
 GRISTIARA/ISTOCK/GETTY IMAGES PLUS
GRISTIARA/ISTOCK/GETTY IMAGES PLUS
Desktop 3D Printing for Occlusal Splints
This case presentation describes the process of using a digital workflow for the fabrication of occlusal guards.
Computer aided design/computer aided manufacturing (CAD/CAM) has come into prominence in many industries, including dentistry. It has advanced to the point it can be used for a wide range of dental applications.1 The workflow for creating computer generated devices had been underutilized due to equipment cost, a limited amount of approved materials, and a traditionally complex workflow.2 Today, newer technologies have brought down costs. In addition, new materials have been introduced for a broad range of services, and improved workflows allow integration with different manufacturing systems. As a result, CAD/CAM use in the dental office is rapidly increasing. Embracing digital dentistry can be accomplished in-office with or without the assistance of a dental laboratory in planning and fabricating various types of appliances (e.g., occlusal splints), restorations and surgical guides.3–6 As an example of the possibilities, this article will describe the design and fabrication of an occlusal appliance using an in-office scanner and three-dimensional (3D) printing technology.
The glossary of prosthodontic terms defines occlusal appliance/device as “any removable artificial occlusal surface affecting the relationship of the mandible to the maxillae used for diagnosis or therapy.”7 The use of occlusal appliances in the diagnosis, relief, management, and prevention of discomfort from occlusal discrepancies, orofacial pain, obstructive sleep apnea, bruxism, and patients undergoing orthodontic or comprehensive prosthodontic/restorative rehabilitation has been well described.8–16
Bruxing and grinding has been reported to occur in up to 37% of certain populations.17 The prevalence of obstructive sleep apnea has been reported to range between 9% and 38%.18 In addition, the American Dental Association has identified 29 sports for which a mouthguard is recommended.19 Considering the prevalence of these type of patients, a proper diagnosis, identifying all causative etiologic factors, developing patient-specific treatment, and considering the potential use of appropriate occlusal devices will help clinicians provide optimal care.

the scanned maxillary cast.
Conventional (or analog) fabrication of occlusal appliances using traditional laboratory techniques — involving impression materials, dental stone, cast fabrication, trimming, designing, processing and finishing — can be time consuming. This approach can also produce appliances of variable quality and consistency. Intralab and interlab variability can result from cast trimming, wax adaptation and acrylic processing, as well as grinding and polishing. Remaking an appliance for a patient, even if it is by the same technician, will also result in slight changes from the original.

