
 GRAPHIC PHOTOART / ISTOCK / GETTY IMAGES PLUS
GRAPHIC PHOTOART / ISTOCK / GETTY IMAGES PLUS
Early Intervention in Pediatric Malocclusion
Hengsheng Lin, BDS, MSD, and Jun Yao, DDS, PhD, discuss how space management and correcting crossbite in children can help support a lifetime of oral health.
Occlusal issues deserve prompt attention, especially with pediatric patients, in whom early diagnosis and treatment can prevent conditions from worsening — and also help set children on a lifelong path of oral health. For insights into malocclusion, Decisions in Dentistry asked pediatric specialists Hengsheng Lin, BDS, MSD, and Jun Yao, DDS, PhD, to share their thoughts on managing occlusal discrepancies in children and adolescents.
Why is it important to manage occlusal discrepancies in the pediatric population?
Having a strategy to manage an existing or developing dental anomaly or occlusal discrepancy is an integral part of comprehensive pediatric oral care. Children will not outgrow the majority of these issues, and the problems often become worse over time. In cases involving pediatric malocclusion, it is most effective to intervene in primary or early mixed dentition to reduce the severity of dental and occlusal problems and avoid future treatment complications.
Pediatric dentists and general dentists are usually the first to detect a child’s malocclusion. Some well-accepted benefits of early orthodontic treatment are that it can eliminate or reduce the severity of a developing malocclusion, and reduce the length and complexity of future orthodontic treatment. It also has the potential to correct problems in skeletal growth, and may reduce the need for extraction of permanent teeth during Phase II orthodontic treatment. In addition, correcting severely protruded upper anterior teeth can significantly reduce dental trauma. Perhaps most importantly, any of these interventions can promote a child’s self-esteem.
What are the goals of early management?
Early management includes preventive and interceptive orthodontic therapies. Early treatment can begin in primary dentition if there is functional deviation, and in early mixed dentition (when all incisors and permanent first molars have erupted) if there are crowding or skeletal problems. Clinicians can also delay treatment until the permanent dentition is in place.
The goal of treatment — and the benefits of early versus late intervention — must be clearly communicated to patients, parents and caregivers. The core goals of treatment are to intercept malocclusions before they become worse, and guide the outcome toward a positive result.
Briefly, can you describe the relationship between orthodontic concerns and dentoalveolar and skeletal issues in children.
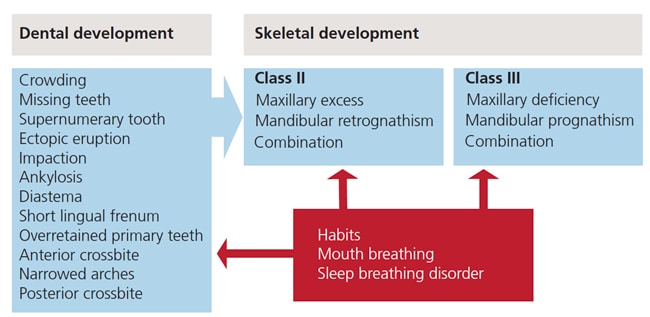
Orthodontic issues can start as early as the eruption of the first tooth. Most dentoalveolar and skeletal problems develop during the mixed dentition period. The soft tissues also play an important role in existing dental or skeletal problems (Figure 1). Treatment modalities can be easily explained in three malocclusion classes: Class I, Class II and Class III (Table 1).
The comprehensive management of early malocclusion in children and adolescents must take into account dental, skeletal and soft tissue problems, and their interrelationships. Successful early orthodontic treatment necessitates a comprehensive evaluation of craniofacial growth, occlusal and dental development, treatment mechanics, the patient’s behavior, and parental/caregiver expectations. Clinicians must develop a thorough diagnosis and definitive treatment plan with clearly set goals.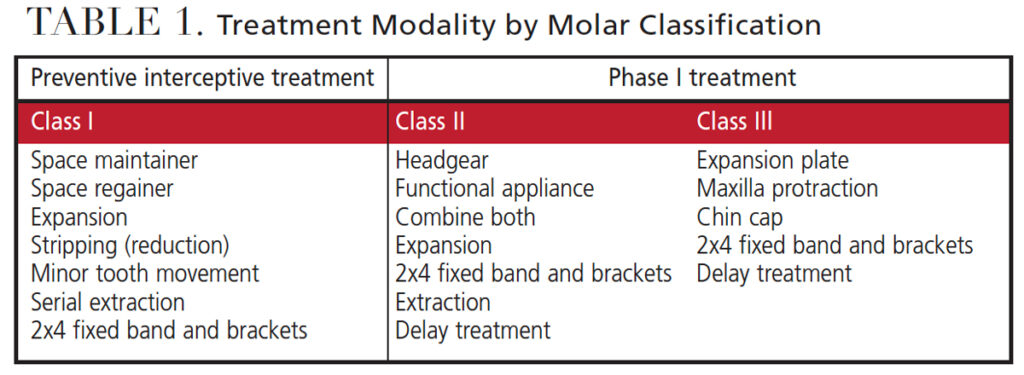
Which organizational approach do you suggest in treatment planning?
