

Healing Progression of the Free Gingival Graft
This clinical chronicle demonstrates the day-to-day healing of a free gingival graft, and correlates the visual presentation with the histology of the healing wound.
PURCHASE COURSE
This course was published in the October 2020 issue and expires October 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the October 2020 issue and expires October 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the concept of periodontal phenotypes, and clinical uses for free gingival grafting procedures.
- Describe the clinical presentation of the wound during various stages of free gingival graft healing.
- Identify the most critical postsurgical time period for a free gingival graft.
The term periodontal phenotype, first proposed by Müller and Eger,1 includes the three-dimensional gingival volume and thickness of the buccal/facial bone plate. Periodontal phenotype has been proposed to replace the term gingival biotype.2 By definition, biotype is genetically predetermined and cannot be modified by clinical interventions.2 In contrast, periodontal phenotype can be changed by surgical intervention, relying primarily on soft and/or hard tissue augmentation, such as a free gingival graft. Clinically, two periodontal phenotypes are identified: thin and thick. Systematic reviews report an association of thin phenotype with diminished thickness of underlying bone and an increased risk of gingival recession.3–5 Conversely, a thick phenotype appears more resistant to gingival recession and is associated with more favorable clinical outcomes following surgical root coverage.4–6
Various grafting procedures have been used to convert a thin periodontal phenotype to a thick phenotype. In this regard, the free soft tissue autogenous graft is a long-standing procedure used to achieve several clinical endpoints; these include increasing the width of keratinized and attached gingiva, deepening the facial/buccal vestibular depth, dissipating muscle and frenulum pull, covering exposed root surfaces, and converting a thin periodontal phenotype to a thick phenotype.7,8 Numerous articles regarding surgical techniques and the rationale for use of the free gingival graft have been published;9–11 papers have also addressed the stages of clinical and histologic healing.12–17 However, no article has comprehensively chronicled the day-to-day healing of the free gingival graft. For patients (as well as providers not familiar with the healing process), the graft can appear to have failed during the first few days postsurgery. While clinicians can find literature explaining surgical grafting technique,18,19 this paper will focus on the progression of healing and correlate its appearance with the histology of the healing wound.
![]() CLINICAL CONSIDERATIONS
CLINICAL CONSIDERATIONS
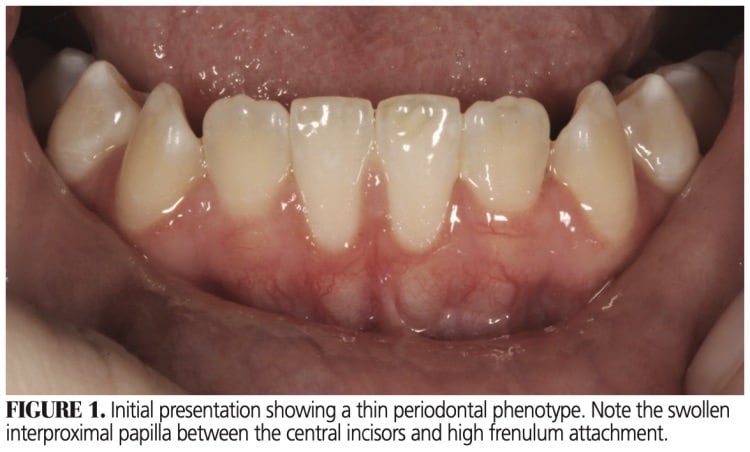
A typical patient with a thin periodontal phenotype overlying the mandibular central incisors is depicted in Figure 1. In this type of case, generally there is thin or no facial bone, and the height of root surface convexity is positioned outside the alveolar housing. Such root-bone architecture can be verified by cross-sectional cone beam computed tomography, but is usually clinically evident. The situation may become even more problematic due to a prominent labial midline frenulum, gingival recession (with varying degrees of root exposure), gingival inflammation, and complicating treatments, such as orthodontic therapy.
