

Dental Management of Medication-Related Osteonecrosis of the Jaw
While rare, this pathology has devastating effects on patient health and quality of life
PURCHASE COURSE
This course was published in the September 2023 issue and expires September 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the September 2023 issue and expires September 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 730
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the causes of and risk factors for medication-related
osteonecrosis of the jaw (MRONJ). - Identify the stages of MRONJ.
- List the prevention strategies for this oral pathology.
Medication-related osteonecrosis of the jaw (MRONJ) is a devastating pathology that occurs in a small fraction of patients taking antiresorptive or antiangiogenic drugs for the treatment of certain bone pathologies. It’s not completely understood why MRONJ develops.
MRONJ is relevant to dentists because it appears in the jaws and maxillofacial region. Necrotic bone of the oral-facial area can drastically alter a patient’s quality of life by causing tooth loss, paresthesia, infection, swelling, and pain.1 Ultimately, the best option for patients at risk for MRONJ is prevention. However, this is not always possible due to the urgency of medical treatment or lapses in dental care.
Causes and Risk Factors
The nomenclature to describe MRONJ has evolved as new information about the disease becomes available. The first MRONJ cases were described in 2003 when surgeons identified 36 people with treatment-resistant exposed bone in their jaws accompanied by pain. This was described as pamidronate- and zoledronate-induced avascular necrosis of the jaw.2
Then bisphosphonate-related osteonecrosis of the jaw described this condition until newer, nonbisphosphonate medications were implicated, resulting in MRONJ as the currently accepted term.3 According to the American Association of Oral and Maxillofacial (AAOMS), a MRONJ diagnosis involves clinical presentation and pharmacological history, and must fulfill all three of the following criteria:4
- Current or previous treatment with antiresorptive therapy alone or in combination with immune modulators or antiangiogenic medications.
- Exposed bone or bone that can be probed through an intraoral or extraoral fistula(e) in the maxillofacial region that has persisted for more than 8 weeks.
- No history of radiation therapy to the jaws or metastatic disease to the jaws.
Antiresorptive medications inhibit osteoclast activity, causing decreased bone resorption.5 Traditionally, bisphosphonates have been implicated in MRONJ. They are used to treat or prevent osteopenia, osteoporosis, hypercalcemia, and metastatic bone disease.4,6
Bisphosphonates are divided into nitrogen-containing bisphosphonates (NBPs) and nonNBPs, which have different mechanisms of action. NBPs contain a nitrogen moiety in their molecular structure, rendering them more potent than nonNBPs.6 Consequently, NBPs also have a higher risk of inducing MRONJ.6
In 2009, the United States Food and Drug Administration approved the monoclonal antibody denosumab for the treatment of osteoporosis, bone metastasis, and giant cell tumors.7 Denosumab inhibits osteoclast recruitment and action.8,9 In 2019, another monoclonal antibody, romosozumab, was approved for osteoporosis treatment, as it decreases vertebral fracture risk. This drug enhances bone formation and reduces bone resorption. Cases of MRONJ were reported in the romosozumab registration trial, though the real-world incidence is not known.10
Angiogenesis is required for tumor development and cancer progression.11 Antiangiogenic drugs, used in cancer treatment, block the angiogenesis signaling cascade and prevent new blood vessel formation.11 Osteonecrosis is classically associated with decreased blood flow to the affected bone, and the function of these medications likely contributes to MRONJ. These drugs are broadly divided into tyrosine kinase inhibitors (TKIs) and monoclonal antibodies.11,12
TKIs, such as sunitinib and sorafenib, inhibit phosphorylation of receptors involved with vascular endothelial growth factor receptor (VEGFR) and platelet-derived growth factor receptor.11 Monoclonal antibodies, including bevacizumab, target VEGFR or VEGFR2.11 More MRONJ cases are associated with the use of antiresorptive drugs, with a smaller number resulting from antiangiogenic medications.13,14 However, there is a current literature gap on antiangiogenic medications in MRONJ development.
MRONJ incidences vary depending on the indication for treatment. When antiresorptive or antiangiogenic medications are used for cancer therapy, drug doses tend to be higher. These drugs are prescribed in the treatment of breast, prostate, multiple myeloma, and other cancers. When these medications are used to treat nonmalignant diseases, the doses are lower and reflect a decreased MRONJ risk.