In comparison, digital fabrication can provide consistency, quantitative control and speed, while eliminating some or all of these the physical materials (such as impressions, stone casts and waxing). A digital workflow uses an optical scanner to capture the anatomy, CAD software to design the appliance, and a CAM system to mill or print the appliance.1–6
This can be a completely digital process, although a combination digital/analog approach (using some conventional techniques) is also possible. The latter might include making a conventional dental impression and having the lab scan the impression or stone cast, design the appliance, and print it — or, alternately, using an in-office desktop scanner with a 3D printer.1,20 As previously noted, the latter workflow will be described here. Either way, even if the practice does not have an in-office 3D printer, it is still beneficial and time efficient to be able to visualize the planning, designing, and modification of the appliance by the lab prior to its fabrication.
the interocclusal record.
CASE PRESENTATION
This case presentation involves the fabrication of an occlusal guard for a patient complaining of “grinding at night and sore jaw muscles” on waking and at the end of the day. His spouse confirmed this nocturnal grinding. Upon examination, the patient had an intact dentition, with the exception of missing tooth #18. In addition, tooth #17 was mesially drifted. The restorations and crowns were intact and without defects or caries. The patient had isolated areas of gingivitis associated with plaque accumulation; otherwise, there was no bleeding on probing. The exam revealed cervical abfraction lesions and areas of tooth-tooth attrition, incisal wear, and deflective contacts in lateral excursion. The patient indicated no history of orthodontic treatment. On extraoral exam, there was no limitation of opening or deviation, and no present or prior history of temporomandibular joint problems. Examination of the muscles of mastication revealed slight tenderness to palpation of the right temporalis and masseter. An orthotic appliance was recommended to reduce further wear of the dentition and establish mutually protected occlusion with the appliance in place. The use of such an appliance is also advocated prior to irreversible occlusal treatment or restorations.8,9,21
Clinical Technique
1. Diagnostic casts can be made of the maxillary and mandibular arches with a material of choice or scanned with an intraoral scanner.
2. The patient is asked to gently close with the anterior teeth on a leaf gauge or Lucia jig8,9 for 15 to 20 minutes. This will separate the posterior teeth and reduce the proprioceptive reflexes of the teeth to the neuromuscular system, thereby deactivating the mandibular elevator muscles.8,9 The use of a leaf gauge or Lucia jig can readily control the posterior interocclusal distance and create a stable position for obtaining the interocclusal record, which should approximate the thickness of the final appliance (~2 mm).
3. An interocclusal registration material of choice is used to record the centric relation.
Digital Planning Using a Scanner and CAD Software
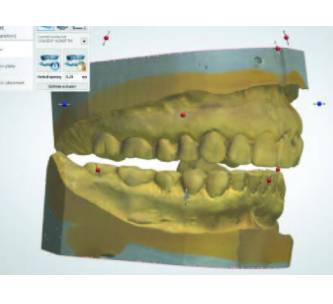
1. The diagnostic stone casts are scanned individually using a desktop scanner (assuming an intraoral scanner was not used initially; Figures 1A and 1B).
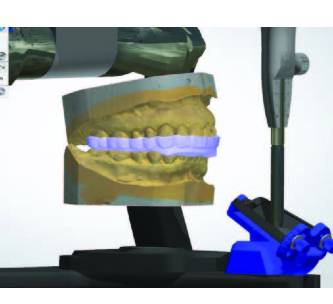
2. The casts are positioned in the interocclusal bite registration, and scanned in the articulated position (Figure 2).
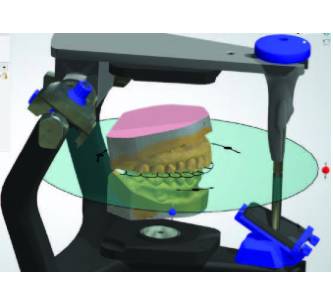
3. The maxillary cast is mounted on the virtual articulator. In order to obtain mutually protected occlusion, the incisal guide table is set in left and right lateral inclinations and protrusive inclination (Figure 3).
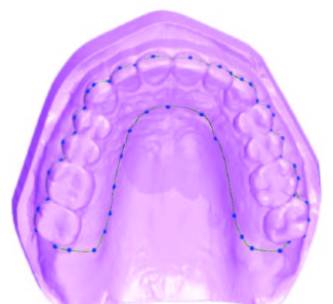
4. The path of insertion of the occlusal splint is determined. Retention and undercut/block out is established, and the boundary of the appliance is marked on the block-out model (Figure 4).
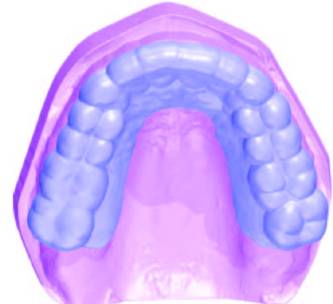
5. A shell is generated (Figure 5A). The thickness parameters are set (1.5 to 2 mm thickness). A bar is added to the occlusal surface to add thickness and begin to develop opposing occlusal contacts (Figure 5B).

6. The maxillary cast with the occlusal shell is again mounted on the articulator to the mandibular cast (preadaptive phase; Figure 6).
7. Simulated jaw movements are made on the articulator. Heavy occlusal contacts and extraneous contacts are identified on the preliminary appliance design and removed (post-adaptive phase; Figure 7).
8. The appliance is smoothed and contoured. The patient’s name can be added (Figures 8A and 8B). The data is exported as a standard tessellation language (STL) file to the 3D printer and printed using a biocompatible resin.
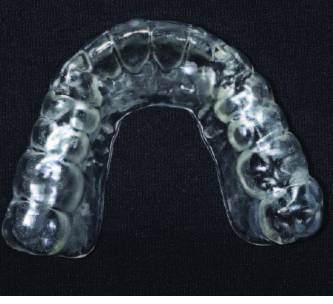
9. After printing (Figure 9A), the appliance is rinsed in isopropyl alcohol according to the manufacturer’s instructions and the printing supports are removed. The appliance is finished and polished with rotary rubber abrasives (Figures 9B and 9C).