There are multiple options for converting a thin periodontal phenotype to a thick phenotype, including free gingival graft, subepithelial connective tissue graft (CTG), and coronally positioned flaps combined with autogenous, allogenic or xenograft augmentation. In the case presented here, a free gingival graft was chosen to accomplish the goals of therapy with the least risk of failure. Given the nonelastic character of thin mucosa and lack of facial bone, a mucoperiosteal flap reflection to accommodate a CTG was considered a risky procedure subject to further tissue loss and an increased chance of failure.
![]() PROGRESSION OF HEALING
PROGRESSION OF HEALING
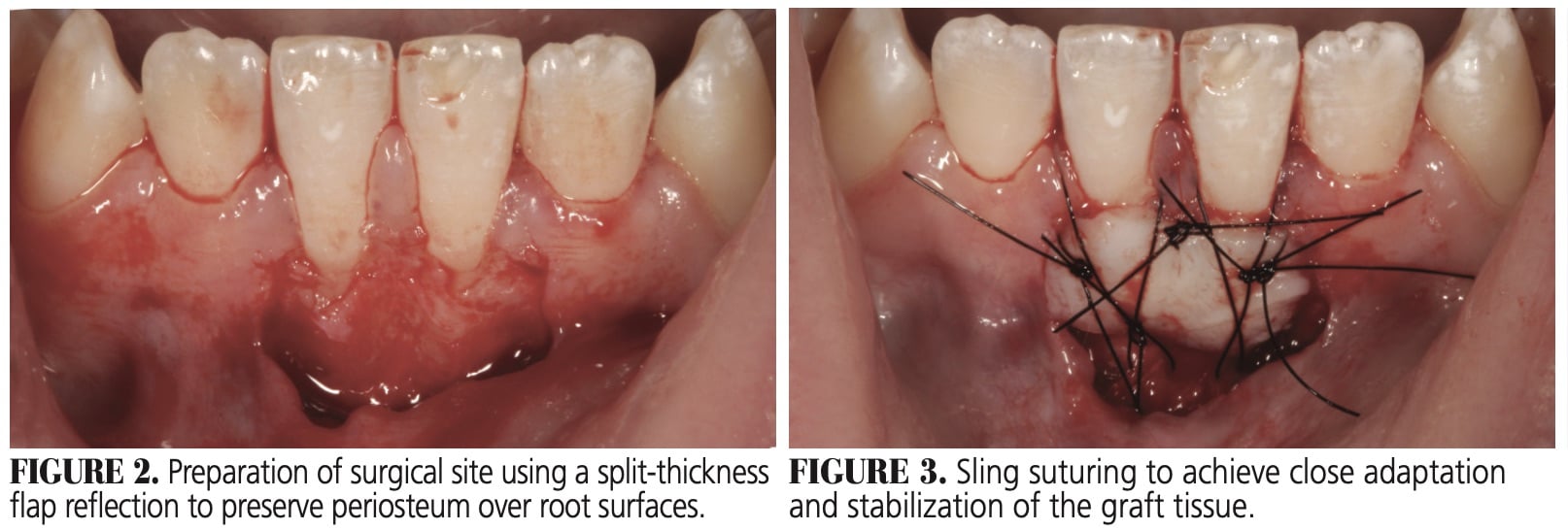
Figure 1 illustrates the thin periodontal phenotype overlying teeth #24 and 25. Figure 2 shows the prepared recipient site, achieved by a split-thickness incision, allowing for periosteum retention over the root surfaces. Sling sutures were used to hold and compress a graft (≈ 1.5 mm thickness) against the recipient bed (Figure 3). Note that even at this point the graft tissue exhibits a pale color due to loss of blood supply.
