
 OKAN AKDENIZ / ISTOCK / GETTY IMAGES PLUS
OKAN AKDENIZ / ISTOCK / GETTY IMAGES PLUS
Full-Mouth Restoration of a Heavy Smoker With Diabetes
This clinical report presents a comprehensive look at the full-mouth restoration of a patient with failing dentition complicated by Type 2 diabetes and chronic tobacco use.
PURCHASE COURSE
This course was published in the August 2022 issue and expires August 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the August 2022 issue and expires August 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe clinical considerations during patient selection for dental implant treatment.
- Explain the challenges to implant therapy for the patient in this case study.
- Discuss the fundamental treatment approach to this patient’s full-mouth rehabilitation.
Researchers studying blood flow at England’s Cambridge University in the early 1950s devised a method of constructing a titanium chamber that was embedded into the ears of rabbits. At the same time, Swedish orthopedic surgeon Branemark was investigating bone healing and regeneration, and he adopted the Cambridge model for use in the rabbit femur. But when he subsequently tried to retrieve the expensive titanium chambers, he discovered bone had grown in such close proximity to the titanium that it effectively adhered to the metal. Further research using both animal and human subjects confirmed this unique property of titanium.1 During this time frame, just four months after graduating from dental school, Linkow placed his first dental implant. As one of the pioneers in inserting titanium and other metal implants into the jawbone, Linkow is often referred to as the “father of implant dentistry.”1
The work of Branemark and Linkow led to an exciting new field in dentistry, implantology. This therapeutic approach provided practitioners with many new modalities to restore patients to an acceptable functioning dentition. Over the years, many implant shapes and materials have been developed. Root form implants have become the standard of care in implant dentistry, and modern implants are usually made of titanium alloy or ceramic. Currently, an implant survival rate of 95% for five years is considered a successful outcome.
During patient selection for implant therapy, clinicians must be aware of medical conditions, the state of oral hard and soft tissues, and any oral habits that may directly affect the long-term outcome of implant placement. General health and patient-related oral factors, such as bone quality, quantity and anatomical location, must be considered. Oral habits such as bruxism, for example, can play a significant role in implant failure.2 In addition, smoking, diabetes, hypertension and cardiovascular disease can affect dental implant outcomes over time.3
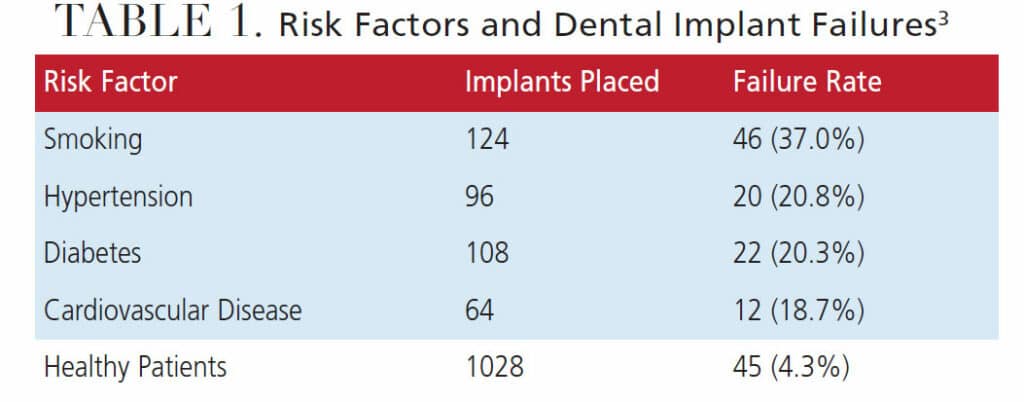
As illustrated in Table 1, in 2020, Singh et al3 reported revealing statistics in a university study conducted on 1420 implants placed in 826 patients. Healthy subjects in this study had a 95.7% success rate; this stands in contrast to patients who smoked, who had a 63.0% success rate. Therefore, when reviewing the health history of a patient, dentists must be keenly aware of potential negative issues — whether they are medical conditions, personal behaviors, oral conditions, or any combination thereof. In this litigious era, it is extremely important that practitioners clearly understand and are able and willing to convey the spectrum of possible complications and their frequency to their patients.4 This discussion must include all facets of the proposed treatment plan, in combination with the patient’s desires.
This paper will look at some of the greatest risk factors for poor outcomes (Table 1) in light of implant therapy for a patient who presented with Type 2 diabetes and a chronic smoking habit — two of the most significant causes of implant failure.