10. The appliance is inserted and adjusted intraorally to the desired contacts, which will vary depending on the type of appliance, patient-specific needs, and occlusal philosophy of the clinician (in this case, posterior tooth centric point contacts and anterior guidance ramps to provide posterior disclussion in protrusion and lateral movement;8–10,21 Figure 10 and Figure 11).


DISCUSSION
A digital workflow for the in-office fabrication of an occlusal appliance was described using a desktop scanner and desktop 3D printer. Clinicians can also choose other types of workflows, such as using an intraoral scanner, which could eliminate the need for making impressions and the use of impression materials, trays, stone and casts, along with the need for their disinfection.22

Studies have shown the accuracy of digital versus conventional impressions to be similar;22,23 while some investigators have found greater accuracy with digital scanning,22,24–26 other studies have shown conventional impressions to be more accurate, especially for full arches.22,27–29 In addition, full-arch scanning has been shown to be more time consuming than making conventional impressions,24,29–32 and this may be a consideration in patients who have difficulty opening for long periods. The variability in scanner accuracy24,25 and technique used for scanning33 should also be considered, as some have stated that full-arch digital scanning poses a steeper learning curve.34
Intraoral scanning is a useful alternative for some impression procedures, and as digital technology continues to progress it may become more accepted — but, for now, it is not a complete replacement for all conventional impressions. Indeed, impression making is a valuable tool and skill individually developed and refined by each dentist, and one they may be less likely to give up. Clinicians have the flexibility to gradually incorporate digital workflows into their practice.
In-office 3D printers and scanners have been shown to produce high-quality occlusal appliances. Using free CAD software, Vasques et al35 found the internal fit of 3D-printed occlusal devices was better than that of conventionally fabricated devices. They also noted occlusal adjustment was similar between the groups.

APPLIANCE MATERIALS
Several materials are available for the fabrication of occlusal appliances. The most common for conventional fabrication is autopolymerizing polymethylmethacrylate (PMMA), with thermoplastic resin or vinyl polymers.8,9,10 Most occlusal devices utilizing CAD/CAM technology have involved 3D printing (as opposed to milling);20,35–37 however, there is sparse information regarding the exact composition of the proprietary ingredients, or their physical properties for either fabrication technique (printed or milled). Reyes-Sevilla et al37 compared the wear rates of conventional splint materials and CAD/CAM-fabricated splint materials, and found less wear with printed PMMA and polyamide resins materials than conventional PMMA or milled PMMA. This is in contrast to Lutz et al,36 who found milled PMMA had higher wear resistance and fracture resistance than 3D printed or conventional PMMA. Prpic et al38 evaluated conventional PMMAs, milled PMMA, milled polyamide resin, and 3D-printed nonacrylic light-polymerizing resin and acrylic light-polymerizing resin. They found PMMA resins had the most consistent hardness values, regardless of fabrication technique. Printed resins had lower surface hardness, but higher flexural strength than other PMMAs. It should be noted that all materials tested met International Organization for Standardization requirements for flexural strength. Prpic et al’s38 research found the mechanical properties of occlusal devices depended more on the material than the particular fabrication process.

The clinical implication of these new materials is not yet clear. New products suitable for dental 3D printing must be tested and submitted to the U.S. Food and Drug Administration for approval. From a clinical perspective, providers must understand a material’s physical properties when selecting a material, appliance design and fabrication method. This will allow the dentist to choose an occlusal splint material according to the patient’s specific needs. For example, flexibility is important for absorbing energy, as when a patient drops an appliance or for use as an athletic mouthguard. By comparison, a material with greater wear resistance may be a better option for a patient who bruxes.