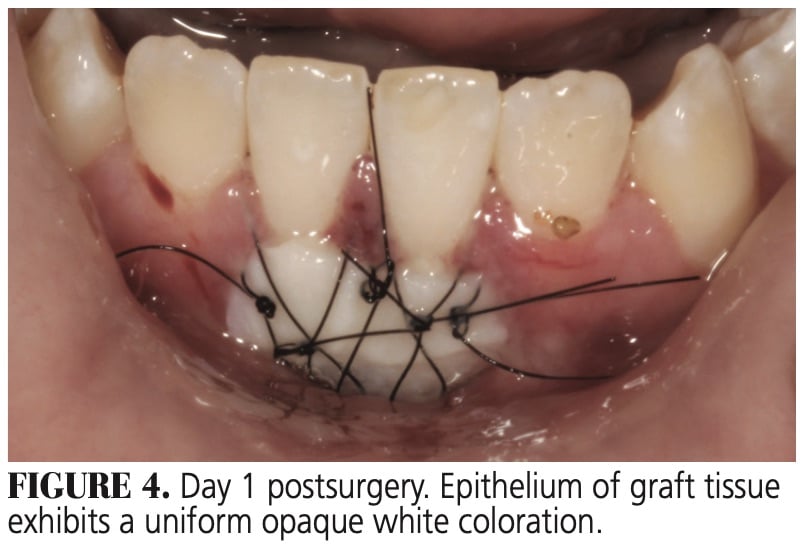 On day 1 post-graft placement, host tissues will exhibit a deep red color (Figure 4), indicating the vascular phase of the inflammatory reaction, with hyperemia and slight stagnation of blood flow into and out of the surgical site. The lateral graft margins will appear sealed to adjacent host tissues by a fibrin mesh (Figure 4). Such an adaptation will persist throughout the subsequent healing stages. Studies examining graft healing agree that initially the graft is separated from the recipient bed by a layer of fibrin exudate and, for at least two days postsurgery, graft viability is maintained by plasmatic circulation.14–17 During this period, all epithelial strata (except the stratum basale) become necrotic, exhibit an opaque cream color, and begin to desquamate.
On day 1 post-graft placement, host tissues will exhibit a deep red color (Figure 4), indicating the vascular phase of the inflammatory reaction, with hyperemia and slight stagnation of blood flow into and out of the surgical site. The lateral graft margins will appear sealed to adjacent host tissues by a fibrin mesh (Figure 4). Such an adaptation will persist throughout the subsequent healing stages. Studies examining graft healing agree that initially the graft is separated from the recipient bed by a layer of fibrin exudate and, for at least two days postsurgery, graft viability is maintained by plasmatic circulation.14–17 During this period, all epithelial strata (except the stratum basale) become necrotic, exhibit an opaque cream color, and begin to desquamate.
During days 3 through 6 postsurgery (Figure 5 and Figure 6), there will be little change in clinical appearance. The graft is characterized by a slight degree of edema and a surface layer of opaque desquamating epithelium, with subjacent reddish areas representing subepithelial vascular proliferation.A comparison of the images for days 1 through 6 shows a gradual reduction in epithelial opacity, indicating various degrees of epithelium desquamation. The surrounding host tissues exhibit a progressive decrease in the inflammatory response. At day 3 (Figure 5), the oral mucosa at the inferior border will be slightly inverted and not sealed to the graft tissue, which is typical of healing by secondary intention. Also, on days 3 through 6 (Figure 5 and Figure 6), any graft tissue overlying enamel may exhibit a yellow-cream color and appear necrotic.
