

Fixed Treatment Options for Single Incisor Replacement
An examination of three tooth replacement options for a single incisor.
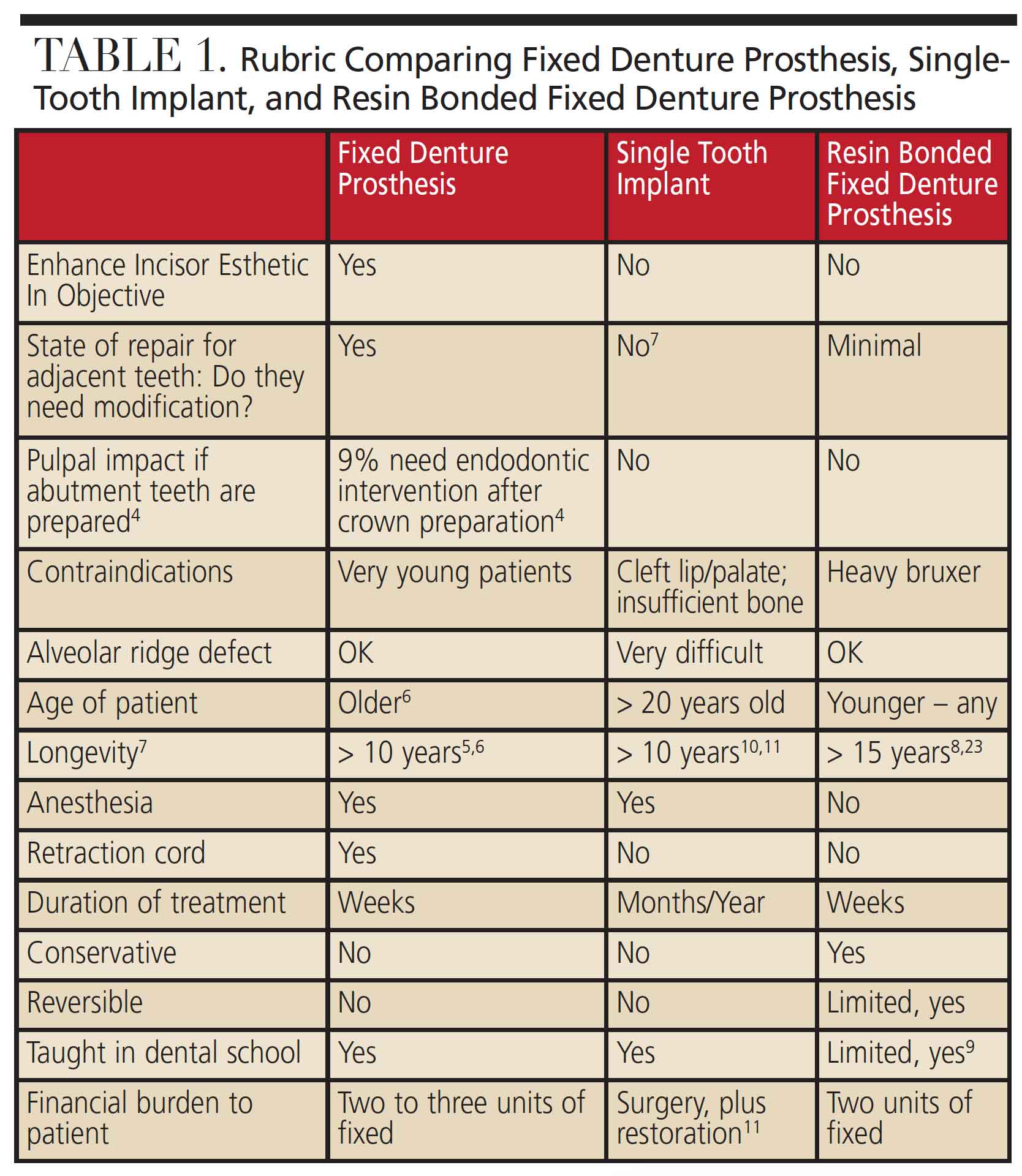
The replacement of a single incisor presents unique challenges in clinical practice. There are many fixed dental prosthesis options to restore esthetics and function. It is incumbent upon clinicians to diagnose and plan each case individually based on the patient’s needs. A rubric can be used to guide thoughtful consideration of clinical findings, radiographic information, the patient’s wishes, esthetic considerations, and best practice based on evidence. The three clinical cases presented in this paper are the source of the rubric found in Table 1, which presents different fixed tooth replacement options: a full coverage all-ceramic conventional fixed dental prosthesis (FDP), single-tooth implant (STI) restoration, and an all-ceramic cantilevered resin bonded fixed dental prosthesis (RBFDP).
A missing incisor is a challenge due to esthetics.1 If there is a need to Enhance Incisor Esthetics In Objective, smile analysis and design are indicated.2 Restoration of adjacent teeth may also be required. Among fixed restoration options, choosing between an FDP, STI or RBFDP will depend on multiple factors. Each option is listed in the rubric. The left column asks a question, and the answer will determine which option is logical and appropriate. The level of evidence for each option ranges from pragmatic observations by experienced clinicians to the highest level of evidence-based sources, such as Cochrane.3–16
PATIENT 1: FIXED DENTAL PROSTHESIS
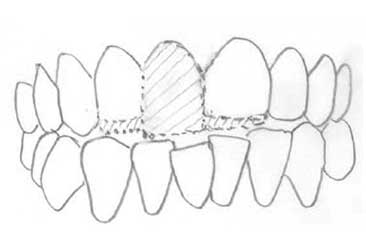
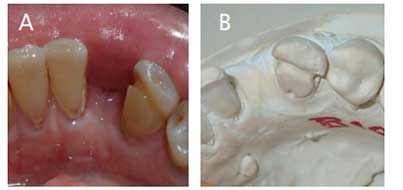
A 24-year-old male presented to the dental clinic at the University of the Pacific asking to change the gold crown on his front tooth. The patient’s medical history was noncontributory. A comprehensive exam with radiographs revealed an anterior open bite. A mesiodens in position #8 (Figure 1) had a gold crown with an open margin and overhang (Figure 2).
For correction of open bite in adults, a combination of orthodontics, surgery and speech therapy is necessary.12,13 The patient declined orthodontics and wished to proceed with restorative treatment to eliminate the gold restoration and improve his smile. Due to a poor crown-to-root ratio, extraction of the mesiodens was recommended. The options of an STI, FDP or RBFDP were considered. Several pencil sketches were drawn to compare the three restorative options (Figure 3, Figure 4 and Figure 5). An FDP would allow for shaping and contouring the abutment teeth to reduce the anterior open bite, which would not be possible with an STI or RBFDP.14 This decision confirms the findings for an FDP in the rubric.


