
 SIMPSON33/ISTOCK/GETTY IMAGES PLUS
SIMPSON33/ISTOCK/GETTY IMAGES PLUS
Endodontic Treatment Planning: Beyond Diagnosis
Advances in imaging technology and biomaterials help support successful endodontic outcomes.
Root canal therapy is a treatment modality to address periapical pathology, and early studies demonstrate the primary etiology for pulpal and periradicular disease is the progression of bacteria into the confines of the dental pulp.1 Bacterial studies have focused on how best to eradicate bacteria through chemical means, with sodium hypochlorite as the gold standard in the dissolution of tissue and bacteria from the pulpal space.2 Anatomical studies have focused on canal complexities and anatomical canal arrangements using three-dimensional cone beam computed tomography (CBCT).3 Similar technological advances have allowed for precise and effective canal preparation with both nickel titanium files and changes to the metallurgy of instrument design that increases the safety and efficiency of today’s armamentarium.4,5
The essence of appropriate endodontic therapy relies on an accurate diagnosis in order to properly treat the canal space and remove the bacteria within its confines. A proper diagnosis can only be established when clinicians understand the chief complaint, establish clinical tests — including periodontal probings, sensibility testing, and percussion and palpation tests — and interpret the necessary radiographic imaging. Once a diagnosis is achieved, it is paramount to answer three additional questions: What is the etiology of this diagnosis? How does it affect prognosis? And how can the diagnosis and etiology be used with advanced imaging, products and materials to achieve the best outcome? This article detail how advances in imaging, technology and biomaterials may be used in the context of etiology and prognosis to aid in treatment choices.
Since its introduction, the use of CBCT in endodontics has been steadily increasing. A 2017 survey of 1083 endodontists reveals that 80% of the respondents had access to a CBCT unit.6 Due to its increasing use, the American Association of Endodontists (AAE) and American Association of Oral and Maxillofacial Radiology (AAOMR) published a joint position paper in regard to its use in endodontics.7 While it provides recommendations and rationale for the use of CBCT, the paper stopped short of calling it the “standard of practice.” Rather, it presented CBCT as “the imaging modality of choice” in these particular areas:
- Diagnosis when there is contradictory or non-specific signs and symptoms of endodontic disease
- Preoperative imaging if extra canals or morphological aberrations are suspected
- Intra-appointment imaging to locate calcified canals
- Retreatment if conventional X-rays are inconclusive for a potential vertical root fracture
- Evaluation of nonhealing endodontically treated teeth to determine the necessity and options for additional care
- Presurgical assessments both for implant placement and apical surgery
- Evaluation of procedural errors (e.g., extrusion or file separation)
- Trauma-related cases to limited dento-alveolar fractures or luxation
When CBCT images are utilized, a proper interpretation of the periapical tissue, and an evaluation of the anatomical configuration of the root structure (in regard to length, width, curvature, canal size and available dentin) are necessary. A clinician who overlooks these aspects of information on a CBCT may be missing crucial data that will help guide the method of care.
IRRIGATION TECHNOLOGY
The future emphasis in endodontics appears to be shifting in regard to clinicians’ ability to irrigate the complex anatomical areas of the canal system. As with rotary instrumentation, magnification and CBCT, years of research are necessary to present a body of evidence that suggest the changes to clinical care meet a new standard of practice.8 Traditionally, endodontic irrigation has relied on irrigant delivered via a syringe and side-vented irrigation needles. This type of irrigation creates a positive pressure irrigant that, at its worst, can be toxic and dangerous if irrigants are positively expressed beyond the apical terminus. Caution in irrigation usually results in providers choosing to stay 2 to 3 mm coronal to the canal apex when placing the irrigant. Recent studies have evaluated the efficacy of irrigants with adjunct methods of delivery or agitation, including negative pressure systems, acoustic energy or ultrasonic activation. This research has shown favorable outcomes in regard to the ability to remove debris from the canal system.9–11 These advances may indeed change how the anatomical spaces of the canal are cleaned and shaped.
BIOCERAMIC MATERIALS
Bioceramics have been utilized for years in the dental field, and most notably in endodontic microsurgical root end fillings.12 The most utilized bioceramic material has been mineral trioxide aggregate.13 Slight changes to the composition of bioceramics have allowed for additional products in the areas of endodontic sealers, as well as filling materials that allow for bioactivity.14,15 Calcium silicate bioceramics have been shown to be an adequate dentin replacement material with bioactive properties that can withstand the oral environment and forces necessary to serve as a restoration.16,17 Bioceramic advances have the ability to change how clinicians obturate particular cases, such as perforations, open apices, or other areas with concern in regard to materials in close proximity to periapical tissues.
The following cases present examples of how the utilization of technology can positively impact endodontic treatment plans, as well as treatment decisions. It should be noted that all cases were treated under normal endodontic procedures with rubber dam isolation and use of an operating microscope.
CASE 1
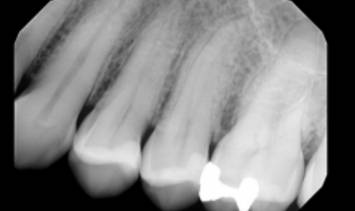
A 46-year-old female presented with a chief complaint of pain on the maxillary left premolar area. Diagnostic testing revealed periodontal probings less than 4 mm, with no bleeding on probing. Sensibility testing revealed no response on tooth #12, with positive responses on all other teeth in the quadrant. Tooth #12 was +1 percussion sensitive, with all other teeth within normal limits (WNL) to percussion and palpation. A periapical radiograph (PA) was supplied for evaluation (Figure 1A). The radiograph appears WNL, with a normal periapical appearance associated with tooth #12. Diagnosis: #12 necrosis/symptomatic apical periodontitis.
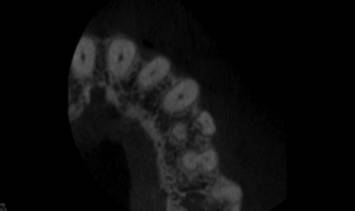
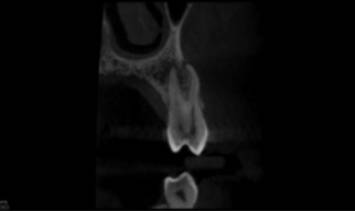
A CBCT image was taken preoperatively (Figure 1B). The limited field of view (FOV) CBCT axial view showed three canals. Multiple studies reveal this anatomical configuration has a prevalence of less than 5% in the general population.3,18 The coronal view also revealed a severe curvature of the buccal root, with limited dentin thickness and decreased density at the apex of the buccal and lingual roots (Figure 1C). Based on this information, the treatment plan changed to a conservative instrumentation technique with a maximum canals enlargement of 15/.04. With limited canal enlargement for irrigation, a technique utilizing a negative pressure irrigation system with a chemo-acoustic technology was chosen. It should be noted that intraoperatively only two canals were located with rotary instrumentation. A resin sealer with a single cone obturation technique with minimal warm vertical compaction was utilized.19
The interoperative radiograph (Figure 1D) revealed a conservative instrumentation technique enhanced with the chemo-acoustic irrigation technique. The
final radiograph shows obturation to the terminus of all three canals (Figure 1E).