markings.
CONCLUDING THOUGHTS
Once the clinician masters the digital workflow, designing occlusal appliances using CAD/CAM technologies can be a relatively straightforward process. Advantages include the need for limited laboratory skills, reproducibility, shorter fabrication time, and the ability to store the data and reprint additional appliances for the patient.
Even if the practitioner uses a laboratory for the design and fabrication steps, digital technologies can still be an efficient way of communicating with the lab and ensuring a timely workflow. Compared to traditional fabrication methods, 3D-printed appliances may be more precise due to fewer accumulated conventional steps and associated processing errors. In addition, the ability to communicate electronically can reduce or prevent lab delays or the need for remakes due to miscommunicated laboratory instructions. As noted, the ability to save files and data is of great benefit should the device ever need to be redesigned or replaced.
It is anticipated that as the technology advances, costs will come down and tools such as 3D printing will bring quick, affordable treatment options for the in-office fabrication of many types of occlusal appliances.
KEY TAKEAWAYS
- In-office three-dimensional (3D) printers and scanners have been shown to produce high-quality occlusal appliances.
- The digital workflow described here uses an optical scanner to capture the anatomy, computer aided design software to design the occlusal guard, and a computer aided manufacturing system to mill or print the appliance.1–6
- This can be a completely digital process, although a combination digital/analog approach (using some conventional techniques) is also possible.
- The advantages of 3D-printed occlusal splints include the need for limited laboratory skills, reproducibility, shorter fabrication time, and the ability to store the data and reprint additional appliances for the patient.
REFERENCES
- Banner LC, Aquino E, Bishop R, Dominici JT. Desktop 3D printing in mandibular reconstruction. Decisions in Dentistry. 2018;4(3):10–14.
- Patel N, Fratianne MA. Sterilthography: the future of dental fabrication. Decisions in Dentistry. 2017;3(11):18–22.
- Torabi, K, Farjood E, Hamedani S. Rapid prototyping technology and their applications in prosthodontics, a review of literatureJ J Dent (Shiraz). 2015;16:1–9.
- Abduo J, Lyons K, Bennamoun M. Trends in computer-aided manufacturing in prosthodontics: a review of the available systems. Int J Dent. 2014:783948.
- Oberoi G, Nitsch S, Edelmayer M, Janjić K, Müller AS, Agis H. 3D printing-encompassing the facets of dentistry. Front Bioeng Biotechnol. 2018;6:172.
- Dawood A, Marti B, Sauret-Jackson V, Darwood A. 3D printing in dentistry. Brit Dent J. 2015;219:521–529.
- Glossary of Prosthodontic Terms GPT-9. Available at: http/://www.academyofprosthodontics.org__Library/ap_articles_download/GPT9.pdf. Accessed April 2, 2020.
- Dawson PE. Functional Occlusion From TMJ to Smile Design. Mosby Elsevier; St Louis: 2007.
- Okeson JP. Management of Temporomandibular Disorders and Occlusion. 8th ed. Mosby Elsevier; St Louis: 2019.
- Racich MJ. Occlusion, temporomandibular disorder, and orofacial pain: an evidence-based overview and update with recommendations. J Prosthet Dent. 2018;120:678–685.
- Klassner GD, Green CS, Lavigne GJ. Oral appliances and the management of sleep bruxism in adults: a century of clinical applications and search for mechanisms. Int J Prosthodont. 2010;23:453–462.
- Strom D, Behrenth E, Ekman K, Unell L, Carlsson GE. Management of tinnitus and jaw-muscle tenderness using an intraoral appliance and acupuncture. Swed Dent J. 2013;37:105–110.
- Turp JC, Komine F, Hugger A. Efficacy of stabilization splints for the management of patients with masticatory muscle pain: a qualitative systematic review. Clin Oral Invest. 2004;8:179–195.
- Daif ET. Correlation of splint therapy outcome with the electromyography of masticatory muscles in temporomandibular disorder with myofascial pain. Acta Ododontol Scan. 2012;70:72–77.
- Lavigne GJ, Herrero Babiloni A, Beetz G, et al. Critical issue in dental and medical management of obstructive sleep apnea. J Dent Res. 2020;99:26–35.
- Jacobowitz O. Advances in oral appliances for obstructive sleep apnea. Adv Otorhinolaryngol. 2017;80:57–65.
