

Fresh Approach to Caries Arrest in Adults
Long used in other countries, silver diamine fluoride is now cleared for use in the U.S. While there is an assumption of use for pediatric caries control, here we explore indications for adults.
Long used in other countries, silver diamine fluoride is now cleared for use in the U.S. While there is an assumption of use for pediatric caries control, here we explore indications for adults.
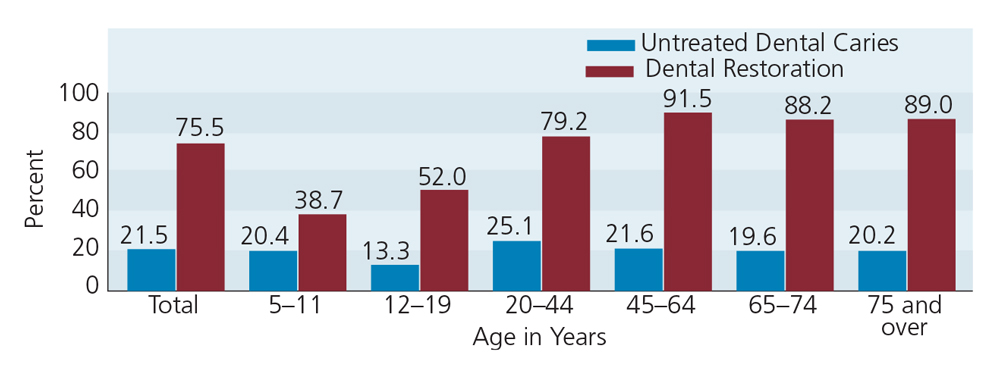
Although it may sound counterintuitive to some dental professionals, there is more untreated caries in adults than any other group. According to national data, the proportion of Americans age 20 and older with untreated tooth decay ranges from 20% to 25%, with younger adults experiencing more disease (Figure 1).1 Indeed, the problem of tooth decay is more severe in U.S. adults than children, yet it has received less attention. The adult population has grown and longevity has increased, while tooth loss has decreased overall — signaling that burden of adult caries is on the rise.2 Data show that 92% of the adult population has had at least one tooth restored, and decay in adults often occurs at the margins of these restorations.1
Root decay is an increasing concern with advancing age, but no current national data are available on its prevalence. That said, we know root surface decay tends to appear in the same population that has experienced coronal decay, and is exacerbated by periodontal attachment loss and the polypharmacy of older age.3 A report from the Northwest Practice-based Research Collaborative found that 20% of middle-aged-and-older adults have root caries.4 A systematic review of existing studies suggested the rate was 24% among older adults.5 Thus, the root surface decay problem is likely as great as that of coronal decay.
Silver diamine fluoride (38% weight per total volume (w/v) Ag(NH3)2F, 30% weight per total weight) is a colorless topical medicament comprising 25% to 29% (w/v) silver and 5% to 6% fluoride. This agent, which is pH 10,6 was only recently cleared for use in the U.S. The first product cleared by the U.S. Food and Drug Administration (FDA) became available in 2015 (Advantage Arrest, Elevate Oral Care, LLC). The silver acts as an antimicrobial, the fluoride promotes remineralization, and the ammonia stabilizes high concentrations in solution.7 Application simply involves drying the surface, then applying sparing amounts of the liquid to the tooth, with no special instructions for post-application care.
Like fluoride varnish, the FDA label indication is for treating dentinal hypersensitivity in adults. There’s another parallel to fluoride varnish, as silver diamine fluoride also shows promise for preventing and treating caries. As with other forms of off-label use, however, choosing silver diamine fluoride for this purpose falls under the purview of clinicians’ professional judgment.
In Japan, Australia, Argentina and other nations, dentists have been placing silver diamine fluoride on caries lesions for more than 80 years. The value of silver ions to treat tooth decay has been known in this country for well over a century. Silver nitrate was commonly used by the forefathers of modern dentistry (e.g., G.V. Black, Percy Howe, Basil Bibby and others). In the past 20 years, dental scientists have more rigorously assessed its efficacy and safety.