second buccal canal.

At a three-month recall appointment, the patient had been asymptomatic and functional. The periodontal probings were all less than 4 mm. Tooth #12 was negative to percussion and palpation. A recall CBCT image was taken to evaluate the effectiveness of the treatment technique. A coronal view revealed an increased density at the apex, with an intact lamina dura (Figure 1F). Tooth #12 has been properly restored with a full coverage restoration.

CASE 2
A 28-year-old male presented for evaluation with a chief complaint of intermittent cold sensitivity on the maxillary right. Diagnostic testing revealed periodontal probings less than 4 mm, with no bleeding on probing. Sensibility testing revealed a slightly lingering response to cold on tooth #3, with positive normal responses on all other teeth in the quadrant. All teeth in the quadrant were WNL to percussion and palpation. A bitewing (BW) radiograph sent from his restorative dentist (Figure 2A) revealed a radiolucency within the pulp chamber. Based on the BW radiograph, a limited FOV CBCT was suggested. The CBCT axial view revealed internal root resorption, with potential perforation on the furcal side of the palatal root (Figure 2B). The CBCT coronal view revealed extensive internal resorption throughout the palatal root (Figure 2C). The diagnosis of tooth #3 was irreversible pulpitis/symptomatic/normal periodical.

radiolucency within the coronal tooth structure.