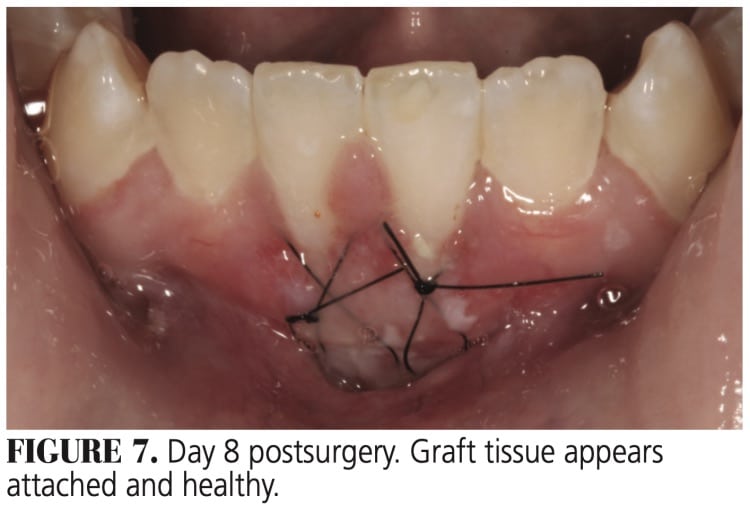
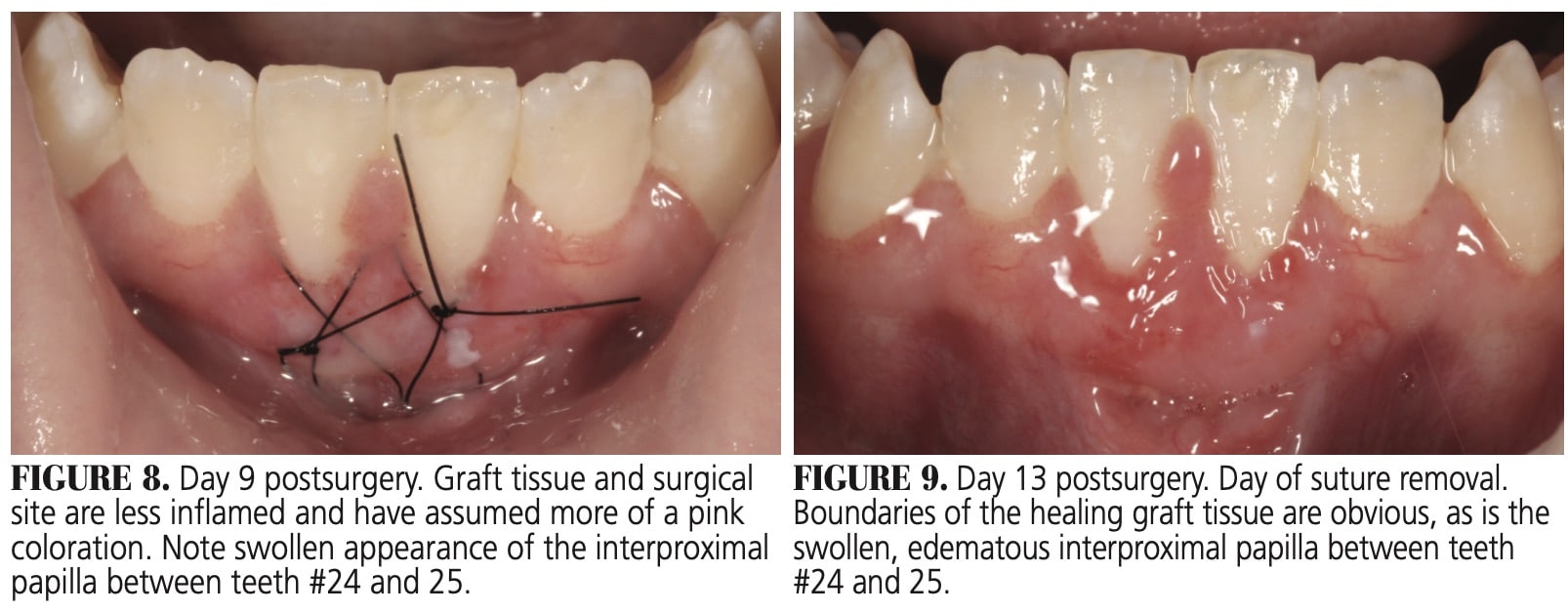
At days 7 through 9 postsurgery (Figure 7), the margins of the graft are merging with adjacent recipient tissues — except for the inferior border, which will still be healing by secondary intention. At days 7 and 8, the graft color will be a mixture of red-pink and white opaque areas. The opaque surface will mostly disappear by day 9 (Figure 8), indicating an intact layer of regenerated epithelium.
 By day 8 (Figure 7) the graft is clearly flattened, edema will have subsided and, except for the inferior border, the graft and host tissues will be contiguous. During days 10 through 13, inflammation will continue to decrease. However, islands of persistent inflammation involving the marginal gingivae may continue up to day 21. By day 13, graft and host tissues at the inferior border will be fused. In this case, the inflamed and hyperplastic interdental papilla between teeth #24 and 25 was removed via gingivoplasty (Figure 9).
