
 NIMH (IMAGE SOURCE):, PUBLIC DOMAIN, HTTPS:/ /
COMMONS.WIKIMEDIA.ORG/ W/ INDEX.PHP?CURID=47201480
NIMH (IMAGE SOURCE):, PUBLIC DOMAIN, HTTPS:/ /
COMMONS.WIKIMEDIA.ORG/ W/ INDEX.PHP?CURID=47201480
Oral Healthcare for Patients With Schizophrenia
Dental teams well versed in schizophrenia are best positioned to manage the oral health complications of this disorder.
PURCHASE COURSE
This course was published in the May 2020 issue and expires May 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the May 2020 issue and expires May 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the prevalence, phases and complications — including oral complications — of schizophrenia.
- Explain oral healthcare considerations when treating this patient population.
- Describe the documentation and interprofessional collaboration needed when treating patients with schizophrenia.
Schizophrenia was first recognized in 1896 by the German psychiatrist Emil Kraepelin, who identified a progressively worsening mental disorder as “dementia praecox.” In 1911, this condition was renamed “schizophrenia” by the Swiss psychiatrist Eugen Bleuler.1 Schizophrenia is a complex psychiatric illness that manifests through certain behavioral changes that can make adhering to treatment plans challenging. Media misrepresentations of the disorder perpetuate misunderstanding and incorrectly stigmatize it.2 The World Health Organization (WHO) asserts that discrimination against patients with schizophrenia, including rights violations, is common.3
Compared to the general population, patients with schizophrenia have higher decayed, missing and filled teeth scores, and are at increased risk of poor oral health.4 In addition, the side effects of prescribed treatment medications can adversely impact patients’ oral health. This paper will provide an overview of this complex brain disorder, covering concepts that dental professionals can utilize while caring for this patient population.
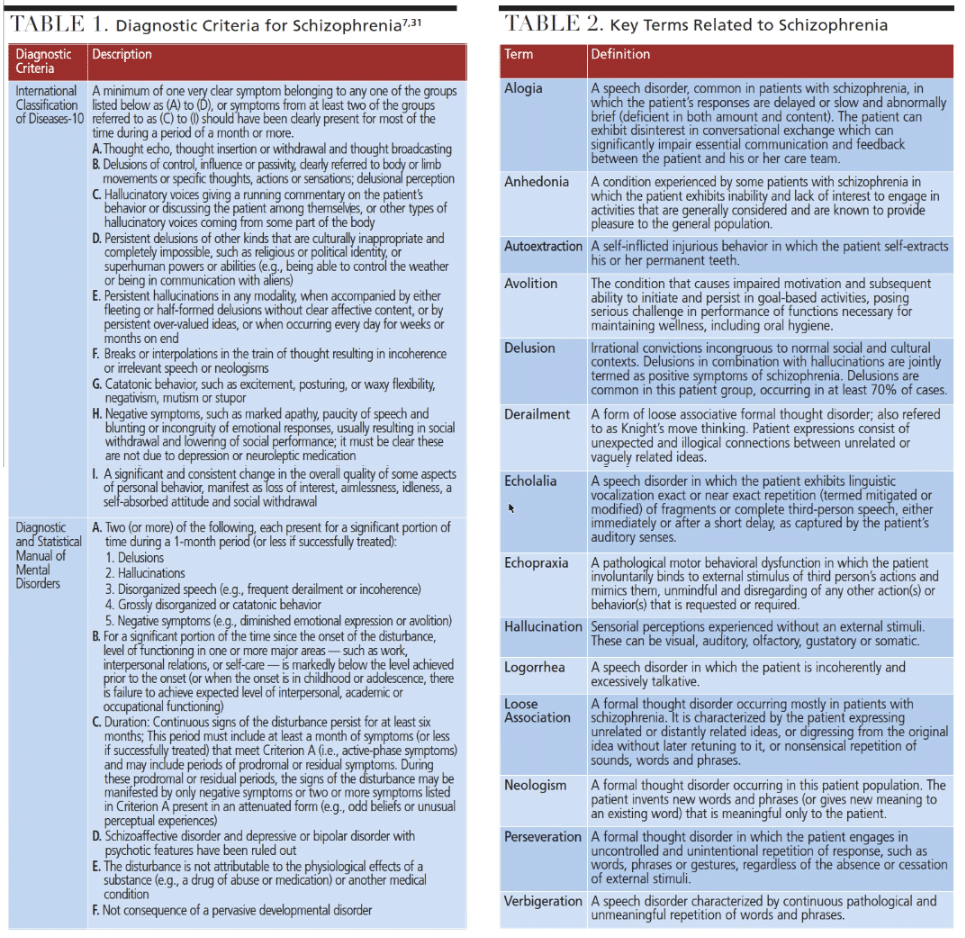