- Serra-Negra JM, Lobbezoo F, Correa-Faria P, et al. Relationship of self-reported sleep bruxism and awake bruxism with chronotype profiles in Italian dental students. Cranio. 2019;37:147–152.
- Senaratna CV, Perret JL, Lodge CJ, et al. Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med Rev. 2017:34:70–81.
- American Dental Association Council of Access Prevention and Interprofessional Relations, ADA Council on Scientific Affairs. Using mouthguards to reduce the incidence and severity of sports related oral injuries. J Am Dent Assoc. 2006;137:1712–1720.
- Lauren M, McIntyre F. A new computer-assisted method for design and fabrication of occlusal splints. Am J Orthod Dentofacial Orthop. 2008;133(Suppl 4):S130–S135.
- Solow RA. Customized anterior guidance for occlusal devices. J Prosthet Dent. 2013;110:259–263.
- Sawase T, Kuroshima S. The current clinical relevancy of intraoral scanners in implant dentistry. Dent Mater J. 2020;39:57–61.
- Ender A, Zimmermann M, Mehl A. Accuracy of complete- and partial-arch impressions of actual intraoral scanning times in vitro. Int J Comput Dent. 2019;22:11–19.
- Wesemann C, Muallah J, Mah J, Bumann A. Accuracy and efficiency of full-arch digitalization and 3D printing: a comparison between desktop model scanner, an intraoral scanner, a CBCT model scan, and stereolithographic 3D printing. Quintessence Int. 2017;48:41–50.
- Amin S, Weber HP, Finkelman M, El Rafie K, Kudara Y, Papaspyridakos P. Digital vs. conventional full-arch implant impressions: a comparative study. Clin Oral Implant Res. 2017;28:1360–1367.
- Zimmermann M, Koller C, Rumetsch M, Ender A, Mehl A. Precision of guided scanning procedures for full-arch digital impression in vivo. J Orofac Orthop. 2017;78:466–471.
- Ender A, Mehl A. In-vitro evaluation of the accuracy of conventional and digital methods of obtaining full-arch dental impression. Quintessence Int. 2015;46:9–17.
- Choi JW, Ahn JJ, Son K, Huh JB. Three-dimensional evaluation on accuracy of conventional and milled gypsum models and 3D printed photopolymer models. Materials (Basel). 2019;12:e3499.
- Grunheid T, McCarthy SD, Larson BE. Clinical use of a direct chairside oral scanner: an assessment of accuracy, time, and patient acceptance. Am J Orthod Dentofacial Orthop. 2014;146:673–682.
- Sivaramakrishnan G, Alsobaiei M, Sridharan K. Patient preference and operating time for digital versus conventional impressions: a network meta-analysis. Aust Dent J. 2020;65:58–69.
- Benic GI, Mühlemann S, Fehmer V, Hämmerle CH, Sailer I. Randomized controlled within-subject evaluation of digital and conventional work-flows for the fabrication of lithium disilicate single crowns. Part I: digital versus conventional unilateral impressions. J Prosthet Dent. 2016;116:777–782.
- Sailer I, Muhlemann S, Fehmer V, Hammerle CH, Benic GI. Randomized controlled clinical trial of digital and conventional workflows for the fabrication of zirconia-ceramic fixed partial dentures. Part I: Time efficiency of complete-arch digital scans versus conventional impressions. J Prosthet Dent. 2019;121:69–75.
- Favero R, Volpato A, Francesco M, Fiore AD, Guazzo R, Favero L. Accuracy of 3D digital modeling of dental arches. Dental Press J Orthod. 2019;24:38e1–37e7.
- Fasbinder DJ, Sterlitz SJ. Practical considerations for digital dentistry. Decisions in Dentistry. 2017;3(9):14–21.
- Vasques MT, Mori M, Laganá DC. Three-dimensional printing of occlusal devices for temporomandibular disorders by using a free CAD software program: A technical report. J Prosthet Dent. 2020;123:232–235.
- Lutz AN, Hamper R, Roos M, Lümkemann N, Eichberger M, Stawarczyk B. Fracture resistance and 2-body wear of 3-dimensional-printed occlusal devices. J Prosthet Dent. 2019;121:166–172.
- Reyes-Sevilla M, Kuijs RH, Werner A, Kleverlaan CJ, Lobbezoo F. Comparison of wear between occlusal splint materials and resin composite materials. J Oral Rehab. 2018;45:539–544.
- Prpic V, Slacanin I, Schauperl Z, Catic A, Dulcic N, Cimic S. A study of the flexural strength and surface hardness of different materials and technologies for occlusal device fabrication. J Prosthet Dent. 2019;121:955–959.
The opinions or assertions expressed in the article are those of the authors and are not to be construed as official policy or the position of the Department of Veterans Affairs or U.S. Government.
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. May 2020;6(5):14–17.