By day 8 (Figure 7) the graft is clearly flattened, edema will have subsided and, except for the inferior border, the graft and host tissues will be contiguous. During days 10 through 13, inflammation will continue to decrease. However, islands of persistent inflammation involving the marginal gingivae may continue up to day 21. By day 13, graft and host tissues at the inferior border will be fused. In this case, the inflamed and hyperplastic interdental papilla between teeth #24 and 25 was removed via gingivoplasty (Figure 9).
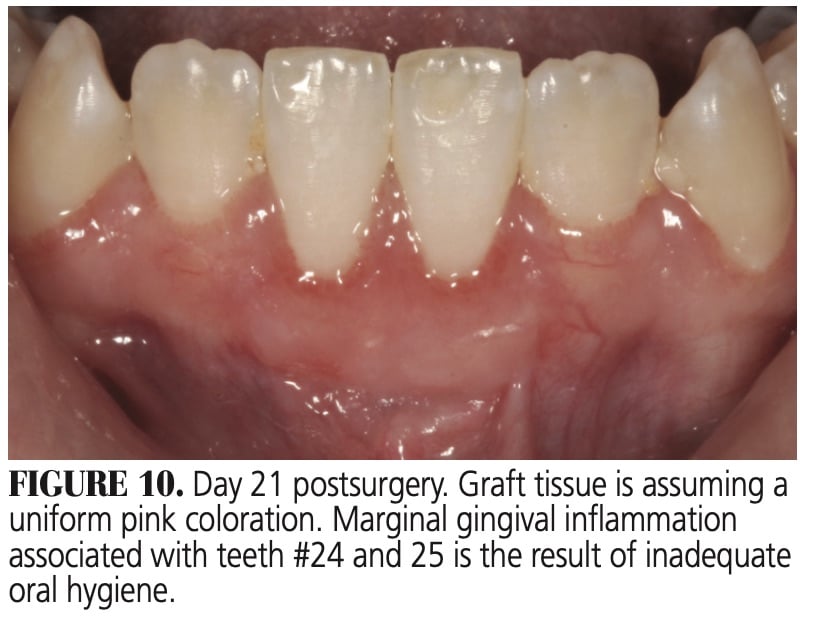
During days 21 through 90 (Figure 10 and Figure 11), the graft will make a transition from reddish-pink to a white-pink color, indicating complete regeneration of the keratinized epithelium. The persistent gingival margin inflammation seen in this case was likely the result of inadequate oral hygiene (Figure 10).
DISCUSSION
The first 48 hours postsurgery are critical to free gingival graft survival. During this time, there is no histologic evidence of vascularization of the graft. It is generally accepted that an exudate consisting of plasma, erythrocytes and white blood cells infiltrates the interface between the graft and periosteum to establish plasmatic circulation.12,13,16 During this period, the graft shows signs of epithelial disruption and desquamation, characterized by a change in color from pink to an opaque white and a edematous surface texture (Figure 4 and Figure 5). At this point, a clinician not familiar with the healing of a free gingival graft might mistake this presentation as a dead and/or failed graft. In addition, patients will frequently complain of a bad smell and indicate their graft is “dead.”