Schizophrenia is a chronic brain disorder that causes acute cognitive deficits and abnormal emotional conditions manifested in thought, speech, and behavioral complications. In turn, these contribute to social and occupational dysfunctions that impair the ability to live autonomously.2,5,6 The International Classification of Disease Version 10 describes schizophrenia as “fundamental and characteristic distortions of thinking, perception and affects that are inappropriate or blunted.”7
The prevalence of schizophrenia in the United States is estimated at 1% to 1.5%.5 The economic burden of this disorder in the U.S. is steadily trending upward: $32.5 billion in 1990,8 $62.7 billion in 2002,9 and $155.7 billion in 2013.10
With an overall weighted life expectancy of 64.7 years, patients with schizophrenia have a shorter life expectancy than the general population.11–13 This disorder occurs 1.4 times more often in men than women,14,15 and life expectancy is 8 years shorter for men, with a mean age of 59.9 at death, compared to age 67.6 for women.16
Although there is no specific age for onset, schizophrenia can occur as early as 5 years of age. Generally, onset is between ages 10 to 25 for men, and ages 25 to 35 for women.17
Mortality risk among patients with schizophrenia is two to three times higher than the general population.15 This increased mortality risk is multifactorial, and exacerbated by comorbidities. Some of the key causes of death among these patients include cardiovascular disease,12 respiratory diseases,12 suicide18 and substance abuse.12
ETIOLOGY, RISK FACTORS AND DIAGNOSIS
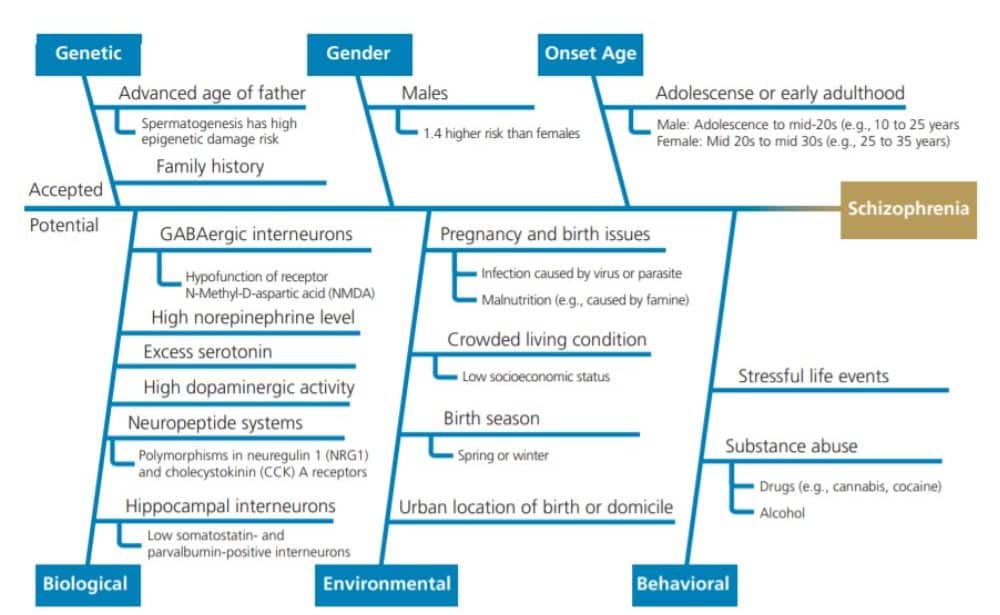
The etiology and pathophysiology of schizophrenia are not known.19,20 However, several risk factors have been identified, and there is consensus that one or more factors in combination can contribute to its onset. Figure 1 summarizes accepted and potential risk factors for schizophrenia, including genetics, gender, biological, environmental and behavioral considerations.14,18,19,21–30
A diagnosis of schizophrenia is generally made using criteria defined in either the American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders31 or WHO’s International Statistical Classification of Diseases and Related Health Problems.7 Table 1 lists the diagnostic criteria, while Table 2 explains key terms.