Differences in nomenclature have led to confusion around this material. In order to systematically review the evidence, a literature review was designed to search PubMed and the International Association of Dental Research abstract archive with the following terms: “33040-28-7” OR “1Z00ZK3E66“ OR “silver diamine fluoride” OR “silver fluoride” OR “silver diammine fluoride” OR “diammine silver fluoride” OR “ammonical silver fluoride” OR “ammoniacal silver fluoride.” We found nine published randomized clinical trials of at least one year in duration evaluating silver diamine fluoride for caries arrest and/or prevention. Two studies focused on caries in adults.
key takeaways
- Cleared by the U.S. Food and Drug Administration for treating dentinal hypersensitivity, in off-label use silver diamine fluoride can be used to prevent and arrest caries.
- The agent acts as an antimicrobial that remains active well after application. It also promotes remineralization and resistance to demineralization in enamel and dentin.
- In order to effectively implement treatment, clinicians should know the indications and contraindications, and gain informed consent for use.
- Dentists and (if allowed by state practice acts) dental auxiliaries who apply this agent must understand precautions for handling silver diamine fluoride.
- Repeat application completely stops many, but not all lesions. Research is needed to determine why some caries are not arrested.
PROMISING TECHNOLOGY
When applied every six months, silver diamine fluoride arrests more than 90% of caries.8,9 In children, applying silver diamine fluoride on active lesions once per year prevents caries in other teeth better than fluoride varnish placed four times per year on all surfaces.10 The same has been shown for direct prevention on noncarious surfaces.11 Six large, randomized clinical trials demonstrated better caries prevention than other noninvasive materials, and six demonstrated better caries arrest than other noninvasive materials (three studies overlap in evaluating both prevention and arrest).12 Silver diamine fluoride has shown similar performance in arresting caries as does the atraumatic restorative technique.9,12,13
Many dentists have long held that, as a disease, dental caries must be “under control” in order for restorative efforts to succeed. This concept was updated by one of the authors with the postulation that caries arises when pathological factors (e.g., fermentable carbohydrates and oral bacteria, such as mutans streptococci and Lactobacilli) outweigh protective factors (e.g., salivary flow, fluoride and antibacterial therapy).14,15 The concept was formalized into Caries Management by Risk Assessment (CAMBRA) and has been shown to be an effective approach.16
The implication is that reducing pathological factors and increasing protective factors reinstates a balance in favor of caries control, and provides an environment in which restorative care can be successful. In particular, fluoride alone is insufficient to swing the caries balance to the “no caries” side unless an antibacterial agent is added to the therapeutic mix. Silver diamine fluoride facilitates both goals in the CAMBRA strategy, wherein the silver decreases pathological bacteria and the fluoride promotes protective remineralization. Further, the low cost and profound ease of application enables widespread rapid adoption.
METHOD OF ACTION
Dental caries is a complex disease in which bacterial products cause demineralization and organic degradation. Once dentin is demineralized, the organic collagen matrix is exposed. Bacterial and host enzymes break down the organic components, and lesions advance.17
Without any excavation of soft dentin, silver diamine fluoride reacts with dentin protein and lays down a layer of silver protein that is resistant to bacterial acids and promotes the formation of hydroxyapatite and fluorapatite. The silver kills the bacteria,18 and treated surfaces are less susceptible to biofilm formation.19 The decayed surface increases in mineral composition and hardness and the lesion gets smaller.20 Figures 2A and 2B show microscopy images of a dentin surface degraded by demineralization compared to a surface treated with silver diamine fluoride.
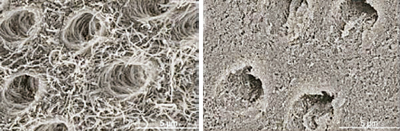
Courtesy of Ch Chu, University of Hong Kong
When used for treating hypersensitive dentin, topical application partially plugs dentinal tubules.20 The resulting decrease in sensitivity among treated patients21,22 is consistent with the hydrodynamic theory of dentinal hypersensitivity.23 In adults, sensitive teeth that are treated several times over a few weeks will show less response to an air blast and should be less sensitive to hot or cold stimuli.21 Comparing a range of studies, silver diamine fluoride appears more likely to decrease tooth sensitivity than fluoride varnish, desensitizers or oxalates.