Osteoporosis is the most common nonmalignant condition that poses a risk for MRONJ. However, other at-risk nonmalignant diseases are osteogenesis imperfecta, chronic kidney disease, and Paget disease. The cumulative dose is the duration and frequency of drug administration, and a higher cumulative dose corresponds to a higher MRONJ risk, which is why it is necessary to know how long a patient has been on drug therapy.15 Additionally, intravenous administration of antiresorptive medications shows increased MRONJ prevalence and severity compared to oral intake.9
Although incidences of patients spontaneously developing MRONJ after taking antiresorptive or antiangiogenic medications have been reported, MRONJ is rare; most cases develop after a dental event.16 Extractions are the number one dental risk factor for MRONJ and, for this reason, clinicians need to be aware of all possible oral issues that may necessitate tooth removal, including trauma, vertical root fracture, periodontal diseases, and caries.
Interestingly, the area that a tooth is extracted from is significant — posterior tooth extractions are six times more likely to cause MRONJ compared to anterior extractions.17 Additionally, MRONJ is more prevalent in the mandible (75%), than in the maxilla (25%); however 4.5% of patients experience MRONJ in both jaws.4
Periodontal diseases are another significant risk factor in the development of MRONJ, and the reason that more than 60% of teeth need extraction in patients ages 45 and older.18 Periodontal diseases are characterized by inflammation and result in catabolism of the supporting jawbone.18 Other dental comorbidities associated with MRONJ include denture trauma, implants, infection/abscess, and general poor oral health.19,20
Demographic factors show that women older than age 65 are at the highest risk, likely due to breast cancer and osteoporosis diagnoses.21 The most recent AAOMS position paper states that corticosteroid use in conjunction with antiresorptive drugs increases MRONJ risk.4 One recent cohort study showed that patients with multiple myeloma, followed by breast and prostate cancers, are at highest risk.19,20 Other studies show tobacco use and cardiovascular disease as medical comorbidities that increase MRONJ risk, although many systemic chronic conditions that influence MRONJ development are still being debated in the literature.4,19
Stages and Diagnosis
The AAOMS has staged MRONJ to reflect the progression of the disease, which informs treatment protocols.4 Stage 0 is defined by having no clinical necrotic bone. However, the patient will present with symptoms, such as dull bone pain or sinus pain, that could be accompanied by inflammation of the sinus wall. Patients might experience loose teeth not caused by chronic periodontal diseases or swelling. Radiographically, early MRONJ will have areas marked by diffuse radiopacity and possible thickening of the lamina dura. The alveolar bone of where teeth were extracted in the past will have little to no bone healing.22
Stage 1 is characterized by exposed and necrotic bone or fistula that probes to the bone in patients who are asymptomatic, without signs of infection or inflammation.4 Radiographic findings are similar to stage 0.
Stage 2 (Figure 1, page 28) presents clinically and radiographically as stage 1, but with signs of infection or inflammation.4 Stage 3 has all the same components of stage 2 and at least one additional feature such as pathological fracture or oral antral/oral-nasal communication.4
Patients should be seen for regular recare visits to catch signs of MRONJ early. The dentist should consider seeing a patient at more frequent intervals than once every 6 months, depending on individual risk factors. Dentists should also encourage patients who are experiencing new oral symptoms to contact their providers.
Most general dentists use a panoramic radiograph to aid in diagnostics. In addition to the radiographic descriptions within each MRONJ stage, some studies have shown differences in the cortical bone, which is believed to be where MRONJ originates, between MRONJ patients and control patients, and this difference then spreads to trabecular bone.23
False positives are possible when clinicians are overly reliant on radiographs.4 For this reason, dentists should consider obtaining cone-beam computed topography images when MRONJ is suspected. Additionally, magnetic resonance imaging may aid in estimating the necrotic invasion into both soft and hard tissue.5
Histologically, necrotic bone areas lack osteocytes and osteoclasts, with smaller bone pieces feeling soft due to the presence of bacteria. Usually several different types of bacteria are present that result in infection, but recent literature suggests that actinomyces, a common species in the oral flora, is present in MRONJ bone specimens.22,24 The diagnostic criteria should be used to exclude differential diagnoses of atypical neuralgia, sarcomas, temporomandibular joint disorders, odontalgia, myofascial pain, sinusitis, and fibro-osseous lesions.25
Prevention
Physicians need to discuss the risk of MRONJ with patients, particularly when other potential comorbidities are present and refer them to a dentist prior to taking the medications. The dentist should take a thorough health history and confirm all diagnoses and medications, including mode of administration and dosage.
