

Impact of Substance Use Disorders On Oral Health: A Case Report
The physical, psychological, and socioeconomic factors surrounding substance use disorders often contribute to dental health deterioration, but successful treatment is available for patients in recovery
Drug use damages many parts of the body such as the oral cavity, lungs, liver, brain, and heart. Drug addiction is defined as physical and psychological dependence on psychotic substances (eg, alcohol, tobacco, heroin) that cross the blood-brain barrier once ingested, temporarily altering the chemical milieu of the brain.1,2
Individuals with substance use disorders experience physical, psychological, emotional and behavioral problems.2 Long-term drug addiction may cause dry mouth and the clenching or grinding of teeth, particulary among those who use stimulants.3 The use of illicit drugs — such as methamphetamine and heroin — often leads to the absence of regular oral hygiene and lack of dental care.
Smoking is common among those with substance use disorders, exacerbating negative effects on oral health. The use of opioids can result in the suppression of pain responses, causing patients to ignore the signs of dental caries, periodontal diseases, and other potential life-threatening oral lesions.
Additionally, the effects of local anesthesia may be minimized among patients with opioid addiction. When used together, local anesthesia and opioids produce “synergistic” analgesia. While the mechanism of this interaction remains unclear since the cellular effects of opioids differ from those of local anesthetic, the potential of opioids to decrease the effectiveness of local anesthetics can lead to unpredictable perioperative outcomes and complex post-operative patient management.4
Oral health professionals are well aware of the ravages brought on by substance use disorders. According to the National Institutes of Health, dental health problems are “among the most prevalent health problems associated with drug addiction.” 5 People with substance use disorders have elevated prevalence of oral diseases, in particular dental caries, periodontal diseases, and xerostomia. When left untreated, these oral health conditions may lead to tooth ache, abscesses, and tooth loss, and, in turn, to poor chewing and digestion. Ultimately, dental esthetic problems and reduced quality of life are also inevitable outcomes.
The main drivers of oral diseases and their progression — poor oral hygiene, frequent sugar intake, and infrequent dental visits — can mainly be ascribed to the irregular lifestyle, low socioeconomic status, and mental health problems that often accompany substance use disorders.6,7
Many substances have devasting consequences on oral health. Some commonly used illicit drugs directly affect the oral cavity. Cocaine can cause movement disorders and transient chorea. In addition, buccolingual dyskinesia may also be present. Regular snorting of cocaine may have severe orofacial effects, such as perforation of the nasal septum and palate, gingival lesions, and erosion of the tooth surfaces.
In the case of heroin use, increased numbers of decayed, missing, and filled teeth are common. This can result from chronic malnutrition, poor oral hygiene due to impaired motor function and neuropathology secondary to infection, vasculitis, septic emboli, thromboembolism, prolonged heroin-induced respiratory depression, hypotension, positional vascular compression, acute Parkinsonism, and spongiform leukoencephalopathy.
Marijuana use can lead to acidic erosion of enamel due to cannabinoid hyperemesis, in which frequent episodes of vomiting occur. In addition, these patients develop dental caries, inflammation, and hyperplasia of the gingival tissue, leukoplakia, oral papillomas, and tongue carcinoma.
In chronic use of methamphetamine, the result is large carious lesions on buccal smooth surface areas and fractured teeth due to increased motor activity.1 Oral effects caused by 3, 4-methylenedioxy-N-methamphetamine (MDMA), or ecstasy include mucosal changes, xerostomia, and dental erosion and bruxism.8
Tobacco is a known risk factor for the development of oral and periodontal diseases. Its use is associated with increased pocket depth, loss of periodontal attachment, loss of alveolar bone, and increased tooth loss. Individuals who smoke also have a much higher risk of oral cancer.
Prolonged and/or heavy use of alcohol increases the risk for tooth decay and periodontal diseases due to the lack of good oral hygiene in individuals who are impaired while drinking. Alcohol is also tied to malnutrition and changes in the oral flora resulting in increased decay and periodontal diseases. The risk of oropharynx cancer also increases with the amount of alcohol consumed.
Case Report
radiograph.
On December 28, 2020, a 39-year-old man, TT, presented to the office for a comprehensive exam. In 2019, at age 37, he reported that he lost all his dentition due to multiple broken and/or badly decayed teeth caused by a substance use disorder. At that time, he received a full maxillary and mandibular removable denture, which he has worn since then.
His chief complaint now is that his dentures are loose, he cannot chew very well, and consistent discomfort. In order to obtain additional information about his health history and habits, TT was placed into a private office to continue the consultation.