bite and a gold crown on the mesiodens.

open bite without the mesiodens.

implant or resin bonded fixed denture
prosthesis: Either option will restore the
missing tooth, but not reduce the
patient’s open bite or address enhanced
incisor esthetics in objective.
prosthesis: The proposed morphologic
change in abutment teeth will reduce
the anterior open bite and enhance
incisor esthetics.

contoured to reduce anterior open bite.


modified ridge-lap pontic on tooth #8.
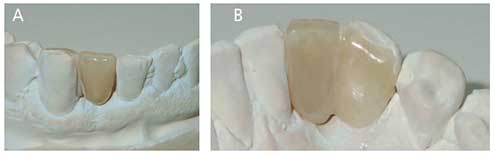
The patient chose a lithium disilicate (LD) FDP. This is a glass ceramic15 in the class of particle-filled glass materials, with high translucency and a lifelike appearance.16 A diagnostic wax-up of the anterior teeth was made, duplicated in dental stone, and then a putty matrix generated for the provisional restoration.
prosthesis restoration (B).
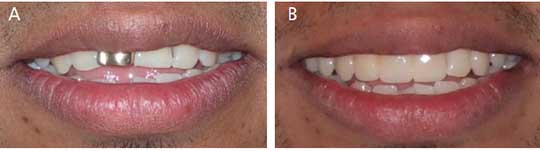
The abutment teeth #7 and 9 were prepared for monolithic LD-FDP abutment, guided by LD-specific recommendations for a 1.2-mm rounded shoulder margin and 15° to 20° taper for the axial walls. The margins were placed 0.5 mm subgingivally for esthetics. After abutment preparation, the mesiodens was extracted and an immediate provisional FDP was fabricated using bis-acryl resin shaped in a putty matrix. The morphology of the provisional restoration was in harmony with phonetics and esthetics (Figure 6), and the patient was pleased. An impression of the dental arch with the provisional was made to communicate morphology to the dental laboratory. After eight weeks of healing, an intraoral scan17 of dental arches and occlusion were captured and sent to the laboratory for LD-FDP fabrication (Figure 7). At the delivery appointment, the definitive restoration was tried intraorally and adjusted for proximal contacts, adaptation, margins, occlusion and esthetics. The open bite was reduced by 4 mm (Figure 8). Figures 9A and 9B show the improvement in esthetics.