Although onset, severity, duration and type of schizophrenia vary, generally, the disorder manifests in three phases — prodrome, active and residual — preceded by a premorbid phase.32 Other than slight indications of social, cognitive or behavioral deficits (with possible minor physical anomalies), there are no clear signs of schizophrenia in the premorbid phase. In the prodromal phase, although criteria for clinical diagnosis are unmet, there are manifestations of negative symptoms, along with the emergence of positive symptoms. Clinical diagnosis is the onset of the disorder’s acute phase, which can include behavioral complications. Patients who enter the residual phase — typically during adulthood and between middle and old age — see discernable reduction of positive and negative symptoms, as well as cognitive and social impairments — but relapses can occur. Behavioral issues can persist even in this phase.
Patients with schizophrenia in the acute and residual phases typically exhibit behaviors categorized into positive and negative symptoms. Positive symptoms are exhibitions of psychological expressions that have no factual basis (e.g., delusions or hallucinations), formal thought disorders (e.g., loose association or derailment, neologisms or perseveration), speech anomalies (e.g., logorrhea, verbigeration or echolalia), and abnormal behavior (e.g., echopraxia).6,21,33 Negative symptoms are psychological and behavioral deficits exhibited by a person with schizophrenia. Examples include alogia (poverty of speech), avolition (loss of desire), social withdrawal, flat or blunted affect, and anhedonia (inability to feel pleasure).6,21,33 The disorder’s complexity is borne out by the extensive and varying array of associative behavioral and emotional complications, coupled with a variable set of cognitive impairments.
Behavioral complications are not consistent across patients, and can include one or more of the following: smoking, parafunctional habits, self-injurious behavior, poor dietary habits, deliberate foreign body ingestion, low physical activity, social withdrawal, lack of motivation for oral care, and substance abuse.4,14,33,34
Associated emotional disorders experienced by patients with schizophrenia are varied, and the set of typical disorders includes anxiety, depression and suicidal tendencies — with anxiety and depression being quite common.35 The prevalence of suicidal tendencies is also high among these patients — and suicide is one of the most frequent causes of death.19 Commonly, social withdrawal adversely impacts communication between patients and their families and care team.
Cognitive deficits result in disorganized thought, an inability to maintain attention and focus, speech disorders (e.g., loose associations, neologisms, perseveration and clang association), and deficiencies in comprehension and recall of verbal communications. They may also compromise executive functions, such as logical understanding, deduction and problem resolution.36,37 Patients with schizophrenia have diminished motivation to maintain or improve oral health, identify health issues, and logically deduce solutions. The severity of the impairment is negatively related to oral health, treatment compliance and outcomes.
PHARMACOLOGICAL TREATMENT
Pharmacological treatment of schizophrenia primarily relies on first-generation antipsychotics (FGA) and second-generation antipsychotics (SGA) to control positive symptoms. Common FGAs include chlorpromazine, thioridazine, perphenazine, fluphenazine, haloperidol, thiothixene and trifluoperazine.38 Commonly prescribed SGAs include aripiprazole, clozapine, olanzapine, quetiapine, risperidone and ziprasidone.38 Both FGAs and SGAs cause xerostomia and hyposalivation — side effects that are also caused by tricyclic antidepressants and mood-stabilizing drugs (e.g., carbamazepine and valproate) prescribed as part of the treatment.39 Dry mouth conditions may produce halitosis. They may also increase risk for caries and other oral lesions (e.g., candidiasis, glossitis or generalized stomatitis), and create difficulty eating, swallowing and speaking.
