
 EVGENIYSHKOLENKO/ISTOCK/GETTY IMAGES PLUS
EVGENIYSHKOLENKO/ISTOCK/GETTY IMAGES PLUS
Enhance Vision and Ergonomics With Loupes and Lights
Clinicians can improve ergonomics, visual acuity and diagnostic accuracy with the proper magnification and illumination.
Visual acuity is not only critical when performing precise movements during clinical care, it also helps sustain proper ergonomics and prevent musculoskeletal disorders (MSDs). According to the American Optometric Association, visual acuity is defined as clarity or sharpness of vision.1 Dentists operate in the oral cavity with a restricted field of vision due to limited space and lighting.2,3 In practice, they also use visual motor integration to control eye and hand coordination, so any challenges to visual acuity can compromise the efficacy of care.2–4 Additionally, deficits in visual acuity impact a dentist’s ability to accurately diagnosis diseases of the hard and soft tissues, read the periodontal probe, and evaluate radiographs — among other challenges.2,5–7 In response to these concerns, oral health professionals may wish to consider loupes and lights to improve ergonomic positioning and enhance their clinical view.
Because visual acuity naturally declines with age, dentists may compromise their ergonomics positioning to enhance their clinical view.7 Considering that many oral health professionals are practicing longer and relying on the overall strength of their bodies to extend their careers, ergonomic health and visual acuity are topics of concern.8,9 This is because visual deficiencies may impact postural positioning, thus compromising ergonomic health and increasing the risk for MSDs.3,4 This risk is exacerbated by prolonged static positions and repetitive clinical movements, especially when operating with a limited field of vision.2–4
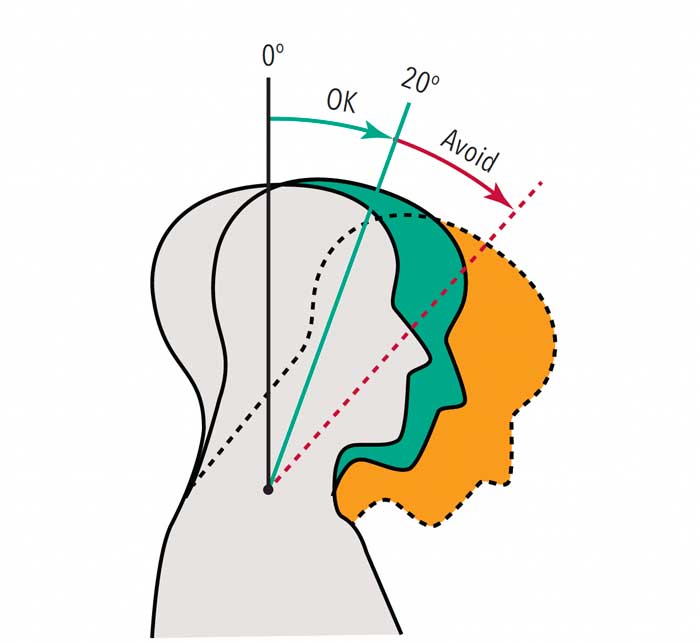
Pain and injury from MSDs are associated with the number of hours practiced weekly, and often affect the spine, shoulders, back and neck.3,8,9 Visual deficiencies may result in the head being tilted forward, overexerted neck flexion, and lack of balance. A neutral neck position should be maintained during clinical care, which encompasses a head tilt range of 0° to 15° and a neck flexion of 0° to 20°. Dentists’ neck flexion is often beyond 20°, causing neck pain (Figure 1).3,10,11 In addition, for every inch the head is tilted forward and the neck is flexed, musculoskeletal stress also increases.12 This adds strain to the cervical muscles of the neck and initiates a domino effect of abnormal forces to the spine, compromising ergonomic health.13 Furthermore, since the start of the COVID-19 pandemic, the widespread use of face shields to protect against spatter and aerosols may impact visual acuity and ergonomic health; hence, selecting a face shield that is lightweight, has a secure fit, and appropriately covers the face will help support proper neck flexion and vision.
Maintaining a neutral neck position can be challenging as visual acuity declines with age and the risk of visual deficiencies — such as presbyopia and farsightedness — increases, especially among clinicians older than 40. Presbyopia is caused by the loss of elasticity in the lens of the eye, which makes it challenging to focus on objects in close range.7,14 While dentists maintain a short working distance from the oral cavity of 27 to 50 cm,15 they also perform visual tasks at greater distances, such as when viewing radiographs or computer monitors. In addition, the expansion of electronic displays in dental settings, as well as prolonged personal electronic use, contribute to eye strain, discomfort and ocular surface changes.16 Visual deficiencies caused by age and blurred vision from presbyopia impact the ability to focus on objects in various ranges during patient care.