Cigarette smoking continues to be the No. 1 factor in patient-related implant failure. As reported by Kasat and Ladda4 in 2012, cigarette smoking has a deleterious influence on general health, as well as oral health. Smoking tobacco negatively affects the outcome of almost all therapeutic procedures performed in the oral cavity. For example, the failure rate of implant osseointegration is considerably higher among smokers than nonsmokers. Additionally, oral hygiene and maintenance around implants are adversely affected by smoking, which increases the risk of peri-implant disease.4

ADVERSE EFFECTS OF SMOKING AND DIABETES
The deleterious effects of cigarette smoking on wound healing after tooth extraction and its association with poor quality of bone are well documented. Cigarette smoke contains nicotine that delays bone healing and increases the rate of infections at the implant insertion site.5 In a study by Nazeer et al5 in 2020, it was reported that crestal bone loss around dental implants was significantly greater in smokers compared to nonsmokers, irrespective of the duration of loading. They also reported that, overall, smoking reduces dental implant success rates and increases marginal bone loss.5 In addition, smoking’s ill effects on the alveolar bone surrounding dental implants include reduced bone height, delayed healing, poor peri-implant bone formation, increased bone loss and peri-implantitis.6
Type 2 diabetes mellitus is a complex endocrine disorder characterized by chronic hyperglycemia that results in lack of glucose uptake by cells due to the impaired action of insulin.6 This is an extremely important disease from the standpoint of dental implant therapy. It is well known that a chronic hyperglycemic state impairs periodontal structure and function which, in turn, may directly impact the integrity of the periodontium and dental implant therapy. This is particularly true for patients whose diabetes is poorly controlled, whereas patients whose disease is well controlled experience few complications.7 However, it seems that poor glycemic status is the most important factor affecting implant complication rates in patients with Type 2 diabetes.8,9
CASE REPORT
A 51-year-old male presented for an initial dental examination and consultation in April 2021. At that time, a complete medical and dental history was obtained that indicated he had two significant issues that could influence the eventual treatment plan: Type 2 diabetes mellitus and a habit of smoking two packs of cigarettes per day. The patient’s chief complaint was that after going to several dentists, no one would treat him unless he agreed to full mouth extractions and complete dentures. He also reported he could not eat because “all of his teeth move” during mastication; in addition, he said his “mouth smells” and he is embarrassed to smile. It was obvious just sitting across from him that he previously had extensive dental work with what appeared to be full coverage on all visible teeth. In addition, when he closed his teeth together, the maxillary teeth intruded, indicating no bone support. After reviewing his concerns and explaining the risks with any treatment due to his medical history, the patient agreed to have radiographs taken so a diagnosis and treatment plan could be developed. Along with a panoramic radiograph, a cone beam computed tomography scan and photographs were taken.

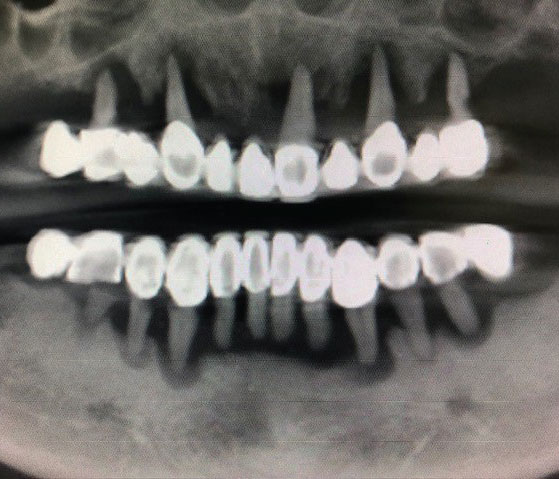
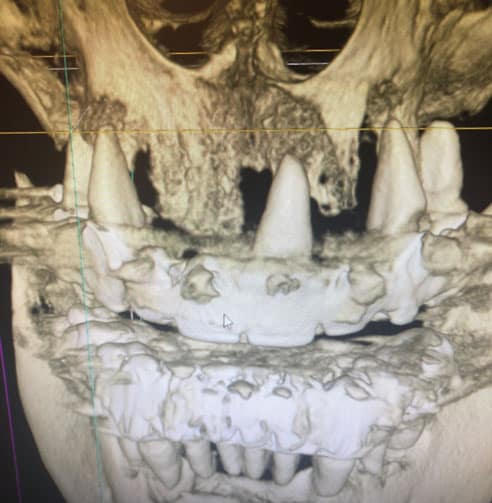
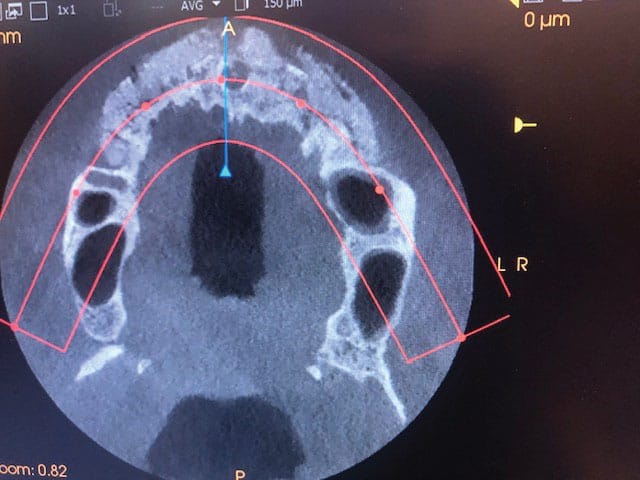
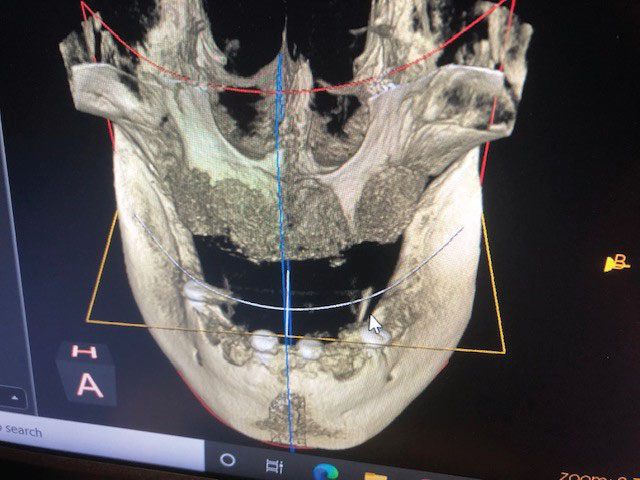