For adult patients, the primary indications for topical treatment with silver diamine fluoride are:
- Treating dentinal hypersensitivity
- Caries stabilization in a new patient whose disease is uncontrolled, and is therefore at high risk of experiencing new lesions (Figure 3)
- Patients with extreme caries risk — for example, patients experiencing xerostomia from cancer treatment or taking multiple hyposalivatory medications (Figure 4)
- Treating vulnerable surfaces, such as roots exposed from periodontal attachment loss, overdenture and partial denture abutments, or partially exposed third molars
- Difficult-to-treat caries lesions (e.g., furcations or at the margins of fixed bridges)
- Adults who cannot cooperate because of cognitive disabilities (e.g., patients with autism or dementia)
- Patients without access to restorative dental services
In these patients, silver diamine fluoride is not merely a substitute for fluoride varnish; it is an effective first-stage treatment.
EFFICACY IN ADULTS
Clinical research on silver diamine fluoride began in earnest in the late 1990s and its initial focus centered on early childhood caries. Randomized, double-blind, controlled clinical trials demonstrate that when treated every six months with silver diamine fluoride, even deep lesions in primary teeth are arrested in more than 90% of cases, with no damage to the pulp or abscess formation.7 Follow-up studies in both the primary and permanent dentition also demonstrate efficacy and safety. The effectiveness of this agent has been demonstrated in treating root caries,11,24 and in its use as an indirect pulp cap.25 Studies also show the value of employing silver diamine fluoride in conjunction with addressing other protective factors (particularly oral health education),24 and case reports have added to the evidence.26
As part of the University of California, San Francisco School of Dentistry paradigm shift committee, we recently formalized best practices for use of silver diamine fluoride based on evidence and clinical experience.12 When a caries risk assessment determines that an adult patient would benefit from treatment with silver diamine fluoride, food debris is rinsed away, individual caries lesions are isolated with cotton rolls, each lesion is dried, and one drop of the agent is applied with a microsponge. Care is taken to use the minimum amount needed to treat the lesion, and not apply the agent to the surrounding gingival tissue.
Note that no mechanical excavation is performed. The material is allowed to take effect for 1 to 3 minutes, and then the area is lavaged using water and high-volume suction. Lesions will harden and then turn dark brown or black within a week as the caries arrests (similar in appearance to naturally arrested lesions). A curing light can accelerate the color change, allowing evaluation of whether the lesion is adequately treated. The agent only discolors infected and affected dentin, and will not stain intact tooth structure. Patients should be advised they are likely to experience a momentary metallic taste, which resolves by itself. Prior to treatment, they should also be informed about the permanent color change, and for this reason it is advisable to secure informed consent.
Lesions should be retreated at regular recall intervals (at least twice per year), until they are restored. Difficult-to-treat lesions — in furcations, for example, or in situations in which restorative dentistry isn’t feasible — can be maintained with this treatment. An example of the latter might include a patient with financial issues that delay definitive treatment.
In adults, untreated caries serve as an environmental niche that promotes growth of cariogenic microorganisms that can spread to cause new lesions. Treating caries with silver diamine fluoride kills the bacteria, thus reducing the potential for the lesion to advance or the bacteria to seed to surrounding dentition. Meanwhile, treated lesions serve as a reservoir of silver, which is reactivated once the bacteria attempt to recolonize. The treated lesion also acts as a reservoir for fluoride, which promotes mineralization and resistance to acid attack. In this sense, treated lesions help to maintain a therapeutic level of fluoride to reverse the effects of acidification following carbohydrate ingestion.
PRECAUTIONS AND SAFETY
Silver allergy is a contraindication. It is noted that nickel allergy is commonly misreported as a silver allergy, and consultation with the patient’s physician may be relevant if the health history suggests a possible allergy. Relative contraindications include any significant desquamative gingivitis or mucositis that disrupts the protective barrier formed by gingiva or mucosa. Increased absorption and pain would be expected with contact. Heightened caution and use of a thin layer of petroleum jelly is recommended.
PROCEDURE BILLING CODE
The Code on Dental Procedures and Nomenclature (CDT) Code Maintenance Commission approved Code 1354 for “interim caries arresting medication application” for 2016. The code definition is: “Conservative treatment of an active, nonsymptomatic carious lesion by topical application of a caries arresting or inhibiting medicament and without mechanical removal of sound tooth structure.” The CDT code is the Health Insurance Portability and Accountability Act standard code set and is required for billing. Insurers are in the process of evaluating coverage for this treatment.