fractured porcelain-fused-tometal crown, with endodontic sealer in the periapical region.

tooth structure with an
inadequate ferrule.

4.1×10-mm implant with a
conical healing abutment.

PATIENT 2: SINGLE-TOOTH IMPLANT-RETAINED CROWN
A 50-year-old female presented with the complaint, “My front tooth is moving.” She had an otherwise stable, moderately restored dentition. Her existing porcelain-fused-to-metal crown on tooth #8 and post were dislodged (Figure 10). She had pain on palpation and percussion. Tooth #8 was diagnosed as previously root canal treated, with symptomatic apical periodontitis. The remaining root-tooth structure was evaluated (Figure 11) and had less than 1 mm of supragingival dentin. Cone beam computed tomography (CBCT) was performed. The tooth could not be restored with a new crown, as the ferrule was inadequate.18 The prognosis in case of endodontic retreatment and orthodontic extrusion would be poor due to the crown-to-root ratio and conical shape of the root. Extraction was recommended, and three options were presented for fixed replacement. After discussing the risks and benefits of each option, the patient chose an STI, in line with the rubric.
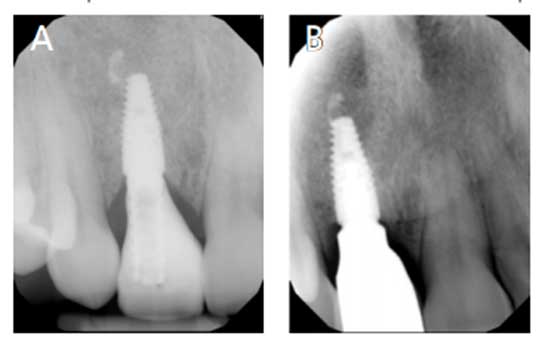
An alginate impression was made to fabricate a stayplate for tooth #8, as well as a surgical guide for implant placement. The presence of infection and excess sealer led to extraction of #8, curettage, and implant site preparation for alveolar ridge preservation. Deproteinized bovine bone mineral was placed for osteogenesis in the defect, with a collagenous membrane cover.19 After six months of healing, the site was reevaluated with CBCT, which showed adequate bone thickness and absence of infection.20 Guided surgery was performed to place a bone-level tapered implant, covered by a 4-mm conical titanium healing abutment (Figure 12) to shape the emergence profile.21

site #8.
Three months later, the healing abutment was replaced by a temporary abutment and provisional crown made of bis-acryl resin shaped in a press-formed splint. The cervical portion was contoured with flowable composite resin to develop the correct soft tissue emergence profile in harmony with adjacent teeth. After eight weeks, the desired gingival contour was obtained (Figures 13A and 13B). An implant impression was made using an open-tray impression coping. To accurately replicate the cervical contour of the implant-provisional restoration, a putty impression was made of the provisional implant crown extraorally. The diagnostic casts, shade selection and corresponding photos were sent to the laboratory. At the delivery appointment, the crown was tried and the occlusion was adjusted to allow passing of shim-stock foil during light contact. Protrusive and lateral excursions were adjusted in harmony with the rest of her dentition. The screw-retained implant prosthesis provided an esthetic outcome and healthy periodontal tissues (Figures 14A and 14B, and Figure 15).