Treatment protocols should be divided into separate phases. The goal of the first phase (Phase I orthodontic treatment) is to intercept existing abnormalities, or reduce the severity of problems in primary and early mixed dentition. The next step is a supervision phase after completion of Phase I treatment, with the goal of retaining the first phase results and monitoring occlusal and dental development. The second orthodontic treatment phase (Phase II orthodontics) or comprehensive treatment phase is to make detailed adjustments of the dentition, as needed.
What are some of the key considerations in space management for primary dentition?
Often, primary incisors are lost due to caries or trauma. This leads to very little change in the primary arch length and does not require space maintenance. An upper lingual arch with teeth, such as the Groper’s appliance, is an option for esthetic concerns, but is not required for orthodontic space maintenance (Figure 2).
When the loss of a primary canine is caused by caries, a space maintainer is not required in this stage. The loss of a primary first molar alone usually does not require a space maintainer in primary dentition when the primary second molar is retained. The loss of primary second molars generally requires a space maintainer, especially when the permanent first molar is actively erupting.

How does crowding factor in?
Crowding is the most common orthodontic issue for patients of all ages. It initiates with incisor liability — the size discrepancy between the primary incisors and permanent incisors. The sum of the maxillary four permanent incisors is, on average, 7.6 mm larger than the primary incisors, and the sum of the mandibular four permanent incisors is 6.0 mm larger than the primary incisors.1
Providers can compensate for this space discrepancy via interdental spacing in primary incisors, labial eruption of permanent incisors, distal movement of mandibular primary canines by lateral incisor forces, and increases in inter-canine width.
Please share your thoughts regarding space management in mixed dentition.
The majority of crowding in the mixed dentition is a combination of tooth size discrepancy and arch length deficiency, and is exacerbated by premature loss of primary teeth due to caries. The management of space issues requires consideration of early correction of incisor crowding, and preservation of leeway space. The early preservation of leeway space can alleviate 72% of crowding cases.2 The well-planned, early use of leeway space can assist in the normal eruption of permanent canines and premolars.
The most common space loss in mixed dentition is premature loss of either one or both lower primary canines. This can create a series of problems; for example, the incisors could tip lingually and distally, resulting in a mandibular dental midline shift; an anterior overjet could increase and deepen the anterior overbite; the permanent canines could erupt ectopically or become impacted; and both arch length and perimeter could be reduced. Almost all articles and textbooks instruct clinicians to extract the contra-lateral primary canine if one is lost prematurely. The goal of this extraction is to maintain symmetry of the lower midline by allowing mandibular anteriors to make a distal shift bilaterally.3–6 This strategy will require future extraction of permanent premolars in a lateral orthodontic treatment of a bilateral loss of primary canines.

What does research suggest about crossbite in primary and mixed dentition?
Posterior crossbite is one of the common problems in mixed dentition. The crossbite can be unilateral or bilateral, a single tooth or a group of posterior teeth, dental or skeletal, or a combination of these. Prevalence is 5% to 8% in U.S. studies, and 4% to 23% in European studies.7,8 Crossbite etiology can include hereditary factors, congenital anomalies, constriction of the maxilla, mouth breathing, nonnutritive sucking habits, localized tooth interference, atypical eruption problems, and trauma.
In primary dentition, 90% of crossbites involve the primary canine and first and second primary molars. The primary lateral incisor is also involved in 60% of cases. Posterior crossbites present with constricted maxilla, reduced inter-canine width, and functional shift at closure, with the chin shifting to the crossbite side. With this shift, the condyle rotates on its axis and translates downward and forward on the non-crossbite side. Therefore, the crossbite side appears as a Class II occlusion or distal step, while the non-crossbite side appears as a Class I/III occlusion or mesial step (Figures 3A through 3C). If left untreated, this functional shift will result in asymmetric jaw growth and the potential for temporomandibular joint disorders.9–11
Please describe treatment approaches for crossbite.