Because medication treatments can change within a short time, the dentist must update this information at every appointment. If there are questions about the patient’s health, a written medical consultation with the appropriate physician(s) is advised. This is another opportunity to educate the patient about MRONJ risk, discuss the importance of oral hygiene, and inform the patient about the consequences of abstaining from preventive dental treatment. Providers should describe MRONJ symptoms for patients to monitor including jaw pain, erythematous gingival tissue, exposed bone, nonhealing sockets, numbness, loose teeth, a foul taste in the mouth, and swelling.26
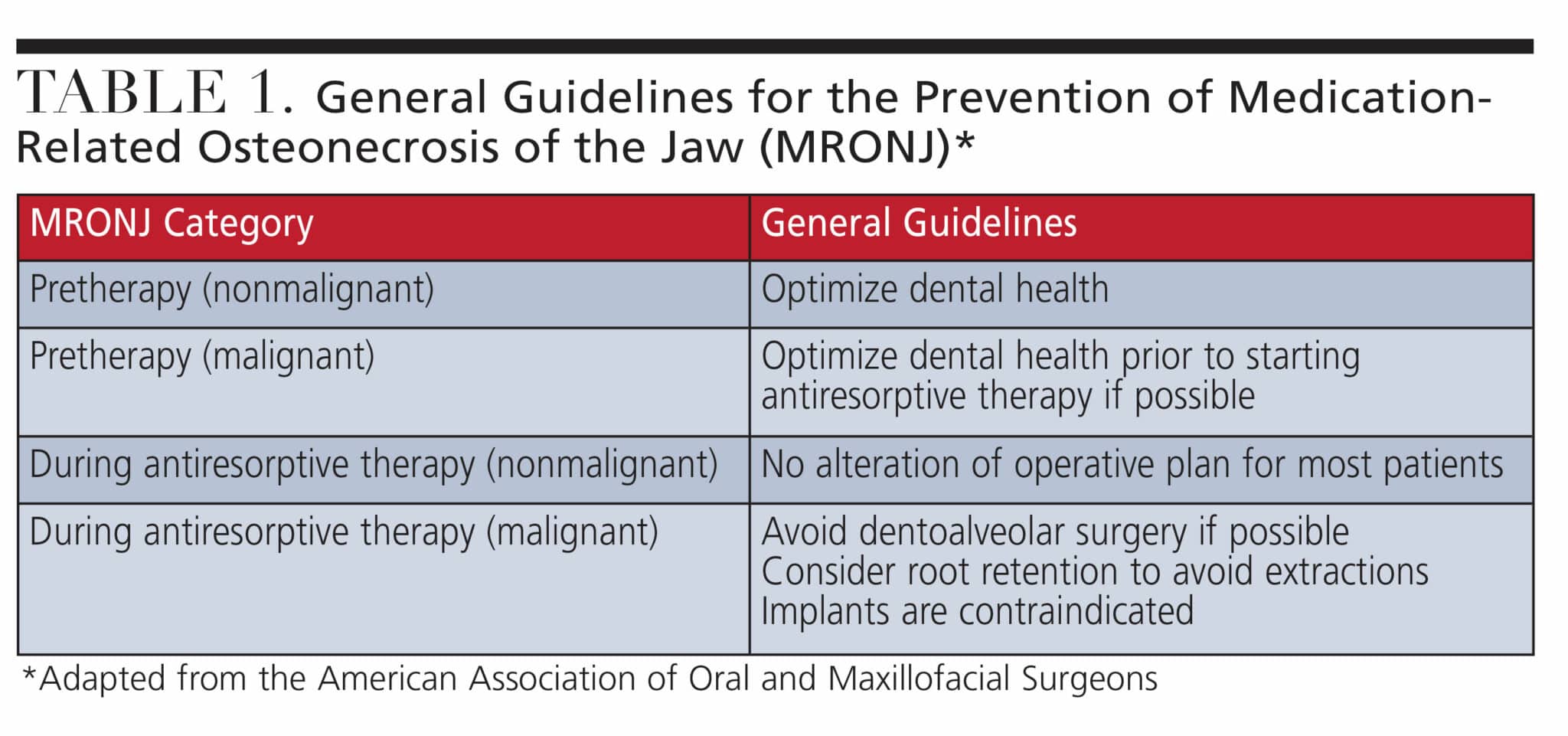 The goal of MRONJ prevention is to eliminate dental risk factors and to maintain a healthy oral environment.27 A thorough dental examination, with periodontal assessment and radiographs, should be initially completed to evaluate the patient’s current oral health and to use as a baseline reference in the future if MRONJ is suspected. Table 1 was developed by the AAOMS to provide dentists with a general guide when treating patients on antiresorptive medications.4
The goal of MRONJ prevention is to eliminate dental risk factors and to maintain a healthy oral environment.27 A thorough dental examination, with periodontal assessment and radiographs, should be initially completed to evaluate the patient’s current oral health and to use as a baseline reference in the future if MRONJ is suspected. Table 1 was developed by the AAOMS to provide dentists with a general guide when treating patients on antiresorptive medications.4
Inflammatory disease presents in 50% of MRONJ cancer patients and indicates the need to complete high-risk dental procedures before therapy when possible.4 Preoperative and post-operative antibiotics and antimicrobial rinses can also be used to minimize MRONJ risk.4
Dental treatment recommendations for patients undergoing cancer therapy are more conservative due to the higher doses prescribed. In the pre-treatment phase for both nonmalignant and cancer patients, restorative, endodontic, and periodontal treatment should be completed to stabilize the oral cavity and remove potential sources of infection.