computed tomography volumetric
rendering.
Significant Medical History. He initially started using marijuana, opioids, and MDMA at age 15. While the marijuana and opioids were used several times per week, the MDMA was taken daily. At age 20, he advanced to methamphetamine and heroin, which led to two overdoses. At age 22, he was placed in rehabilitation which was unsuccessful. Between the ages of 22 and 36, TT was placed in rehabilitation programs an additional 23 times for various periods. During this same time frame, he was admitted into a psychiatric facility four times and placed on several different selective serotonin reuptake inhibitors.
In 2019, he received inpatient treatment at the Cleveland Clinic at which time all of his teeth were removed and his current dentures were fabricated. TT also advised the dental providers that he had acquired immunodeficiency syndrome (AIDS). TT disclosed a history of kidney stones. He was currently taking two prescription drugs: 20 mg of a proton-pump inhibitor for gastroesophageal reflux and abacavir/dolutegravir/lamivudine, a retroviral medication used to treat AIDS.
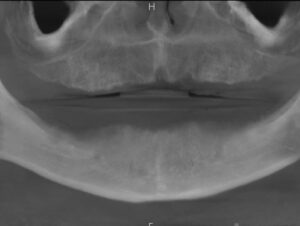
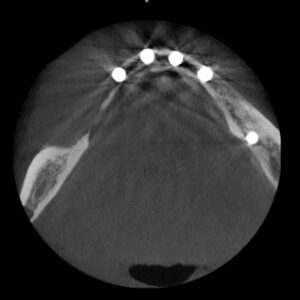
Dental Evaluation. TT returned to the dental operatory where a detailed oral exam was done along with a panoramic radiograph (Figure 1) and a cone-beam computed tomography (CBCT) of his oral cavity revealing his residual maxillary and mandibular ridges (Figure 2).
implant placement.

A detailed treatment plan was presented, which included the placement of implants in both of his arches with the probability of bone augmentation, especially in the maxilla. After appropriate healing time, locators would be placed on the implants, the existing dentures would be hollowed out in the implant areas, and quick cure acrylic would bond the locator retentive housings into the dentures. The outcome would a be stable, implant-supported removable maxillary and mandibular dentures. TT said he would think about it and get back to us.
Treatment. Almost 2 years later, on August 26, 2022, TT returned to the office for an exam and to discuss the proposed treatment plan. He stated he has been in long-term recovery for 3 years and wants to move forward with the original treatment plan.
This was confirmed by contacting the Cleveland Clinic where he has remained in active treatment and in a support program since 2019. Understanding the possibility of relapse and the need to minimize the use of any mood-altering medication,9 an additional consultation was made with clinicians at the Cleveland Clinic program.
With due consideration of his history and the complexity of the surgical procedure, TT was prescribed amoxicillin 500 mg, #30, q8h starting the morning before surgery until gone, acetaminophen #3, #12 prn, and diazepam 10 mg, #2 to be taken 40 minutes prior to the surgery. TT stated that he understood the proposed treatment plan, signed the surgical consent form, and scheduled the first procedure: placement of five implants in his mandibular arch.
On September 2, 2022, TT returned to start his treatment. After a review of the procedure, he was given local anesthetic, lidocaine 2% 1:100,000 and articaine HCl and epinephrine 4% 1:100,000, and profound anesthesia was obtained. Based on the CBCT, the team decided against placing any implants on his mandibular right side due to the amount of grafting that would be required to augment the extensive bone loss in this area and his current immune-compromised health status.
After reflection of the soft tissue, the following implants were placed: #18 – 4.7X8, #s 22, 24, 25, and 26 – 4.2X10 (Figure 3). Polytetrafluoroethylene (PTFE) sutures were used to close the surgical site and TT was scheduled to return in 3 weeks for suture removal.
On September 26, 2022, TT returned to the office. Everything was healing normally, the sutures were removed, and he was scheduled for exposure of the mandibular implants and placement of the locators on all implants. On October 17, 2022, TT returned for exposure of his mandibular implants and placement of the attachments. In addition, his existing denture was hollowed out in the implant areas, retentive metal housings were secured in the denture (Figure 4), and minor occlusal adjustments were made as needed.
placement.