TREATMENT PLANNING
Phased treatment planning is recommended with high-risk caries patients, with the first goals being to arrest active decay and stabilize the caries balance. Often, patients with multiple caries lesions face long and complicated restorative treatment. While awaiting completion of care, new lesions may form and existing lesions may advance, thus further expanding the scope of treatment. In these situations, silver diamine fluoride can help arrest caries prior to comprehensive rehabilitation (Figure 3).

In today’s economic environment, patients often face insurance benefit limitations and out-of-pocket costs that further prolong treatment. Others who have minimal dental benefits or lack insurance need a treatment to hold them until they can afford restorative care. This modality holds promise to address this need.
Lesions treated with silver diamine fluoride can be restored with any dental material (e.g., amalgam, resin, glass ionomer or cast restorations) to address plaque traps, esthetic concerns or occlusal function. Glass ionomer cement (GIC) is directly compatible without excavation, but placement of resin-based composites should follow enamel surface preparation with a bur to maximize bond strength. The dark color change brought on by silver diamine fluoride can show through semitransparent materials, including natural enamel. This can be masked using an opaque composite base or with a sandwich restoration of GIC and composite. It may be preferable to mechanically remove the discolored material, particularly along the dentin-enamel junction. Surprisingly, it is often reported that discolored dentin can be removed without anesthetic.
Special attention should be paid to anticipate recurrent caries at the margins of fixed bridges, partial denture abutments and overdenture abutments. When lesions occur in these areas, treatment with silver diamine fluoride may prove sufficient until more definitive treatment is feasible.
CONCLUSION
Patients with periodontal disease and others who have experienced attachment loss may report sensitivity and be at risk for root surface caries. Careful attention to the caries balance is required with these patients, and the clinical approach to sensitive surfaces and softened dentin is the same as for caries.
Considering this is a fluoride product, dental hygienists and dental assistants may be allowed to apply silver diamine fluoride. When used appropriately, silver diamine fluoride will not stain sound enamel or dentin. Superficial discoloration of adjacent fillings has been observed for some composites, and can be removed with prophy paste. Staining of leaking composite margins is likely and may warrant replacement.

For clinicians who treat cognitively or physically challenged adults, silver diamine fluoride may rapidly become a regular part of the armamentarium. Even in cases in which dental care under general anesthesia or heavy sedation is financially and medically appropriate, this modality can arrest and stabilize caries and reduce the burden on caregivers. For example, Figure 4 shows a cancer patient whose medical treatment greatly increased his caries risk. Silver diamine fluoride was used to restore caries balance for several years while his medical condition presented barriers to definitive restorative treatment. From a public health point of view, clinicians may find this to be an effective agent for treating patient populations that face barriers to care.
Silver diamine fluoride is a new evidence-based technology for U.S. dental practices. It is profoundly useful for managing caries in adult and pediatric populations, and is economically and practically feasible for use in outpatient settings as well as daily practice. Consistent with the CAMBRA principle, it appears to be particularly effective in stabilizing patients for whom caries control is challenging. Indications for this new tool include treating caries in extremely high-risk patients and surfaces, patients who are cognitively or physically challenged, and lesions that are difficult to restore.
References
- Dye BA, Li X, Beltrán-Aguilar ED. Select oral health indicators in the United States, 2005–2008. NCHS Data Brief. 2012;96:1–8.
- Dye BA, Thornton-Evans G. Trends in oral health by poverty status as measured by Healthy People 2010 objectives. Public Health Rep. 2010;125:817–830.
- Beck JD, Drake CW. Do root lesions tend to develop in the same people who develop coronal lesions? J Public Health Dent. 1997;57(2):82–88.
- Chi DL, Berg JH, Kim AS, Scott J. Correlates of root caries experience in middle-aged and older adults in the Northwest Practice-based REsearch Collaborative in Evidence-based DENTistry research network. J Am Dent Assoc. 2013;144:507–516.
- Griffin SO, Griffin PM, Swann JL, Zlobin N. Estimating rates of new root caries in older adults. J Dent Res. 2004;83:634–638.
- Mei ML, Chu CH, Lo ECM, Samaranayake LP. Fluoride and silver concentrations of silver diammine fluoride solutions for dental use. Int J Paediatr Dent. 2013;23(4):279–285.