The antipsychotics can cause pseudoparkinsonism (tremors and rigidity in arms), which is reversible when drugs are stopped, but long-term use can cause irreversible tardive dyskinesia (involuntary movements in the orofacial area)33 — either of which can make oral self-care challenging, even for the motivated patient. These drugs can also induce serious blood disorders, such as leukopenia, agranulocytosis and thrombocytopenia.39 When any of these blood abnormalities occur, dental procedures should only be initiated after verifying that normal levels, either for white blood cells or platelets, are restored.
ORAL CARE FOR PATIENTS WITH SCHIZOPHRENIA
Oral care treatments are dependent on the state of the patient’s disorder — and, to this end, an understanding and application of the phases of schizophrenia development will prove clinically useful.
Assessment — Oral health professionals should review the patient’s complete medical history and perform an oral examination. For patients clinically diagnosed with schizophrenia, the provider should note prescribed medications, allergies, contraindications, concurrent medical conditions, comorbidities, and recorded behavioral, emotional and cognitive impairments. The oral examination must take into account the potential for oral conditions from medication side effects, blood studies, factors affecting oral hygiene self-care (such as impaired physical abilities and lack of motivation), and self-injurious behaviors, such as autoextractions. The clinician should consult the patient’s primary care physician and other healthcare providers, as required to obtain necessary information and clarifications to complete the assessment.
Diagnosis — Based on the data collected during assessment, the provider determines the patient’s oral health status, which might include xerostomia, periodontitis, caries and other oral lesions. The diagnostic report should note any condition that can impact treatment, such as physical impairments, behavioral issues, emotional issues (such as anxiety), and cognitive dysfunctions.
Planning — The diagnostic statement should assist in creating a treatment plan involving therapeutic and preventive therapies, as well as identifying oral health education targets. For example, with xerostomia the treatment approach should be based on cause and severity. When managing caries, an evidence-based approach — such as Caries Management by Risk Assessment40 — should be incorporated in the treatment plan.
The effectiveness of therapeutic interventions will depend on appropriate, patient-centered oral health education designed to ensure self-care and other preventive measures are consistently applied. In instances in which a patient has severe impairments (e.g., physical, behavioral, emotional and/or cognitive), it is prudent to include the patient’s family, caregiver and support team to ensure compliance with oral health recommendations. In addition, educational strategies should include mitigation measures for known, patient-specific risks, such as self-injurious behavior. Furthermore, in cases in which there are known risks, such as aggressive behavior, suicidal tendencies or anxiety disorders, the treatment plan should address eliminating potential triggers, reducing anxiety, and removing instruments or devices that could cause harm. Dental providers should also make sure the office has an emergency protocol in place, as well as immediate access to the patient’s support and care teams’ contact information.
Implementation — In addition to implementing treatment and self-care plans that might include nonsurgical periodontal therapy and fluoride therapy (such as varnish, silver diamine fluoride or at-home prescription fluoride, depending on case presentation and need), dental teams should continue to monitor the patient’s medical history and vital signs. The goal is to ensure treatment plans align with the patient’s present condition.
Vigilance is necessary during procedures to quickly detect and manage potentially life-threatening responses (such as an abnormal gag reflex) to ensure the airway is protected. Relapses during the residual phase are not uncommon due to nonadherence with treatment regimens; therefore, regular monitoring of the medical history and tracking prescribed medications — along with side effects — is advised. For example, certain antipsychotic medications, such as clozapine, reduce the white blood cell (WBC) count by suppressing bone marrow function. This can preclude dental care until the WBC count is restored to normal limits. When current medication history includes clozapine, oral health professionals should contact the patient’s physician to ascertain the WBC count is within normal limits before initiating treatment.
