definitive full-coverage restoration, without endodontic treatment, had a success rate of 80%, with only 20% of these teeth needing root canal treatment.6,9
Split Tooth
Split teeth are defined as complete discontinuities of coronal tooth structure that extend apically. These types of fractures are typically oriented in a mesiodistal direction and involve one or both marginal ridges. When the propagation of the fracture extends through the floor of the pulp chamber resulting in separate tooth fragments, this is considered a split tooth.2
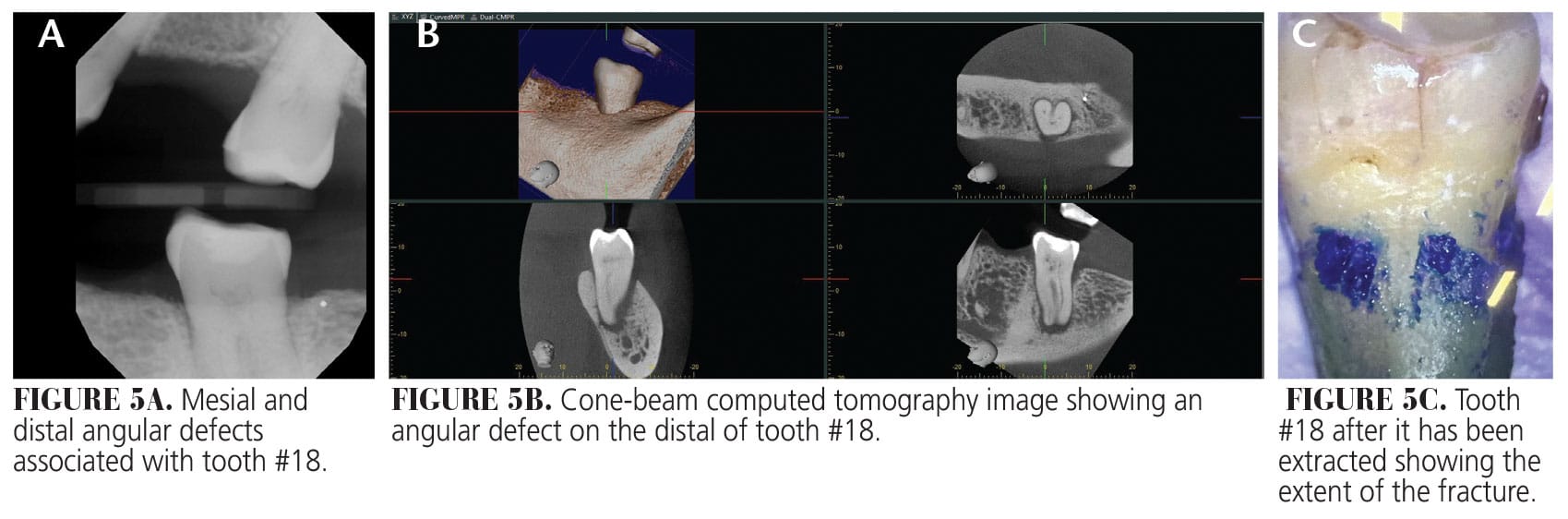
Clinically, bone loss and periodontal defects are signs of split teeth. Vertical loss of the interproximal or interradicular bone may be seen on periapical radiographs or cone-beam computed tomography (CBCT) imaging.2 The presence of angular defects on the CBCT image and an intact buccal cortical plate can help to differentiate a split or cracked tooth from a vertical root fracture (Figures 5A to C).10
Generally, mandibular second molars, mandibular first molars, and maxillary first molars are the most common cracked and split teeth.2 Visible separation of fragments when wedging with an explorer indicates that the fracture has propagated to a tooth surface. Deep periodontal probing depths adjacent to the fracture are often found clinically.2
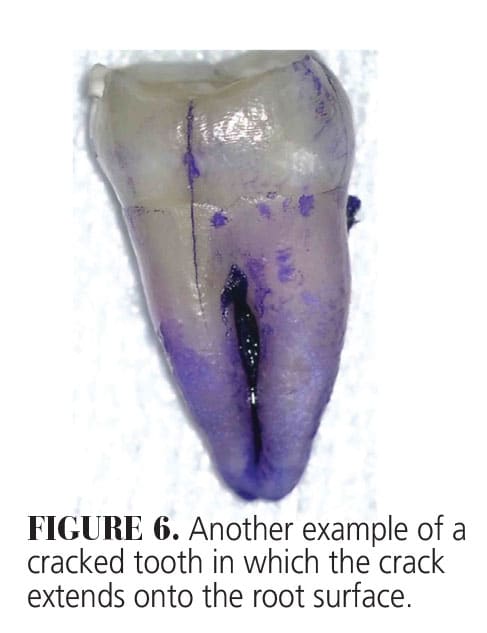
Treatment options for split teeth are limited. If the fracture line extends deep toward the apex of the tooth, the tooth must be extracted (Figure 6).