Bilateral posterior crossbites are usually skeletal in origin. Arising from a constricted maxilla, in most cases bilateral posterior crossbites have no functional shift and no midline discrepancy. They are often associated with mouth breathing, anterior open bite or dolichocephalic growth. It is important to accurately diagnose a unilateral posterior or bilateral posterior crossbite with functional shift before initiating treatment. The first step is to check the centric relation (CR) and centric occlusion (CO). A true unilateral posterior crossbite does not shift from CR to CO. The second step is to examine the symmetry of the maxillary arch. A true posterior crossbite presents with asymmetry of the arch, with narrowing on the crossbite side.
Early intervention in posterior crossbites is simple, effective and stable. The best age to intervene is in late primary dentition or early mixed dentition. Up to 45% of posterior crossbites in primary dentition are self-correcting upon development of the permanent dentition.12
Common treatment modalities for posterior crossbite include:
- Eliminating any patient habits associated with the posterior crossbite.
- Removing tooth interference that causes a CR/CO shift; this can correct unilateral crossbite partially or completely in primary dentition.
- Assisting in maxillary and/or mandibular expansion using various appliances, such as the quad-helix, W-arch and others (Figures 4A and 4B).

Any final thoughts?
Most parents and caregivers do not wish to see a child’s self-esteem negatively affected by poor occlusion and esthetics. Understanding the benefits of improving a child’s appearance and correcting malocclusion at an early age is of value to all dental providers. These malocclusions include premature space loss, arch size/tooth size discrepancy, anterior crossbite, posterior crossbite, and craniofacial development problems.
Trends show that parents and caregivers are seeking orthodontic treatment for children at an earlier age. It has been demonstrated that many early dental and skeletal anomalies can be corrected or reduced in severity in primary or early mixed dentition by clinicians who remain abreast of the latest developments in this area of treatment.
Key Takeaways
- Early diagnosis and treatment of pediatric occlusal issues can prevent conditions from worsening, and help set children on a lifelong path of oral health.
- In cases involving pediatric malocclusion, it is most effective to intervene in primary or early mixed dentition to reduce the severity of dental and occlusal problems and avoid future treatment complications.
- Early treatment can begin in primary dentition if there is functional deviation, and in early mixed dentition (when all incisors and permanent first molars have erupted) if there are crowding or skeletal problems. Clinicians can also delay treatment until the permanent dentition is in place.
- Management of early malocclusion in children and adolescents must take into account dental, skeletal and soft tissue problems, and their interrelationships.
- Crowding is the most common orthodontic issue for patients of all ages.
- Posterior crossbite is a common problem in the mixed dentition.
- The goal of treatment — and the benefits of early versus late intervention — must be clearly communicated to patients, parents and caregivers.
References
- Mayne WR. Serial extraction. In: Graber TM, Swain BF, eds. Current Orthodontic Concepts and Techniques. 2nd ed. Philadelphia: WB Saunders; 1969.
- Gianelly AA. Crowding: timing of treatment. Angle Orthod. 1994;64:414–418.
- Shapira Y, Kuftinec M. The ectopically erupted mandibular lateral incisor. Am J Orthod. 1982;82:426–438.
- Hollander CS, Full CA. Midline correction by extraction of the remaining mandibular canine — myth or reality. J Dent Child. 1992;59:207–211.
- Atkinson CD. The case against early extraction of mandibular primary canines. J Am Dent Assoc. 1982;104:302–304.
- Sayin MO, Türkkahraman H. Effects of lower primary canine extraction on the mandibular dentition. Angle Orthod. 2006;76:31–35.
- Bell R, Kiebach T. Posterior crossbites in children: developmental-based diagnosis and implications to normative growth patterns. Semin Orthod. 2014;20:77–113.
- Kutin G, Hawes RR. Posterior cross-bites in the deciduous and mixed dentitions. Am J Orthod. 1969;56:491–504.
- Hesse KL, Artun J, Joondeph DR, Kennedy DB. Changes in condylar position and occlusion associated with maxillary expansion for correction of functional unilateral posterior crossbite. Am J Orthod Dentofacial Orthop. 1997;111:410–418.
- Myers DR, Barenie JT, Bell RA, Williamson EH. Condylar position in children with functional posterior cross-bite: before and after crossbite correction. Pediatr Dent. 1980;2:190–194.
- Pinto AS, Buschang PH, Throckmorton GS, Chen P. Morphological and positional asymmetries of young children with functional unilateral posterior crossbite. Am J Orthod Dentofacial Orthop. 2001;120:513–520.
- Malandris M, Mahoney EK. Aetiology, diagnosis and treatment of posterior cross-bite in the primary dentition. Int J Pediatr Dent. 2004;14:155–166.
From Decisions in Dentistry. June 2022;8(6)10,13-14,16.