Clinical examination revealed that all of the patient’s dentition was frankly mobile and exhibited gross loss of periodontal tissue and underlying bone support. All areas of exposed tooth structure were covered with plaque and calculus (Figure 1 and Figure 2). In some areas, the roots were fully exposed. The panoramic radiograph revealed that except for two areas of minimal bone in the mandible, all the remaining teeth were totally tissue borne (Figure 3). Examination of the cone beam computed tomography scan confirmed that all maxillary and most of the mandibular teeth were positioned outside of any remaining bone (Figure 4 and Figure 5). Likewise, examination of the three-dimensional volumetric rendering confirmed the lack of any substantial bone or tooth support (Figure 6). It was easy at this point to understand why the patient was having trouble finding anyone to restore his mouth unless he would accept full dentures, which he did not want.

Even though the patient presented with two underlying issues that could totally destroy any attempt to restore his mouth with anything except removable full dentures, an additional treatment plan was developed. It would incorporate substantial bone grafting and implants to eventually provide a stable solution to his severely compromised oral presentation. The treatment plan included extraction of his 15 remaining teeth, along with bone augmentation in the maxillary tooth #4 to 11 and mandibular #20 to 29 areas. After healing and adequate integration of the grafting material, the placement of four maxillary and four mandibular implants could restore form and function.
In addition, the patient would need to understand the importance of quitting smoking, diligently monitoring his glucose level, and continuing his prescribed metformin, which he stated has kept his A1c level between 5 and 6. Any deviation in these areas would result in the discontinuation of treatment. The patient understood this and signed a statement agreeing to the treatment plan and smoking/medication restrictions. Following the recommendation of Bain10 and office protocol of Bergen,11 the patient was instructed to discontinue smoking at least two weeks prior to his next appointment and reminded he would need to maintain a smoke-free lifestyle for at least eight weeks post implant placement. He was scheduled for extraction of all of the remaining teeth, along with bone augmentation of both arches at the next appointment.
ESTABLISHING VERTICAL DIMENSION
Upon the patient’s return to start treatment, he confirmed he had not smoked since his initial visit and was taking his daily diabetes medication. There was no remaining nicotine stain on his tongue and no odor of cigarette smoke on his clothing, supporting his compliance to the agreed protocol. In addition, he reported his recent A1c level was 5.86. After placing wax over his existing loose teeth, impressions were taken of both arches in order to fabricate immediate full maxillary and mandibular dentures. Tooth color/selection was approved by the patient and the vertical dimension was established. He was reminded of the importance of maintaining his smoke-free lifestyle and dismissed.
For his next appointment, the patient was premedicated with 10 mg of diazepam at home and given another 10 mg dose chairside before starting treatment. Under local anesthesia, his maxillary teeth were easily removed, along with all granulation tissue. The tooth #4 to 11 area was grafted using 10 cc of allograft and covered with non-resorbable membrane. The soft tissue was approximated and sutured with interrupted non-resorbing polytetrafluoroethylene (PTFE) sutures, making sure the resulting maxillary ridge was free of any undercuts.