Vertical Root Fracture
A vertical root fracture (VRF) is a complete or incomplete separation of tooth structure originating in the root, usually occurring in a buccal-lingual direction.2 Roots with smaller mesiodistal diameters and deep oval cross-sections, such as maxillary premolars and the mesial roots of mandibular molars, are more prone to VRF.11 Additionally, increasing canal curvature has also been associated with an increased susceptibility to VRF.12
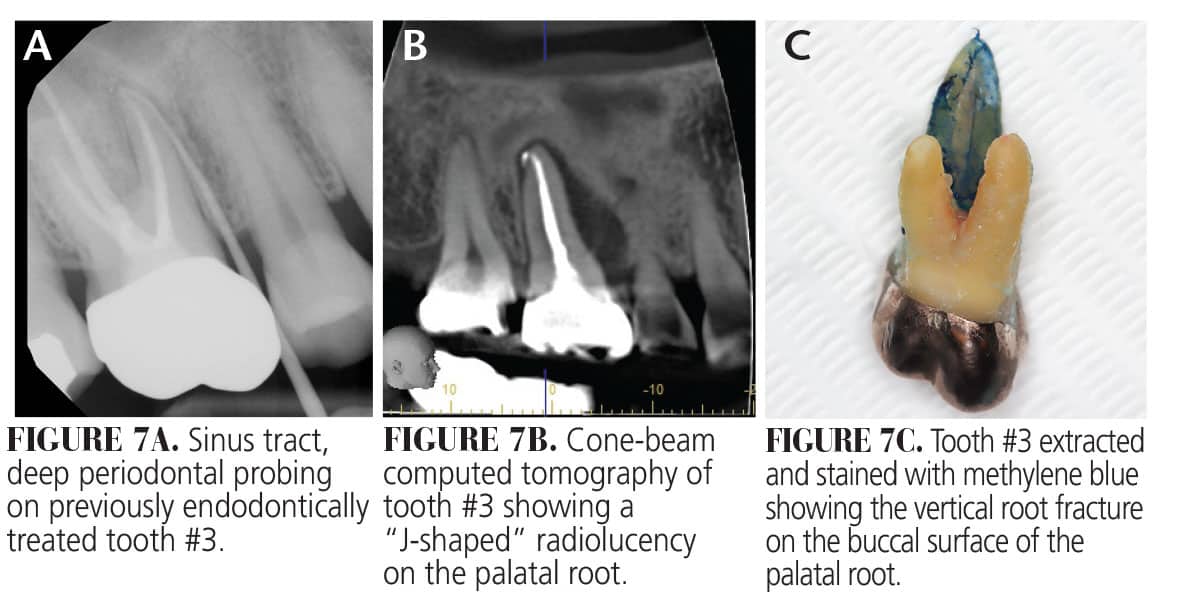
There are four typical signs of a tooth with a vertical root fracture:13
- Previous endodontic treatment
- “J-shaped” or “halo” radiolucency around the root
- Presence of a sinus tract
- Isolated, deep periodontal pocket
VRFs are found in endodontically treated teeth. Excessive removal of tooth structure during root canal preparation and excessive force during obturation can contribute to loss of structural integrity in root dentin.11 The placement of posts for intracanal retention also increases the likelihood of fracture due to lateral wedging forces on root dentin.14-18 Endodontic irrigants, instrumentation of root canal, and thermal stresses during obturation may also induce the formation of microcracks, which can propagate over time, much like a crack in the windshield of a car.16 Vertical root fractures are intraosseous, making them difficult to visualize on intraoral radiographs or on endodontic examination (Figure 7A-C).