TT was given detailed hygiene instructions in the care of his implants/denture. Also, he was given the same prescriptions as before and scheduled for the maxillary arch surgery. TT informed the office that he had forgotten to include an important medical issue on his health history: due to his long-term substance use, he only has 30% kidney function and therefore cannot take ibuprofen.
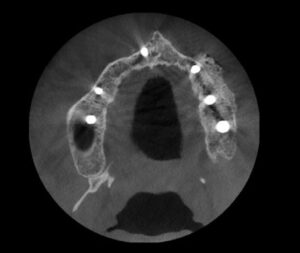
Based on this new medical information, clearance was obtained from his attending physician before continuing with his treatment. On December 9, 2022, TT returned for placement of his maxillary implants. Under local anesthesia, the soft tissue was reflected and the following implants were placed: #3 – 3.7X11, #6 – 3.2X13, #8 – 3.2X10, #11 – 3.2X13, #13 – 3.7X11 and #15 – 4.2X11 (Figure 5).
radiograph.
Minor bone grafting with mixed freeze dried cortical and cancellous graft material was placed in each area and then covered with cytoplasmic resorbable membrane. Primary closure was obtained using PTFE sutures. The sutures were removed in 3 weeks and everything was healing normally.
On February 14, 2023, TT returned to have the maxillary implants exposed and attachments placed. After exposing the implants, locators were placed and the maxillary denture was hollowed out in the implant areas (Figure 6). The metal housings were placed on the locators and picked-up using a quick cure acrylic. After minor adjustments were made, the palate of the maxillary denture was removed. Detailed hygiene instructions were once again given and he was scheduled for a recare exam in 2 weeks.

beam computed tomography
volumetric rendering.
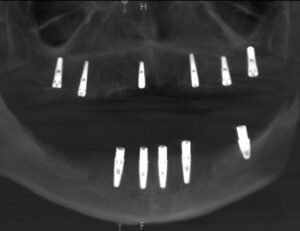
On December 28, 2022, TT returned to the office. A panographic radiograph (Figure 7) and a CBCT (Figure 8) revealed that all the implants and graft material appeared to be integrated.
The patient reported that the discomfort was gone, he could eat anything he wanted, and was very happy with the results (Figure 9.) TT was then placed on 3-month recare for the next 2 years so he could be monitored to ensure patient compliance with oral hygiene and implant maintenance.
Conclusion
Dentists and their team members should be aware of the frequency of which they may see patients with substance use disorders. Patients with substance use disorders typically have acute dental needs and may be reluctant to visit the dentist.

The patient’s medical and social history should be discussed in a nonjudgmental manner. Many times, this needs to be done in a private setting, not in the operatory with other employees present. Letting patients know the importance of this information for their personal treatment may help them feel comfortable enough to provide their full history, not just what they put on the office new patient or recare documents. Dentists, much like all healthcare professionals, need to remain up-to-date on substance use disorders so they can provide the best care possible for their patients.
key takeaways
- Drug use has significant health effects particularly on the oral cavity, lungs, liver, brain, and heart.
- Drug addiction is characterized by both physical and psychological dependence on substances that affect the brain’s chemical balance.
- Long-term substance use can result in oral health issues such as dry mouth, teeth clenching or grinding, and neglect of dental care.
- Patients with substance use disorders may present challenges in dental treatment. plants. Their medical history and health considerations, including compromised immune systems and potential medication interactions, need to be carefully managed during treatment planning and execution.
References
- McFarland s, Giannini PJ, Fung EYK. Addiction and oral health care. Decisions in Dentistry. 2018;4(1):50–53.
- Saini GK, Gupta ND, Prabhat KC. Drug addiction and periodontal disease. J Indian Soc Perio. 2013;17:587–591.
- American Dental Association. Methamphetamine. Available at: ada.o/g/resources/research/science-and-research-institute/oral-health-topics/methamphetamine. Accessed August 4, 2023.
- Ruvins E, Stein M, Kayserman, Brydon KG. Opioids’ impact on dental anesthesia. Decisions in Dentistry. 2023;9(3):26-29.
- Vertava Health. Dental Health and Addiction: How Different Substances Affect Oral Wellness. Available at: vertavahealth.com/addiction-resources/dental-health-and-addiction. Accessed August 4, 2023.
- Rossow I. Illicit drug use and oral health. Addiction. 2021;116:3235–3242.
- Oral Health Foundation. Drugs, Alcohol and Your Oral Health. Available at: dentalhealth.org/drugs-alcohol-and-your-oral-health. Accessed August 4, 2023.
- Brand HS, Dun SN. Ecstasy (MDMA) and oral health. J Br Dent. 2008;204:77–81.
- Myers J, Compton P. Addressing the potential for perioperative relapse in those recovering from opiod use disorder. Pain Med. 2018;19:1908–1915.
From Decisions in Dentistry. September 2023; 1(8):14-19