Evaluation — Dental teams should monitor the patient’s progress during office visits and obtain updates from other healthcare providers (if deemed necessary) to ensure evaluation is based on current information. Reevaluation appointments should be scheduled as appropriate to monitor the patient’s oral health status and engage the patient in maintaining motivation and improving self-care techniques.
Documentation — Oral health professionals should ensure all documents are current, including medical and dental histories, oral assessment reports, diagnostic reports, oral care plans, evaluation statements, and emergency response plans. In addition, patient consent forms, disclosures and contact information (for all care team members) should be kept current. These written representations ensure that all oral health team members, including the patient, understand the diagnoses, care provided, and outcomes.
CONCLUSION
Providing oral care for patients with schizophrenia can be challenging because the disorder can prevent the patient from mindful participation in his or her oral care. These challenges can be further compounded by the presence of motor, cognitive, social and behavioral impairments. Understanding this disorder and its oral implications can help dental teams ensure treatment plans are individually tailored and implemented in an evidence-based fashion designed to optimize oral health outcomes.
REFERENCES
- Countries IoMCoNSDiD. In: Neurological, Psychiatric, and Developmental Disorders: Meeting the Challenge in the Developing World. Washington, DC: National Academies Press (U.S.); 2001.
- Duckworth K, Halpern JH, Schutt RK, Gillespie C. Use of schizophrenia as a metaphor in U.S. newspapers. Psychiatric Services (Washington, DC). 2003;54:1402–1404.
- World Health Organization. Schizophrenia. Available at: https://www.who.int/news-room/fact-sheets/detail/schizophrenia. Accessed April 17, 2020.
- Tani H, Uchida H, Suzuki T, et al. Dental conditions in patients with schizophrenia: a large-scale multi-site survey. BMC Oral Health. 2012;12:32.
- Perry MM, Dougherty NJ. In: Patton LL, Glick M, eds. The ADA Practical Guide to Patients With Medical Conditions. 2nd ed. Hoboken, New Jersey: Wiley-Blackwell; 2016:528.
- Siever LJ, Davis KL. The pathophysiology of schizophrenia disorders: perspectives from the spectrum. Am J Psychiatry. 2004;161:398–413.
- World Health Organization. Schizophrenia, Schizotypal and Delusional Disorders (F20-F29). In: International Statistical Classification of Diseases and Related Health Problems. Available at: https://apps.who.int/classifications/apps/icd/icd10online2003/fr-icd.htm?gf20.htm+. Accessed April 17, 2020.
- Rice DP. The economic impact of schizophrenia. J Clin Psychiatry. 1999;60(Suppl 1):4–6; discussion 28–30.
- Wu EQ, Birnbaum HG, Shi L, et al. The economic burden of schizophrenia in the United States in 2002. J Clin Psychiatry. 2005;66:1122–1129.
- Cloutier M, Aigbogun MS, Guerin A, et al. The economic burden of schizophrenia in the United States in 2013. J Clin Psychiatry. 2016;77:764–771.
- Olfson M, Gerhard T, Huang C, Crystal S, Stroup TS. Premature mortality among adults with schizophrenia in the United States. JAMA Psychiatry. 2015;72:1172–1181.
- HjorthoJ C, Sturup AE, McGrath JJ, Nordentoft M. Years of potential life lost and life expectancy in schizophrenia: a systematic review and meta-analysis. Lancet Psychiatry. 2017;4:295–301.
- Laursen TM, Nordentoft M, Mortensen PB. Excess early mortality in schizophrenia. Annu Rev Clin Psychol. 2014;10:425–448.
- Abel KM, Drake R, Goldstein JM. Sex differences in schizophrenia. Int Rev Psychiatry. 2010;22:417–428.
- McGrath JJ, Susser ES. New directions in the epidemiology of schizophrenia. Med J Aust. 2009;190(Suppl 4):S7–S9.
- Galletly CA. Premature death in schizophrenia: bridging the gap. Lancet Psychiatry. 2017;4:263–265.