MAGNIFICATION AND ILLUMINATION
The use of loupes is an evidence-based strategy to improve clinical performance and ergonomics.17–19 In dentistry, both Galilean and Keplarian telescope systems are used. The Keplarian prismatic loupes have a higher magnification compared to the Galilean design. Because of their 3.5x to 8.0x magnification, Keplarian loupes have longer barrels and are heavier than Galilean loupes. This increase in magnification creates a smaller field of view, decreases the amount of light entering the lens, and is more challenging to adapt to for new users. Variable Keplarian loupes offering different levels of magnification — ranging from 3x to 5x — in a single loupe are becoming more popular with dentists. Galilean loupes offer a magnification range from 2.0x to 3.5x. With a concave lens and a convex lens, Galilean loupes produce a more distinct image than a single lens setup.20 Most general dentists require a 2.5x magnification range, whereas specialty practice (periodontics and endodontics, for example) may require magnification of 3.5x or greater.
Panoramic loupes with a 3.5x magnification are also available. The panoramic lens is rectangular; this allows for increased peripheral vision, doubling the Keplarian prismatic viewable area. This type of loupe may be ideal to see more teeth at one time.
The use of loupes improves ergonomics and reduces the risk of MSDs.6,8,9,21,22 Additionally, loupes enhance indirect vision, improve visual acuity during delicate procedures, and help address visual deficiencies among clinicians older than 40.2,6,7 Clinical vision within the oral cavity can also be enhanced with the combined use of loupes and lights.23,24
When properly fitted, loupes should be considered a foundational component to musculoskeletal health, and have been documented as an ergonomic intervention to reduce MSD prevalence and pain in the neck and back.8,9 Enhancing magnification with illumination from a headlight also improves visual acuity and supports balance. The literature, however, is limited on the impact of loupes on treatment outcomes.9
DISADVANTAGES OF LOUPES AND LIGHTS
The use of loupes and lights is not without disadvantages. A clinician’s sensorimotor may be altered while wearing loupes due to the eyes shifting from magnified to nonmagnified fields, making it challenging to maintain balance and a neutral neck position. Changes in magnification fields may also cause vertigo and eye fatigue. Providers should know the adjustment period for wearing loupes is usually two to three weeks.25–27
Both the Galilean and Keplarian loupe lenses can be mounted onto the front of the frame as a “flip up” or entrenched into the spectacle lens itself, which is known as a through-the-lens (TTL) loupe. For dentists with prescription glasses, the flip-up loupe is best because the prescription lenses can easily be placed in and out as needed. The flip-up loupe, however, is heavier than the TTL loupe. Although the fixed TTL loupe is lighter, it is also more expensive, and clinicians do not have the ability to easily switch between magnified and direct vision.
The weight and cost of loupes and lights are also considerations. Loupes and accessories cost between $850 and $2400, and lights range between $300 and $600. In regard to ergonomic health, the additional weight of loupes, lights and face shields poses risks as well. As noted, Keplarian telescope systems provide higher magnification, but are heavier than Galilean loupes; they are also more expensive. In addition, LED headlamps add weight, as some LED headlamps require an attached battery pack. Headlight systems vary greatly between manufacturers, however, and most illumination systems are offered with either cordless or corded batteries. Lights with corded batteries are often lighter on the frame. Another consideration is that at certain intensities LED illumination may harm the retina; thus it is important to verify that a headlight’s LED has white or colorless beams.28
The type of loupe and light purchased depends on the user’s individual needs. Loupes must be properly adjusted to conform to the dentist’s facial features, as even the smallest fitting error can cause eyestrain.29 As light intensities can vary, dentists should inquire about illumination products that will be both safe and comfortable. Providers should educate themselves on loupe and light brands and seek professional assistance for customized fitting before making a purchase. Other factors to consider when purchasing loupes and lights are the cost of accessories and replacement parts, as well as ease of routine care and maintenance.
SUMMARY
Dentists wishing to extend their careers should strive to maintain ergonomic health. Toward this goal, visual acuity is necessary to provide optimal care and sustain proper ergonomics. Oral health professionals should be aware of visual deficiencies and the natural process of declining vision with age. Considering the effect of visual acuity on clinical care and ergonomics, providers should have their vision evaluated regularly. The addition of loupes and lights may compensate for visual deficiencies and improve ergonomics, thereby allowing dentists to avoid MSDs, practice safely, and potentially enhance diagnosis and treatment outcomes.
KEY TAKEAWAYS
- Dentists operate in the oral cavity with a restricted field of vision due to limited space and lighting;2,3 consequently, optimizing visual acuity will aid diagnosis and treatment outcomes.
- Enhanced visual acuity also helps sustain proper ergonomics and prevent musculoskeletal disorders (MSDs) arising from the cumulative stress of daily practice.
- Integrating magnification and illumination in clinical care can help enhance visual acuity and promote ergonomic health.
- The use of loupes is an evidence-based strategy to improve ergonomics and clinical performance.17–19
- Similarly, loupe-based light systems optimize clinicians’ view of the field of operation.
- Most general dentists require a 2.5x magnification range, whereas specialty practice (periodontics and endodontics, for example) may require magnification of 3.5x or greater.
- When properly fitted, loupes should be considered a foundational component to musculoskeletal health and have been documented as an ergonomic intervention to reduce MSD prevalence.8,9
References
- American Optometric Association. Visual Acuity: What is 20/20 vision? Available at: aoa.org/patients-and-public/eye-and-vision-problems/glossary-of-eye-and-vision-conditions/visual-acuity. Accessed November 9, 2021.