With the diagnosis and etiology in mind, a discussion in regard to options and potential prognosis took place with the patient. Despite the extensive resorption and questionable prognosis, the patient chose to attempt to retain tooth #3. With an understanding of the etiology and desire to remove or arrest the clastic cells contributing to the etiology, a chemo-acoustic irrigation technique was chosen. Following access, instrumentation, and the application of chemo-acoustic technology (Figure 2D), the remaining tooth structure could be visualized with the operating microscope. The canals were obturated with a bioceramic sealer and gutta-percha. The gutta-percha was removed from the coronal one-half of the palatal root, and the remaining canal space, as well as cervical and pulpal floor, was filled with a bioceramic restorative material. The access was restored with a composite restoration (Figure 2E). Despite the endodontic therapy, the patient was monitored for six months prior to any definitive cuspal coverage. The patient returned for a six-month recall asymptomatic, and all periodontal probings were less than 4 mm. Tooth #3 was negative to percussion and palpation. A PA radiograph (Figure 2F) revealed no advancement of the resorptive defect at this time. Clinically, a full-coverage restoration on tooth #3 was suggested, and the prognosis was changed from questionable to favorable.



CASE 3
A 69-year-old male presented for endodontic therapy on tooth #19. His chief complaint was slight tenderness when biting on the left side. An exam indicated all periodontal probings were less than 4 mm on tooth #19. Sensibility testing revealed #19 was nonresponsive to cold, with adjacent teeth responding to sensibility testing. Tooth #19 was +1 to percussion and negative to palpation, with all other teeth in the quadrant WNL to percussion/palpation. Tooth #19 was restored with an occlusal amalgam and fracture lines were noted on the mesial and distal marginal ridge. The patient’s BW and PA radiographs were sent for evaluation (Figure 3A). The PA radiograph revealed a diffuse periapical radiolucency associated with the distal root and widening of the ligament on the distal root (Figure 3B). The diagnosis of tooth #19 was necrosis/symptomatic apical periodontitis.

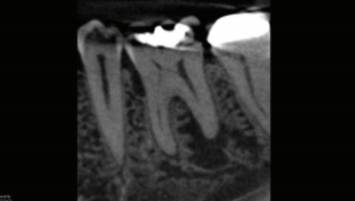
A limited FOV CBCT was taken preoperatively (Figure 3C). The axial view revealed a well-localized cervical bone loss along the mesial root. This corresponds to the fracture noted on the mesial marginal ridge. Despite the bone loss, the location did not allow for periodontal probing of the defect. In the endodontic literature, a few clinical findings have been associated with a decreased prognosis of teeth treated with endodontic therapy. Teeth exhibiting mesial and distal fracture, terminal teeth, and teeth with periodontal pockets greater than 5 mm exhibited success ranging from 31% to 74%, which is a considerable difference compared to teeth that do not exhibit fractures.20,21 A cohort study followed cracked teeth for two to four years after root canal therapy and found no difference in the survival rate of teeth with cracks up to 5 mm into the canal.22 Despite the differing opinions in the literature in regard to the best treatment for cracked teeth, early detection and discussion with patients are paramount in treatment planning. This case demonstrates how the use of limited FOV CBCT may allow for discussing the long-term prognosis of endodontic therapy before clinical signs are discernable. Based on an understanding of the extent of the fracture in this case and discussion with the patient, tooth #19 was removed and replaced. Certainly, other factors play into the treatment decision with each patient, but knowledge of pulpal and periradicular etiological factors is paramount in discussing prognoses.

