
 DANIELZGOMBIC/E+/GETTY IMAGES PLUS
DANIELZGOMBIC/E+/GETTY IMAGES PLUS
Digital Workflow for Porcelain Veneers
With the use of digital planning and digital workflows, clinicians can help ensure streamlined veneer treatment and predictable outcomes.
This case presentation illustrates the advantages of using a digital workflow in porcelain veneer treatment. Digital planning is a clinically helpful tool that aids precision, reduces chairtime, and allows visualization of the future treatment outcome.1,2 A digital workflow includes digital photographs, digital models of the patient, and digital communication with the dental laboratory or in-office design and fabrication system in order to achieve the final goal.
The case involves a 22-year-old female who presented to the Advanced Education in General Dentistry clinic at the University of Connecticut School of Dental Medicine. Her chief complaint was that she wanted to “cover or hide the stains on her front teeth” (Figure 1). The patient’s medical history proved nonsignificant, and she had no known drug allergies.

stained teeth.
A clinical examination of the patient was completed, with her periodontal diagnosis being gingivitis associated with dental biofilm alone. No caries were noted. Initial treatment consisted of oral hygiene instructions and a prophylaxis. When asked about the staining on her teeth, she indicated she was unsure of the origin. The patient did not have a history of orthodontic treatment, and reported no knowledge of being on antibiotics (such as tetracycline) as a child or having water-induced fluorosis.
The stains were determined to be intrinsic, as they could not be removed by pumice. The clinical team recommended the patient undergo home bleaching to decrease the intensity of the stains, followed by treatment with porcelain veneers. The patient agreed to the treatment plan and consent was obtained.
Lithium disilicate porcelain veneers were recommended due to the minimal tooth preparation required and ability to mask discoloration that might remain after bleaching and tooth preparation. Bonded porcelain veneers have been a hallmark treatment that is supported by evidence-based literature.3–6 After consulting the patient, a decision was made to fabricate veneers for teeth #6 through 11. The premolars were not included to minimize patient costs.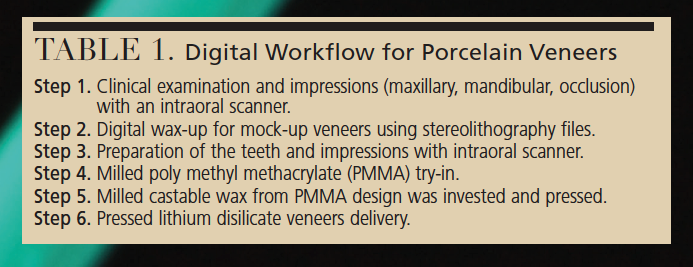
As noted, the patient accepted the plan and understood that veneer treatment would begin following the completion of bleaching. The patient was given a professionally supervised home-bleaching regimen, following the manufacturer’s directions. After a few weeks, the whitening treatment resulted in a reduction of the intrinsic stains and improvement in tooth color. The patient reported being satisfied with the outcome; in addition, clinical consensus among the team was that bleaching results were better than expected. At this point, a final decision was made to utilize a digital workflow in designing and fabricating the veneers for this patient (Table 1).

digital impression.
DIGITAL PLANNING
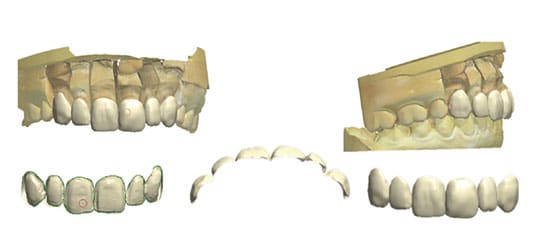
An intraoral digital impression was achieved which was converted to a stereolithography (STL) file using special software (Figure 2). The STL files were introduced into additional software systems for design and fabrication of a digital wax-up (Figure 3). The digital wax-up was fabricated with a three-dimensional (3D) printer and presented to the patient, who approved the wax-up.
Teeth #6 through 11 were minimally prepared for lithium disilicate press veneers (Figures 4A and 4B). The margins were kept in enamel for predictable bonding of the veneers. The prepared teeth were scanned to enable the laboratory to print 3D models.