CBCT images are more accurate than periapical radiographs when visualizing the characteristic defects associated with VRF.19,20 These characteristic defects include:
- “J-shaped” bone loss10
- Complete separation of the root fragments10,11,21
- Complete loss of the buccal and/or lingual/palatal cortical plate22
- Radiolucency around a root where a post terminates22
- Loss of cortical bone at a mid-root level either buccally or lingually indicating origin point. Coronal and apical extension of mid-root radiolucency indicate advanced lesion22
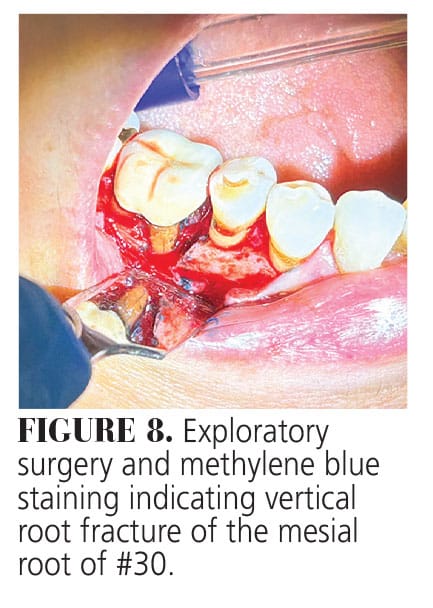
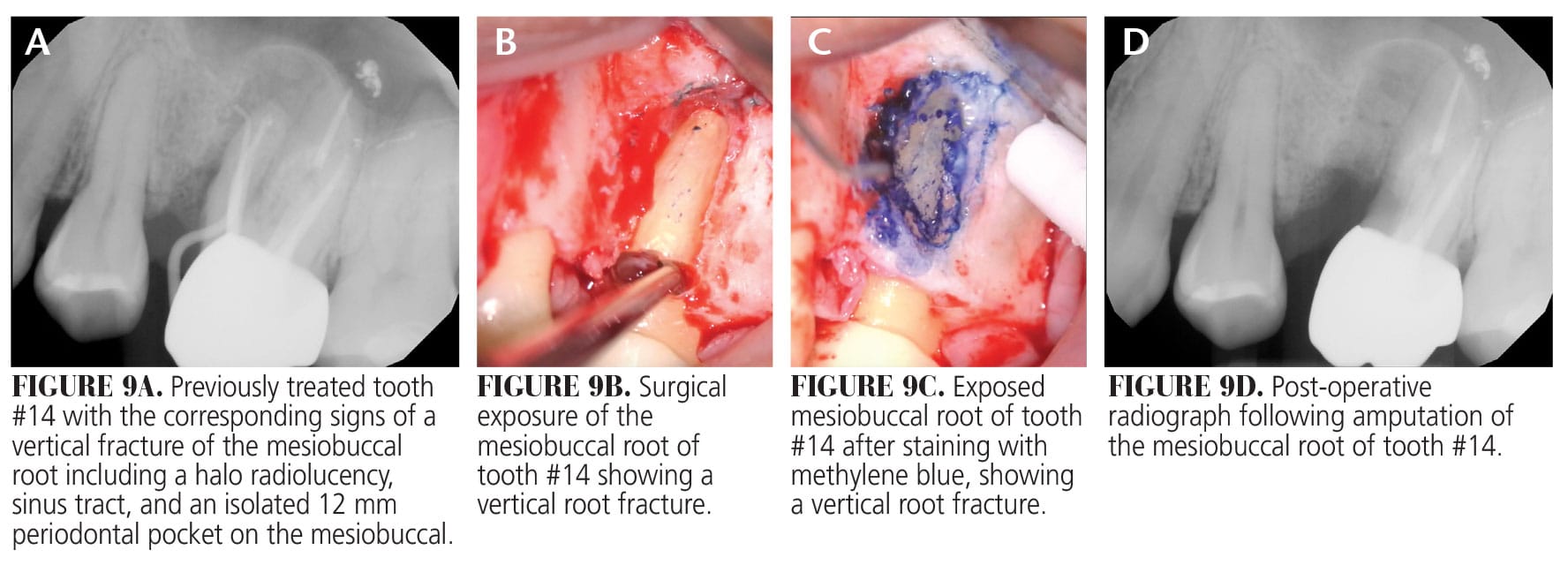
The most accurate method of determining the presence of a VRF is exploratory surgery and staining with methylene blue (Figure 8). A conservative flap and gentle retraction of the tissue can be done to facilitate visual confirmation.14,21 The most accepted treatment modality is extraction of the vertically fractured tooth. If the vertical root fracture involves only one root of a multirooted tooth, root amputation, resection or hemisection may be a viable option (Figure 9A-D).11,23
Conclusion
The increase in the number of dental cracks and fractures since the onset of the COVID-19 pandemic underscores the importance of their early detection and intervention. The use of a surgical operating microscope with high magnification and illumination, the use of transillumination, and the use of CBCT increases the clinician’s ability to more accurately diagnose cracks and fractures as well as to better determine the long-term prognosis of the tooth or teeth in question. Further, these microscopic and CBCT images can be used as tools to better educate patients on the risks, benefits, and alternative treatment options, thereby helping them make an informed treatment decision about their cracked or fractured tooth.24,25 Lastly, educating patients on prevention and the potential consequences of untreated cracks can enhance long-term oral health and reduce the need for complex, costly treatments.26
Acknowledgments
The authors would like to thank Ankita Kathpalia, DDS; Gabriel Murphy, DMD; Neha Dawar, DDS; Ahmed Salman, DDS, MSD; Mia Tittle, DDS, MSD; Gretchen Bruce, DDS; and Amro Elkhatieb, DDS; for providing the images that accompany this article.