CONCLUSION
What happens after the diagnosis of endodontic therapy is dependent on the information gathered. The decision to retain the natural dentition must be based on the etiology and how to utilize materials to maximize biological principles of success and failure. All three of these cases present challenges to endodontic treatment protocols. In each case, the information provided through CBCT imaging aided the discussion of etiology and prognosis, and ultimately helped determine the treatment plan.
In the first case, the information of additional canals, location of canals and anatomical challenges allowed for using a new irrigation technique to address the biological needs. The second case led to decisions to utilize both new technology in irrigation and biomaterials to aid in the long-term prognosis. Lastly, in the third case, information gathered from the CBCT offered insights into the etiology of pulpal pathology. This understanding allowed a discussion in regard to prognosis that ultimately aided the patient’s treatment decision.
In addition to an accurate diagnosis, an understanding of anatomical and biological complexities becomes paramount in gathering the knowledge to inform patients of treatment prognoses. Based on the aggregate of this information, the clinician should be able to make better decisions when choosing methods and materials for endodontic therapy.
REFERENCES
- Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol. 1965;20:340–349.
- Siqueira JF, Batista MMD, Fraga RC, de Uzeda M. Antibacterial effects of endodontic irrigants on black-pigmented Gram-negative anaerobes and facultative bacteriaJ J Endod. 1998;24:414–416.
- Bürklein S, Heck R, Schäfer E. Evaluation of the root canal anatomy of maxillary and mandibular premolars in a selected German population using cone-beam computed tomographic data. J Endod. 2017;43:1448–1452.
- Esposito PT, Cunningham CJ. A comparison of canal preparation with nickel-titanium and stainless steel instruments. J Endod. 1995;21:173–176.
- He R, Ni J. Design improvement and failure reduction of endodontic files through finite element analysis: application to v-taper file designs. J Endod. 2010;36:1552–1557.
- Setzer FC, Hinckley N, Kohli MR, Karabucak B. A survey of cone-beam computed tomographic use among endodontic practitioners in the United States. J Endod. 2017;43:699–704.
- AAE/AAOMR Joint Position Statement — Use of Cone Beam Computed Tomography in Endodontics — 2015/2016 update. Available at: https://f3f142zs0k2w1kg84k5p9i1o-wpengine.netdna-ssl.com/specialty/wp-content/uploads/sites/2/2017/06/conebeamstatement.pdf. Accessed May 30, 2020.
- Endodontics Colleagues for Excellence 2014. Available at: https://f3f142zs0k2w1kg84k5p9i1o-wpengine.netdna-ssl.com/specialty/wp-content/uploads/sites/2/2017/07/col035fall2014standardofpracticeupdate.pdf. Accessed May 30, 2020.
- Chan R, Versiani MA, Friedman S, et al. Efficacy of 3 supplementary irrigation protocols in the removal of hard tissue debris from the mesial root canal system of mandibular molars. J Endod. 2019;45:923–929.
- Ma J, Shen Y, Yang Y, et al. In vitro study of calcium hydroxide removal from mandibular molar root canals. J Endod. 2015;41:553–558.
- Molina B, Glickman G, Vandrangi P, Khakpour M. Evaluation of root canal debridement of human molars using the GentleWave System. J Endod. 2015;41:1701–1705.
- Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review — part III: clinical applications, drawbacks, and mechanism of action. J Endod. 2010;36:400–413.
- Kaur M1, Singh H, Dhillon JS, Batra M, Saini M. MTA versus Biodentine: review of literature with a comparative analysis. J Clin Diag Res. 2017;11:ZG01–ZG05.
- Jafari F, Jafari S. Composition and physicochemical properties of calcium silicate based sealers: a review article. J Clin Exp Dent. 2017;9:e1249–e1255.
- Giacomino CM, Wealleans JA, Kuhn N, Diogenes A. Comparative biocompatibility and osteogenic potential of two bioceramic sealers. J Endod. 2019;45:51–56.
- Aktemur Türker S, Uzunoğlu E, Deniz Sungur D, Tek V. Fracture resistance of teeth with simulated perforating internal resorption cavities repaired with different calcium silicate–based cements and backfilling materials. J Endod. 2018;44:860–863.
- Silva LA, Pieroni KA, Nelson-Filho P, et al. Furcation perforation: periradicular tissue response to biodentine as a repair material by histopathologic and indirect immunofluorescence analyses. J Endod. 2017;43:1137–1142.
- Ahmad IA, Alenezi MA. Root and root canal morphology of maxillary first premolars: a literature review and clinical considerations. J Endod. 2016;42:861–872.
- Iglecias EF, Freire LG, Candeiro GT, Santos M, Antoniazzi JH, Gavini G. Presence of voids after continuous wave of condensation and single-cone obturation in mandibular molars: a micro-computed tomography analysis. J Endod. 2017;43:638–642.
- Krell KV, Caplan DJ. 12-month success of cracked teeth treated with orthograde root canal treatment. J Endod. 2018;44:543–548.
- Kang SH, Kim BS, Kim Y. Cracked teeth: distribution, characteristics, and survival after root canal treatment. J Endod. 2016;42:557–562.
- Davis MC, Shariff SS. Success and survival of endodontically treated cracked teeth with radicular extensions: a 2- to 4-year prospective cohort. J Endod. 2019;45:848–855.
The author discloses he consults for Sonendo and Dentsply Sirona.
From Decisions in Dentistry. June 2020;6(6):12–15.