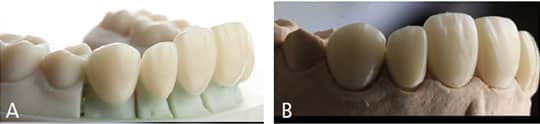
Initially, the laboratory was advised to follow digital wax-up in order to fabricate milled poly methyl methacrylate (PMMA) veneers. A PMMA provisional was utilized to check the accuracy of the fit and esthetics of the wax-up created with the digital workflow (Figures 5 and 5B). The resulting PMMA provisional adapted perfectly to the teeth, and the patient reported being pleased with the esthetics.
DISCUSSION
Permanent lithium disilicate press veneers for teeth #6 through 11 were ordered. The decision to prescribe pressed versus milled veneers was due to the minimal tooth preparation needed, and to maximize esthetics. In cases such as this, a skilled laboratory technician is essential in layering ceramic that can opaque-out remaining stain in the natural teeth, but create translucencies to mimic natural enamel structure. Studies report a thickness of 0.5 to 1 mm facial reduction on these veneer preparations is sufficient for longevity of the pressed restorations when bonded to the tooth.7 Preservation of enamel for successful bonding is key to increased bond strength and, ultimately, strength of the veneers. Fabrication of the pressed laminate veneers was perhaps the only step in this process that was not truly digital. In the future, updates in software and materials may allow layering of such veneers in a completely digital manner. The veneers were delivered with minimal adjustments, and the patient reported being completely satisfied (Figures 6A through 6E).

CONCLUSION
Based on the current protocol and experience of the authors, there is a clear advantage to using a digital workflow for veneer treatment. Digital planning reduces chairtime and improves lab communication, as well as communication between the clinical team and patient. The resulting veneers exhibited accurate marginal adaptation and excellent esthetics. Studies with larger patient groups are warranted in order to evaluate the repeatability and accuracy of this protocol.
KEY TAKEAWAYS
- In veneer treatment, digital planning is a clinically helpful tool that aids precision, reduces chairtime, and allows visualization of the future treatment outcome.1,2
- In this case, lithium disilicate porcelain veneers were recommended due to the minimal tooth preparation required and ability to mask discoloration that might remain after bleaching and tooth preparation.
- Following digital impressions and design, a digital wax-up was fabricated with a three-dimensional printer and presented to the patient.
- poly methyl methacrylate (PMMA) provisional was utilized to check the accuracy of the fit and esthetics of the wax-up created through the digital workflow.
- The resulting PMMA provisional adapted perfectly to the patient’s teeth.
- After laboratory fabrication, the final veneers were delivered with minimal adjustments, and the patient reported being pleased with the esthetics.
REFERENCES
- Coachman C, Calamita M. Digital smile design: A tool for treatment planning and communication in esthetic dentistry. Quintessence Dent Technol. 2012;35:101–109.
- Coachman C, Van Dooren E, Gürel G, Landsberg CJ, Calamita MA, Bichacho N. Smile design: From digital treatment planning to clinical reality. In: Cohen M, ed. Interdisciplinary Treatment Planning. Vol 2: Comprehensive Case Studies. Chicago: Quintessence Publishing Co; 2012:119–174.
- Calamia JR, Calamia CS. Porcelain laminate veneers: reasons for 25 years of success. Dent Clin N Am. 2007;51:399–417.
- Strassler HE. Minimally invasive porcelain veneers: Indications for a conservative esthetic dentistry treatment modality. Gen Dent. 2017;55:686–694.
- Magne P, Belser U. Bonded Porcelain Restorations in the Anterior Dentition: A Biomimetic Approach. Chicago: Quintessence Publishing Co; 2002.
- Christopher CK, Grobler B. Porcelain veneers: Treatment guidelines for optimal aesthetics. Australas Dent Prac. 2011;22:154–164.
- Begum Z, Chheda P, Shruthi CS, Sonika R. Effect of ceramic thickness and luting agent shade on the color masking ability of laminate veneers. J Indian Prosthodont Soc. 2014;14(Suppl 1):46–50.
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. October 2019;5(9):21—23.