References
- Nosrat A, Yu P, Verma P, et al. Was the coronavirus disease 2019 pandemic associated with an increased rate of cracked teeth? J Endod. 2022;48:1241-1247.
- Rivera EM, Walton RE. Longitudinal tooth cracks and fractures: an update and review. Endod Topics. 2015;33:14-42.
- Hasan S, Singh K, Salati N. Cracked tooth syndrome: overview of literature. Int J Appl Basic Med Res. 2015;5:164-168.
- Brännstrom M, Lindén LA, Aström A. The hydrodynamics of the dental tubule and pulp fluid: a discussion on its significance to dential sensitivity. Caries Res. 1967;1:310-317.
- Hargreaves KM, Berman LH. Cohen’s Pathways of the Pulp. St, Louis: Elsevier; 2020:848-869.
- Krell KV, Rivera EM. A six-year evaluation of cracked teeth diagnosed with reversible pulpitis: treatment and prognosis. J Endod. 2007;33:1405-1407.
- Kakka A, Gavriil D, Whitworth J. Treatment of cracked teeth: A comprehensive narrative review. Clin Exp Dent Res. 2022;8:1218-1248.
- Krell KV, Caplan DJ. 12-month success of cracked teeth treated with orthograde root canal treatment. J Endod. 2018;44:543-548.
- Olivieri JG, Elmsmari F, Miró Q, et al. Outcome and survival of endodontically treated cracked posterior permanent teeth: a systematic review and meta-analysis. J Endod. 2020;46:455-463.
- Alaugaily I, Azim AA. CBCT patterns of bone loss and clinical predictors for the diagnosis of cracked teeth and teeth with vertical root fracture. J Endod. 2022;48:1100-1106.
- Liao WC, Chen CH, Pan YH, et al. Vertical root fracture in non-endodontically and endodontically treated teeth: current understanding and future challenge. J Pers Med. 2021;11:1375.
- Lertchirakarn V, Palamara JEA, Messer HH. Patterns of vertical root fracture: factors affecting stress distribution in the root canal. J Endod. 2003;29:523-528.
- Tamse A. Vertical root fractures in endodontically treated teeth: diagnostic signs and clinical management. Endod Topics. 2006;13:84-94.
- Alamri HM, Altamimi A, Mirza MB, et al. Detecting Vertical Root Fractures Using Modified Methylene Blue Dye: A Preliminary In Vitro Study. Healthcare (Basel). 2023;11:504.
- Meister Jr F, Lommel TJ, Gerstein H. Diagnosis and possible causes of vertical root fractures. Oral Surg Oral Med Oral Pathol. 1980;49:243-253.
- Yap RC, Alghanem M, Martin N. A narrative review of cracks in teeth: Aetiology, microstructure and diagnostic challenges. J Dent. 2023;138:104683.
- Sorenson JA, Engelman MJ. Effect of post adaptation on fracture resistance of endodontically treated teeth. J Prosthet Dent. 1990;64:419-424.
- Govare N, Contrepois M. Endocrowns: a systematic review. J Prosthet Dent. 2020;123:411-418.
- Dias DR, Iwaki LCV, de Oliveira ACA, et al. Accuracy of high-resolution small-volume cone-beam computed tomography in the diagnosis of vertical root fracture: an in vivo analysis. J Endod. 2020;46:1059-1066
- Edlund M, Nair MK, Nair UP. Detection of vertical root fractures by using cone-beam computed tomography: a clinical study. J Endod. 2011;37:768-772.
- Moule AJ, Kahler B. Diagnosis and management of teeth with vertical root fractures. Aust Dent J. 1999;44:75-87.
- Fayad MI, Ashkenaz PJ, Johnson BR. Different representations of vertical root fractures detected by cone-beam volumetric tomography: a case series report. J Endod. 2012;38:1435–1442.
- Salihu B, Stavileci M. Review of approaches to the management of vertical dental root fractures and tooth preservation. Med Sci Monit. 2024;30:e943100-1–e943100-7.
- Rivera E, Walton RE. Longitudinal tooth fractures: findings that contribute to complex endodontic diagnosis. Endodontic Topics. 2007;16(1):82-111.
- Kim JH, Eo SH, Shrestha R, Ihm JJ, Seo DG. Association between longitudinal tooth fractures and visual detection methods in diagnosis. J Dent. 2020;101:1-5.
- Li F, Diao Y, Wang J, et al. Review of cracked tooth syndrome: etiology, diagnosis, management and prevention. Pain Res Manag. 2021;1:3788660
From Decisions in Dentistry. January/February 2025;11(1):28-31.