defect and unrestored intact adjacent teeth (B).
PATIENT 3: ALL-CERAMIC CANTILEVER RESIN BONDED FIXED DENTAL PROSTHESIS
A 69-year-old male presented with a complaint that he had lost his front tooth. His medical history was noncontributory and his dentition was otherwise stable and minimally restored. He pointed to a missing mandibular lateral incisor (tooth #26) extracted because of a vertical root fracture (Figures 16A and 16B). The buccal plate had a fenestration associated with the root fracture. All three fixed tooth replacement options for tooth #26 were discussed with the patient. In this case, the difficulty with an STI approach included a bony defect, narrow space for implant osteotomy, and potential damage to adjacent teeth.22 A conventional FDP would involve the removal of sound tooth structure on unrestored, healthy abutment teeth. Long-term studies demonstrate excellent clinical outcome for the much more conservative treatment option of an RBFDP.8,23 The rubric concurred, and the patient elected an all-ceramic cantilevered RBFDP.
Non-precious etched metal RBFDP (Maryland bridges)24 were used previously, but their long-term service did not hold up as well as current designs using all-ceramic cantilevered with more defined abutment preparations.8,23–25 The preparation design has an uncanny resemblance to a classic three-quarter crown preparation for cast gold, with these notable details: the margin and finish lines are supragingival, and axial reduction is minimal. The exit angle for milled zirconia preparation should be close to 90°. The proximal boxes or grooves may expose a limited amount of dentin, but more than 90% of the prepared tooth is enamel, thus allowing enamel bonding. The prepared axial walls are kept parallel with addition of grooves near the terminal line angles for mechanical retention (Figures 17A and 17B). Because of the minimally invasive design of the preparation, anesthesia is not required, and the supragingival margin placement avoids the use of gingival retraction for impressions.
The prepared tooth is not sensitive and does not require a temporary restoration.26 A tray anterior sextant impression using an addition-reaction silicone impression material was used and the dental laboratory fabricated a zirconia ceramic three-quarter crown abutment with a porcelain layered pontic. The parallel grooves on the opposing walls provided mechanical retention (Figures 18A and 18B). The restoration was tried and adjusted. The intaglio surface of the abutment was air abraded to enhance resin bonding to zirconia. The abutment tooth was acid etched, rinsed, dried, and the RBFDP was bonded. This case demonstrates conservative and minimally invasive treatment with an RBFDP27 for partial edentulism (Figures 19A and 19B).