Next, the mandibular arch was addressed and, after local anesthesia, the 10 remaining mandibular teeth were extracted. Again, all granulation tissue was removed and the remaining native bone was evaluated. At this time, it was noted the residual bone could be used to create a platform to support the planned implants and graft material with adequate stability. Based on this chairside evaluation, a decision was made to place the four mandibular implants, along with the graft at this visit (Figure 7). A 6 cc volume of the same allograft material was placed along the residual ridge, and four implants were placed in the area of teeth #20 (3.7×10 mm), 24 (3.2×10 mm), 25 (3.2×10 mm) and 29 (3.7×10 mm). The grafted area was covered with collagen resorbable material. The soft tissue was approximated and sutured with interrupted PTFE non-resorbing sutures.
After irrigating the entire mouth and making sure all tissue was closed, the maxillary and mandibular immediate dentures were delivered and adjustments made to ensure the patient would be comfortable. Because this was an extensive surgical procedure, he was prescribed clindamycin and a methylprednisolone dose pack, along with 800 mg ibuprofen and 5/ⰽoxycodone/acetaminophen, as needed.
Three weeks later, the soft tissue was healing within normal limits, so all mandibular sutures were removed. The maxillary sutures over the non-resorbable membrane were not removed at this time. Several minor adjustments were made to the dentures and the patient was dismissed. He returned in another two weeks and the maxillary sutures were removed. The patient was then scheduled for the future placement of the maxillary implants.
CONCLUSION
Although many dentists might avoid a patient with the medical and dental history of the individual described in this case report, his desire for a stable outcome and willingness to deal with an acute smoking habit allowed the treatment plan to move forward.
A comparison of the patient’s initial presentation (Figure 3) with the outcome following extraction of all of his teeth and placement of freeze-dried bone demonstrates acceptable preservation and augmentation of the maxillary and mandibular ridges (Figure 7 through Figure 9).
Appearing in a future issue, the concluding installment of this two-part series will cover placement of the maxillary implants and permanent restoration of both arches.
REFERENCES
- Dental implant. Available at: https://en.wikipedia.org/wiki/Dental_implant. Accessed June 28, 2022.
- Chitumalla R, Kumari KV, Mohapatra A, Parikar AS, Anand KS, Katragadda Assessment of survival rate of dental implants in patients with bruxism: A 5-year retrospective study. Contemp Clin Dent. 2018;9(Suppl 2):S278–S282.
- Singh R, Parihar AS, Vaibhav V, Kumar K, Singh R, Jerry JJ. A 10 years retrospective study of assessment of prevalence and risk factors of dental implant failures. J Family Med Prim Care. 2020;9:1617–1619.
- Kasat V, Ladda R. Smoking and dental implants. J Int Prev Community Dent. 2012;2:38–41.
- Nazeer J, Singh R, Suri P, et al. Evaluation of marginal bone loss around dental implants in cigatette smokers and nonsmokers. A comparative study. J Family Med Prim Care. 2020;9:729–734.
- Kumar A, Nasreen S, Bandgar S, Bhowmick D, Vatsa R, Priyadarshni P. Comparative evaluation of marginal bone loss and implant failure rate in smokers and nonsmokers. J Pharm Bioallied Sci. 2021;13:203–206.
- Al Zahrani S, Al Mutairi A. Crestal bone loss around submerged and non-submerged dental implants in individuals with type-2 diabetes mellitus: A 7-year prospective clinical study. Med Princ Pract. 2019;28:75–81.
- Ghiraldini B, Conte A, Casarin RC, et al. Influence of glycemic control on peri-implant bone healing: 12-month outcomes of local release of bone-related factors and implant stabilization in type-2 diabetes. Clin Implant Dent Relat Res. 2016;18:801–809.
- Javed F, Romano GE. Impact of diabetes mellitus and glycemic control on the osseointegration of dental implants: a systemic literature review. J Perio. 2009;80:1719–1730.
- Bain CA. Smoking and implant failure — Benefits of a smoking cessation protocol. Int J Oral Maxillofac Implants. 1996;11:756–759.
- The Negative Effects of Smoking on Dental Implants. Available at: https://www.bergenoralsurgery.com/blog/the-
negative-effects-of-smoking-on-dental-implants/#:~:text=Here%20are%20a%20few%20alarming%20facts%
20about%20smoking,patient%20to%20receive%20dental%20implants.%20More%20items…%20. Accessed June 28, 2022.
From Decisions in Dentistry. August 2022;8(8)30-33.