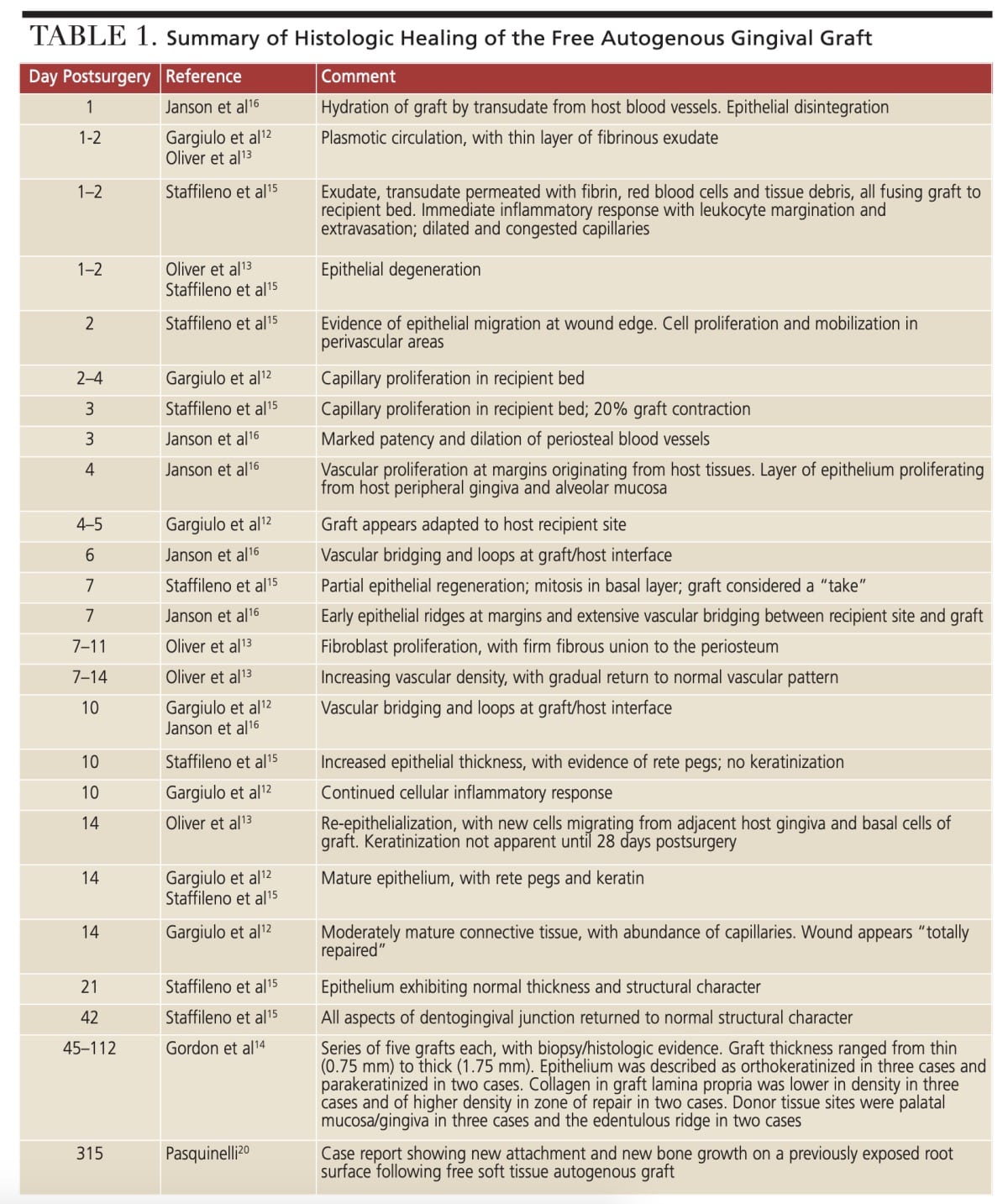
Because plasmatic circulation is important to graft survival, pooling of blood — sufficient to form a clot at the interface between host and graft tissues — will be detrimental to success. In this regard, Sullivan and Atkins17 noted that to prevent pooling of blood, the recipient site should be as smooth as possible. The earliest change in blood supply was reported by Gargiulo et al12 and Staffileno et al,15 with both groups noting the initial stages of capillary proliferation at 2 to 4 days. Various authors have reported the progressive changes in vascular development during days 3 to 14 postsurgery, including increased patency and dilation of periosteal vessels,16 significant vascular proliferation at the wound edge,16 capillary proliferation and budding in the recipient bed that eventually penetrates the overlying graft,15 vascular bridging and loops at the graft/host interface,12,16 and increasing vascular density up to seven days, followed by a gradual reduction and return to a normal vascular pattern after 14 days.13 During the first few days postsurgery, connective tissues in the graft lamina propria exhibit a loss of normal organization and collagenolysis.16 Multiple authors have reported increased fibroblast proliferation and establishment of a firm union of graft and underlying periosteum between days 7 through 14.12,13,15 Indeed, Garguilo et al12 characterized the histologic presentation at day 14 as “total repair.” Of interest in this respect is a report by Pasquinelli20 showing attachment of connective tissue and new bone growth on a previously exposed root surface at 315 days postplacement.