- Hoerler SB, Branson BG, High AM, Mitchell TV. Effects of dental magnification lenses on indirect vision: a pilot study. J Dent Hyg. 2012;86:323–330.
- Hayes MJ, Taylor JA, Smith DR. Predictors of work-related musculoskeletal disorders among dental hygienists. Int J Dent Hyg. 2012;10:265–269.
- Hayes MJ, Smith DR, Taylor JA. Musculoskeletal disorders in a 3-year longitudinal cohort of dental hygiene students. J Dent Hyg. 2014;88:36–41.
- Bly J. Visual acuity and ergonomic health. Decisions in Dentistry. 2020;6(8):24–25.
- Arnett MC, Gwozdek AE, Ahmed S, Beaubien HD, Yaw KB, Eagle IT. Assessing the use of loupes and lights in dental hygiene educational programs. J Dent Hyg. 2017;91:15–20.
- Perrin P, Ramseyer ST, Eichenberger M, Lussi A. Visual acuity of dentists in their respective clinical conditions. Clin Oral Investig. 2014;18:2055–2058.
- Roll SC, Tung KD, Chang H, et al. Prevention and rehabilitation of musculoskeletal disorders in oral health care professionals: A systematic review. J Am Dent Assoc. 2019;150:489–502.
- Lietz J, Ulusoy N, Nienhaus A. Prevention of musculoskeletal diseases and pain among dental professionals through ergonomic interventions: a systematic literature review. Int J Environ Res Public Health. 2020;17:3482.
- Branson BG, Black MA, Simmer-Beck M. Changes in posture: a case study of a dental hygienist’s use of magnification loupes. Work. 2010;35:467–476.
- Gehrig JS, Sroda R, Saccuzzo D. Ergonomics and periodontal instrumentation. In: Fundamentals of Periodontal Instrumentation and Advance Root Instrumentation. 8th ed. Philadelphia: Wolters Kluwer; 2017:1–38.
- Kapandji AI. The Physiology of the Joints: the Spinal Column, Pelvic Girdle and Head. 7th ed. Pencaitland, Scotland: Handspring Publishing Ltd; 2019.
- Dylla JM, Forrest JL. Practice in motion: Part 1. Available at: dentalcare.com/en-us/professional-education/ce-courses/ce553. Accessed November 9, 2021.
- Eichenberger M, Biner N, Amato M, Lussi A, Perrin P. Effect of magnification on the precision of tooth preparation in dentistry. Oper Dent. 2018;43:501–507.
- Kellogg Eye Center. Refractive Errors. Available at: umkelloggeye.org/conditions-treatments/refractive-errors. Accessed November 9, 2021.
- Rosenfield M. Computer vision syndrome: a review of ocular causes and potential treatments. Ophthalmic Physiol Opt. 2011;31:502–515.
- Hart RG, Hall J. The value of loupe magnification: an underused tool in emergency medicine. Am J Emerg Med. 2007;25:704–707.
- Buller AJ, Ramchndani M, Fenerty C. Better optic disc examination: wearing loupes enhances the indirect opthalmoscope image. J Pediatr Opthalmol Strabmisus. 2006;43:102–103.
- Maggio MP, Villegas H, Blatz MB. The effect of magnification loupes on the performance of preclinical dental students. Quintessence Int. 2011;42:45–55.
- Turcotte C. How do I know when it’s time to upgrade my loupes? Dimensions of Dental Hygiene. 2021;19(4):46.
- Congdon LM, Tolle SL, Darby M. Magnification loupes in U.S. entry-level dental hygiene programs — occupational health and safety. J Dent Hyg. 2012;86:215–222.
- Khan SA, Chew KY. Effect of working characteristics and taught ergonomics on the prevalence of musculoskeletal disorders amongst dental students. BMC Musculoskelet Disord. 2013;14:118.
- Holt ER, Hoebeke R. Shine a light. Dimensions of Dental Hygiene. 2012;10(9):25–27.
- Brame JL. Seating, positioning, and lighting keep your body injury-free with these cornerstones of ergonomics. Dimensions of Dental Hygiene. 2008;6(9):36–37.
- Hayes MJ, Osmotherly PG, Taylor JA, Smith DR, Ho A. The effect of loupes on neck pain and disability among dental hygienists. Work. 2016;53:755–762.
- Sunell S, Rucker L. Surgical magnification in dental hygiene practice. Int J Dent Hyg. 2004;2:26–35.
- Branson BG, Bray KK, Gadbury-Amyot C, et al. Effect of magnification lenses on student operator posture. J Dent Educ. 2004;68:384–389.
- Stamatacos C, Harrison JL. The possible ocular hazards of LED dental illumination applications. J Tenn Dent Assoc. 2013;93:25–29.
- Shanelec DA. Optical principles of loupes. J Calif Dent Assoc. 1992;20:25–32.
From Decisions in Dentistry. December 2021;7(11):22-24.