- Rajji TK, Ismail Z, Mulsant BH. Age at onset and cognition in schizophrenia: meta-analysis. Br J Psychiatry. 2009;195:286–293.
- National Institute of Mental Health. Schizophrenia. Available at: https://www.nimh.nih.gov/health/statistics/schizophrenia.shtml. Accessed Apil 17, 2020.
- Yolken RH, Torrey EF. Viruses, schizophrenia, and bipolar disorder. Clin Microbiol Rev. 1995;8:131–145.
- Boos HB, Postma HD, Cahn W. Neurotoxicity and Schizophrenia. In: Stolerman IP, Price LH, eds. Encyclopedia of Psychopharmacology. 2nd ed. New York, New York: Springer; 2015:7.
- Andreasen NC, Flaum M, Swayze VW II, Tyrrell G, Arndt S. Positive and negative symptoms in schizophrenia. A critical reappraisal. Arch Gen Psychiatry. 1990;47:615–621.
- Boyd JH, Pulver AE, Stewart W. Season of birth: schizophrenia and bipolar disorder. Schizophr Bull. 1986;12:173–186.
- Caceda R, Kinkead B, Nemeroff CB. Involvement of neuropeptide systems in schizophrenia: human studies. Int Rev Neurobiol. 2007;78:327–376.
- Coyle JT. Glutamate and schizophrenia: beyond the dopamine hypothesis. Cell Mol Neurobiol. 2006;26:365–384.
- Eggers AE. A serotonin hypothesis of schizophrenia. Med Hypotheses. 2013;80:791–794.
- Ek M, Wicks S, Svensson AC, Idring S, Dalman C. Advancing paternal age and schizophrenia: the impact of delayed fatherhood. Schizophr Bull. 2015;41:708–714.
- Kesby JP, Eyles DW, McGrath JJ, Scott JG. Dopamine, psychosis and schizophrenia: the widening gap between basic and clinical neuroscience. Transl Psychiatry. 2018;8:30.
- Konradi C, Yang CK, Zimmerman EI, et al. Hippocampal interneurons are abnormal in schizophrenia. Schizophr Res. 2011;131:165–173.
- Torrey EF, Yolken RH. Toxoplasma gondii and schizophrenia. Emerg Infect Dis. 2003;9:1375–1380.
- van Kammen DP, Peters J, Yao J, et al. Norepinephrine in acute exacerbations of chronic schizophrenia: negative symptoms revisited. Arch Gen Psychiatry. 1990;47:161–168.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatry Association Publishing; 2013.
- Lieberman JA, Perkins D, Belger A, et al. The early stages of schizophrenia: speculations on pathogenesis, pathophysiology, and therapeutic approaches. Biol Psychiatry. 2001;50:884–897.
- Gupta S, Pk P, Gupta R. Necessity of oral health intervention in schizophrenic patients — A review. Nepal J Epidemiol. 2016;6:605–612.
- Frankel F, Simmons JQ. Self-injurious behavior in schizophrenic and retarded children. Am J Mental Deficiency. 1976;80:512–522.
- Buckley PF, Miller BJ, Lehrer DS, Castle DJ. Psychiatric comorbidities and schizophrenia. Schizophr Bull. 2008;35:383–402.
- Bowie CR, Harvey PD. Cognitive deficits and functional outcome in schizophrenia. Neuropsychiatr Dis Treat. 2006;2:531–536.
- Diamond A. Executive functions. Annu Rev Psychol. 2013;64:135–168.
- Muench J, Hamer AM. Adverse effects of antipsychotic medications. Am Fam Physician. 2010;81:617–622.
- Little J, Miller C, Rhodus N. Little and Falace’s Dental Management of the Medically Compromised Patient. 9th ed. Maryland Heights, Mo: Mosby; 2017.
- Maheswari SU, Raja J, Kumar A, Seelan RG. Caries management by risk assessment: A review on current strategies for caries prevention and management. J Pharm Bioallied Sci. 2015;7(Suppl 2):S320–S324.
From Decisions in Dentistry. May 2020;6(5):40–44.