![]() CHANGES DURING HEALING
CHANGES DURING HEALING
The epithelium of a free gingival graft undergoes dramatic change while healing. Investigators have reported epithelial disintegration as early as 1 day postsurgery.13,15,16 In the present case, epithelial disintegration and desquamation were clinically evident from day 1 through day 8. Various authors have studied epithelial activity during the healing of a free gingival graft.12,13,15,16 Epithelial migration originating from peripheral gingiva and alveolar mucosa was observed at days 2 and 4 postsurgery,15,16 and by day 7 mitotic activity was noted in the stratum basale and suprajacent layers of the stratum spinosum.15 Of note, after seven days Staffileno et al15 considered the graft a “take.” By day 14, the epithelium achieves a normal histologic presentation.12,15 However, Oliver et al13 reported that epithelial maturation and keratinization was not clinically obvious until 28 days postsurgery. Total repair of the grafted site is reported at 14 days, and the epithelium achieves normal thickness and structural character at 21 days.12,13,15 This latter observation confirms the 21-day clinical presentation of the healed graft in the current case (Figure 10).
 Lastly, the issue of graft contraction during healing should be addressed. Staffileno et al15 reported a 20% decrease in graft size as early as three days postsurgery. According to Sullivan and Atkins,17 graft thickness determines behavior during healing, as well as its ultimate character. For example, in contrast to a thin graft (≈ 0.5 to 1.0 mm), a thick graft (≈ 1.25 to 1.75 mm) will immediately contract upon detachment from the donor site — this is termed primary contraction. Again, according to Sullivan and Atkins,17 a thick donor tissue procured from the palate generally contains some elastic connective tissue fibers and, when severed from the donor site, it may contract as much as 43%.
Lastly, the issue of graft contraction during healing should be addressed. Staffileno et al15 reported a 20% decrease in graft size as early as three days postsurgery. According to Sullivan and Atkins,17 graft thickness determines behavior during healing, as well as its ultimate character. For example, in contrast to a thin graft (≈ 0.5 to 1.0 mm), a thick graft (≈ 1.25 to 1.75 mm) will immediately contract upon detachment from the donor site — this is termed primary contraction. Again, according to Sullivan and Atkins,17 a thick donor tissue procured from the palate generally contains some elastic connective tissue fibers and, when severed from the donor site, it may contract as much as 43%.
Secondary contraction occurs during healing, a result of cicatrization. The effect of cicatrization depends on the thickness of the donor tissue lamina propria and rigidity of the recipient bed. Thus, a thick graft on a rigid bed offers optimal resistance to cicatrix contraction and will undergo minimal secondary contraction. In the case presented here, a comparison of measurements taken of the day 1 graft versus the day 90 healed graft indicates minimal contraction in the horizontal dimension (≈ 5%), but moderate contraction (≈ 23%) in the vertical dimension. A comparison of the graft in Figure 3 and Figure 12 shows ≈ 10% shrinkage in the coronal-apical dimension. Shrinkage was minimal in the horizontal dimension (mesial-distal). This result is similar to the 12% shrinkage in the horizontal dimension reported by de Resende et al.21 
CONCLUSION
The primary clinical traits that determine periodontal phenotype are gingival thickness, keratinized tissue width and bone morphotype. Collectively, these features are important in the maintenance of periodontal health.22
This report demonstrates the conversion of a thin periodontal phenotype to a thick phenotype using a free gingival graft. Documentation of day-to-day healing allows clinicians to differentiate normal healing from necrosis and graft failure. Further, the discussion of the histologic healing allows providers to correlate histologic features with the visual presentation.
The authors have no commercial conflicts of interest to disclose.