- Rosenblatt A, Stamford TCM, Niederman R. Silver diamine fluoride: a caries “silver-fluoride bullet.” J Dent Res. 2009;88(2):116–125.
- Llodra JC, Rodriguez A, Ferrer B, Menardia V, Ramos T, Morato M. Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of schoolchildren: 36-month clinical trial. J Dent Res. 2005;84(8):721–724.
- Zhi QH, Lo ECM, Lin HC. Randomized clinical trial on effectiveness of silver diamine fluoride and glass ionomer in arresting dentine caries in preschool children. J Dent. 2012;40(11):962–967.
- Chu CH, Lo ECM, Lin HC. Effectiveness of silver diamine fluoride and sodium fluoride varnish in arresting dentin caries in Chinese pre-school children. J Dent Res. 2002;81(11):767–770.
- Tan HP, Lo ECM, Dyson JE, Luo Y, Corbet EF. A randomized trial on root caries prevention in elders. J Dent Res. 2010;89(10):1086–1090.
- Horst JA, Ellenikiotis H, UCSF Silver Caries Committee, Milgrom PM. The UCSF protocol for caries arrest using silver diamine fluoride: rationale and clinical application. J Calif Dent Assoc. in press.
- Santos dos VE Jr, Filho AV, Targino AGR, et al. A new “silver-bullet” to treat caries in children — nano silver fluoride: a randomised clinical trial. J Dent. 2014;42(8):945–951.
- Featherstone JDB. The caries balance: contribution factors and early detection. J Calif Dent Assoc. 2003;31:129–133.
- Featherstone JDB. The science and practice of caries prevention. J Am Dent Assoc. 2000;131:887–899.
- Cheng J, Chaffee BW, Cheng NF, Gansky SA, Featherstone JDB. Understanding treatment effect mechanisms of the CAMBRA randomized trial in reducing caries increment. J Dent Res. 2015;94:44–51.
- Featherstone JDB. The continuum of dental caries — evidence for a dynamic disease process. J Dent Res. 2004;83 Spec No C:C39–C42.
- Tanzer JM, Thompson A, Whitford G. Silver diamine fluoride, carious lesion arrest, and antimicrobial action. J Dent Res. in press.
- Knight GM, McIntyre JM, Craig GG, Mulyani, Zilm PS, Gully NJ. Inability to form a biofilm of Streptococcus mutans on silver fluoride- and potassium iodide-treated demineralized dentin. Quintessence Int. 2009;40(2):155–161.
- Mei ML, Ito L, Cao Y, Li QL, Lo ECM, Chu CH. Inhibitory effect of silver diamine fluoride on dentine demineralisation and collagen degradation. J Dent. 2013;41(9):809–817.
- Castillo JL, Rivera S, Aparicio T, et al. The short-term effects of diammine silver fluoride on tooth sensitivity: a randomized controlled trial. J Dent Res. 2011;90(2):203–208.
- Craig GG, Knight GM, McIntyre JM. Clinical evaluation of diamine silver fluoride/potassium iodide as a dentine desensitizing agent. A pilot study. Aust Dent J. 2012;57(3):308–311.
- Markowitz K, Pashley DH. Discovering new treatments for sensitive teeth: the long path from biology to therapy. J Oral Rehabil. 2008;35(4):300–315.
- Zhang W, McGrath C, Lo ECM, Li JY. Silver diamine fluoride and education to prevent and arrest root caries among community-dwelling elders. Caries Res. 2013;47(4):284–290.
- Shimizu A, Kawagoe M. A clinical study of effect of diamine silver fluoride on recurrent caries. J Osaka Univ Dent Sch. 1976;16:103–109.
- Milgrom P. Management of patients with active caries. J Calif Dent Assoc. 2014;42:449–453.
- Chu CH, Lo ECM. Promoting caries arrest in children with silver diamine fluoride: a review. Oral Health Prev Dent. 2008;6:315–321.

[…] Decisions in Dentistry, The New York […]
Dental caries is one of the most prevalent chronic oral diseases across the globe that can be both treated and prevented. Preventive management strategies can effectively arrest and even completely reverse the caries process. This article aimed to review the literature on different approaches explored towards arresting caries progression.