CONCLUSION
Patients 1, 2 and 3 each presented with unique dental concerns, and it is wise to listen to the patient and thoroughly examine the clinical findings to determine the best treatment option. The use of a rubric may be helpful in decision-making. The evolution of digital technology and introduction of new restorative materials have improved tooth replacement options, as demonstrated by these cases involving a single incisor.
For the esthetic zone, systematic treatment planning — combined with the careful choice of technique, materials and shade selection, along with good laboratory communication — will yield superior prosthetic results.
KEY TAKEAWAYS
- There are many fixed dental prosthesis options to restore esthetics and function when replacing a single incisor.
- Based on the patient’s needs, a rubric (Table 1) can be used to guide careful consideration of clinical findings, radiographic information, the patient’s wishes, esthetic considerations, and best practices.
- For restorations in the esthetic zone, systematic treatment planning — combined with a careful choice of technique, materials and shade selection, along with good laboratory communication — will yield superior prosthetic results.
REFERENCES
- Studer S, Pietrobon N, Wohlwend A. Maxillary anterior single-tooth replacement: comparison of three treatment modalities. Prac Periodontics Aesthet Dent. 1994;6:51–62.
- Tjan AH, Miller GD. The JG. Some esthetic factors in a smile. J Prosthet Dent. 1984;51:24–28.
- Fugazzotto PA. Evidence-based decision making: replacement of the single missing tooth. Dent Clin North Am. 2009;53:97–129.
- Kontakiotis EG, Filippatos CG, Stefopoulos S, Tzanetakis GN. A prospective study of the incidence of asymptomatic pulp necrosis following crown preparation. Int Endod J. 2015;48:512–517.
- Kassardjian V, Varma S, Andiappan M, Creugers NH, Bartlett D. A systematic review and meta analysis of the longevity of anterior and posterior all-ceramic crowns. J Dent. 2016;55:1–6.
- Ioannidis G, Paschalidis TH, Petridis HP, Anastassiadou V. The influence of age on tooth supported fixed prosthetic restoration longevity. A systematic review. J Dent. 2010;38:173–181.
- Salinas TJ, Eckert SE. In patients requiring single-tooth replacement, what are the outcomes of implant — as compared to tooth-supported restorations? Int J Oral Maxillofac Implants. 2007;22 (Suppl):71–95.
- Kern M. Fifteen-year survival of anterior all-ceramic cantilever resin-bonded fixed dental prostheses. J Dent. 2017;56:133–135.
- 9. Virdee SS, Lynch CD, Sadaghiani L, et al. Contemporary teaching of bridges (fixed partial dentures) in Ireland and United Kingdom dental schools. Br Dent J. 2018;224:741–745.
- Loza-Herrero MA, Rivas-Tumanyan S, Morou-Bermudez E. Success and complications of implant-retained prostheses provided by the Post-Doctoral Prosthodontics Program, University of Puerto Rico: a cross-sectional study. J Prosthet Dent. 2015;114:637–643.
- Scheuber S, Hicklin S, Brägger U. Implants versus short-span fixed bridges: survival, complications, patients’ benefits. A systematic review on economic aspects. Clin Oral Implants Res. 2012;23(Suppl 6):50–62.
- Tavares CA, Allgayer S. Open bite in adult patients. Dental Press J Orthod. 2019;24:69–78.
- Teittinen M, Tuovinen V, Tammela L, Schätzle M, Peltomäki T. Long-term stability of anterior open bite closure corrected by surgical-orthodontic treatment. Eur J Orthod. 2012;34:238–243.
- Mourshed B, Samran A, Alfagih A, Samran A, Abdulrab S, Kern M. Anterior cantilever resin-bonded fixed dental prostheses: a review of the literature. J Prosthodont. 2018;27:266–275.
- Harada K, Raigrodski AJ, Chung KH, Flinn BD, Dogan S, Mancl LA. A comparative evaluation of the translucency of zirconias and lithium disilicate for monolithic restorations. J Prosthet Dent. 2016;116:257–263.
- Kern M, Sasse M, Wolfart S. Ten-year outcome of three-unit fixed dental prostheses made from monolithic lithium disilicate ceramic. J Am Dent Assoc. 2012;143:234–240.
- Abdel-Azim T, Rogers K, Elathamna E, Zandinejad A, Metz M, Morton D. Comparison of the marginal fit of lithium disilicate crowns fabricated with CAD/CAM technology by using conventional impressions and two intraoral digital scanners. J Prosthet Dent. 2015;114:554–559.
- Mamoun JS. On the ferrule effect and the biomechanical stability of teeth restored with cores, posts, and crowns. Eur J Dent. 2014;8:281–286.
- Hämmerle CH, Jung RE, Yaman D, Lang NP. Ridge augmentation by applying bioresorbable membranes and deproteinized bovine bone mineral: a report of twelve consecutive cases. Clin Oral Implants Res. 2008;19:19–25.
- Buser D, Chappuis V, Belser UC, Chen S. Implant placement post extraction in esthetic single tooth sites: when immediate, when early, when late? Periodontol 2000. 2017;73:84–102.
- Rokn A, Bassir SH, Rasouli Ghahroudi AA, Kharazifard MJ, Manesheof R. Long-term stability of soft tissue esthetic outcomes following conventional single implant treatment in the anterior maxilla: 10–12 year results. Open Dent J. 2016;10:602–609.
- Ariyakriangkai W, Vargas MA, Kwon SR. Management of peg-shaped maxillary lateral incisors and congenitally missing mandibular lateral incisors. Decisions in Dentistry. 2017;3(10):26–30.
- Kern M, Sasse M. Ten-year survival of anterior all-ceramic resin-bonded fixed dental prostheses. J Adhes Dent. 2011;13:407–410.
- Thompson VP, Del Castillo E, Livaditis GJ. Resin-bonded retainers. Part I: resin bond to electrolytically etched non precious alloys. J Prosthet Dent. 1983;50:771–779.
- Piemjai M, Özcan M, Garcia-Godoy F, Nakabayashi N. A 10-year clinical evaluation of resin-bonded fixed dental prostheses on non-prepared teeth. Eur J Prosthodont Restor Dent. 2016;24:63–70.
- Stylianou A, Liu PR, O’Neal SJ, Essig ME. Restoring congenitally missing maxillary lateral incisors using zirconia-based resin bonded prostheses. J Esthet Restor Dent. 2016;28:8–17.
- Wei YR, Wang XD, Zhang Q, et al. Clinical performance of anterior resin-bonded fixed dental prostheses with different framework designs: a systematic review and meta-analysis. J Dent. 2016;47:1–7
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. April 2021;7(4):8–10,12.