References
- Müller HP, Eger T. Gingival phenotypes in young male adults. J Clin Periodontol. 1997;24:65–71.
- Jepsen S, Caton JG, Jasim M, et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018;45(Suppl 20):S219–S229.
- Chambrone L, Tatakis DN. Long-term outcomes of untreated buccal gingival recessions: a systematic review and meta-analysis. J Periodontol. 2016;87:796–808.
- Kim DM, Neiva R. Periodontal soft tissue non-root coverage procedures: a systematic review from the AAP regeneration workshop. J Periodontol. 2015;86(Suppl 2):S56–S72.
- Kim DM, Bassir SH, Nguyen TT. Effect of gingival phenotype on the maintenance of periodontal health: an American Academy of Periodontology best evidence review. J Periodontol. 2020;91:311–338.
- Hwang D, Wang HL. Flap thickness as a predictor of root coverage: a systematic review. J Periodontol. 2006;77:1625–1634.
- Scheyer ET, Sanz M, Dibart S, et al. Periodontal soft tissue non-root coverage procedures: a consensus report from the AAP Regeneration Workshop. J Periodontol. 2015;86(Suppl 2):S73–S76.
- Zuhr O, Baumer D, Hurzeler M. The addition of soft tissue replacement grafts in plastic periodontal and implant surgery: critical elements in design and execution. J Clin Periodontol. 2014;41(Suppl 15):S123–S142.
- Sullivan HC, Atkins JH. Free autogenous gingival grafts. III. Utilization of grafts in the treatment of gingival recession. Periodontics. 1968;6:152–160.
- Mlinek A, Smukler H, Buchner A. The use of free gingival grafts for the coverage of denuded roots. J Periodontol. 1973;44:248–254.
- Dordick B, Coslet JG, Seibert JS. Clinical evaluation of free autogenous gingival grafts placed on alveolar bone. Part II. Coverage of nonpathologic dehiscence and fenestrations. J Periodontol. 1976;47:568–573.
- Gargiulo AW, Arrocha R. Histo-clinical evaluation of free gingival grafts. Periodontics. 1967;5:285–291.
- Oliver RC, Löe H, Karring T. Microscopic evaluation of the healing and revascularization of free gingival grafts. J Periodontal Res. 1968;3:84–95.
- Gordon HP, Sullivan HC, Atkins JH. Free autogenous gingival grafts. II. Supplemental findings — histology of the graft site. Periodontics. 1968;6;130–133.
- Staffileno H, Levy S. Histologic and clinical study of mucosal transplants in dogs. J Periodontol. 1969;40:311–319.
- Janson WA, Ruben MP, Kramer GM, Bloom AA, Turner H. Development of the blood supply to split-thickness free gingival autografts. J Periodontol. 1969;40:707–716.
- Sullivan HC, Atkins JH. Free autogenous gingival grafts. I. Principles of successful grafting. Periodontics. 1968;6:121–129.
- Mormann W, Schaer F, Firestone AR. The relationship between success of free gingival grafts and transplant thickness. Revascularization and shrinkage — a one year clinical study. J Periodontol 1981;52:74–80.
- Miller PD Jr. Root coverage with the free gingival graft. Factors associated with incomplete coverage. J Periodontol. 1987;58:674–681.
- Pasquinelli KL. The histology of new attachment utilizing a thick autogenous soft tissue graft in an area of deep recession: a case report. Int J Periodontics Restorative Dent. 1995;15:248–257.
- de Resende DR, Greghi SL, Siqueira AF, Benfatti CA, Damante CA, Zangrando MS. Acellular dermal matrix allograft versus free gingival graft: a histological evaluation and split-mouth randomized clinical trial. Clin Oral Investig. 2019;23:539–550.
- Eger T, Müller HP, Heinecke A. Ultrasonic determination of gingival thickness. Subject variation and influence of tooth type and clinical features. J Clin Periodontol. 1996;23:839–845.
- Matter J, Cimasoni G. Creeping attachment after free gingival grafts. J Periodontol. 1976;47:574–579.
From Decisions in Dentistry. October 2020;6(9):26-28, 31.