The status of teeth with root canal therapy (RCT) should be evaluated, as MRONJ can be initiated from poorly performed RCTs. When it is suspected that a patient needs endodontic therapy, pulpal testing should be completed to obtain a proper periapical and pulpal diagnoses and to rule out MRONJ. The clinician’s skill level in performing RCT should be considered as teeth with over- or underfilled canals can lead to MRONJ.28
Dentures are another area of concern. Existing prosthetics must be examined to minimize compression on the mucosa, which could cause ulcerations, with special attention given to the posterior lingual flange where mucosal trauma is more common. Lesions within the mucosa, such as sore spots, provide a route for bacteria to reach the bone, causing inflammation.29 Denture stability should be optimized and relines in soft resins are possible when indicated. Additionally, patients must be cautioned to remove their dentures for 8 to 12 hours per day.
When a pretreatment extraction is completed, the tooth should be removed atraumatically, and osseous healing should be complete, usually requiring 4 to 6 weeks before antiresorptive medication is started.27 Every attempt to avoid extractions in patients taking high drug doses for cancer therapy should be made.
Interestingly, drug holidays are an area of debate. Some studies suggest that drug holidays decrease MRONJ risk, while others do not observe a statistical significance in MRONJ outcomes. This continues to be an active area of investigation. Patients who need high-risk extractions and patients with new MRONJ diagnoses should be referred to an oral surgeon.
MRONJ treatment decisions are dependent on the stage of progression and individual patient factors, with treatment categorized as nonoperative or operative. In conservative stage 1 therapy, antimicrobial rinses or the removal of mobile sequestrum can be used, while surgical intervention involves marginal resection of the mandible or alveolectomy in the maxilla.4
Stage 2 and 3 nonsurgical therapies include stage 1 treatments with the addition of systemic antibiotics or pain control, while surgical intervention involves mandibular segmental resection or partial infrastructure maxillectomy.4 Once a MRONJ diagnosis has been made, treatment is aimed at curing the disease and improving quality of life.
Conclusion
The past 20 years have shown considerable progress in understanding MRONJ, but research remains ongoing. Many of the recommendations in this article come from the AAOMS, but there are several international organizations with their own positions. An accurate MRONJ diagnosis relies on the dentist’s ability to combine aspects of the patient’s health history, clinical findings, and different imaging modalities.
Dentists should make sure they remain up-to-date on the best practices regarding MRONJ. Furthermore, MRONJ management is a collaborative effort of the healthcare team. Dentists must work with patients and physicians to offer individualized preventive and maintenance MRONJ strategies.
References
- Mark AM. What Is MRONJ? J Am Dent Assoc. 2021;152:710.
- Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg. 2003;61:1115-1117.
- Wang Q, Liu J, Qi S, Liao X, Liu D, Pan J. Clinical analysis of medication related osteonecrosis of the jaws: a growing severe complication in China. J Dent Sci. 2018;13:190-197.
- Ruggiero SL, Dodson TB, Aghaloo T, et al. American Association of Oral and Maxillofacial Surgeons’ Position Paper on medication-related osteonecrosis of the jaw–2022 update. Available at: aaoms.org/docs/govt_affairs/advocacy_white_papers/mronj_position_paper.pdf. Accessed August 8, 2023.
- AlDhalaan NA, BaQais A, Al-Omar A. Medication-related osteonecrosis of the jaw: a review. Cureus. 2020;12:e6944.
- Rogers MJ, Mönkkönen J, Munoz MA. Molecular mechanisms of action of bisphosphonates and new insights into their effects outside the skeleton. Bone. 2020;139:115493.
- Limones A, Sáez-Alcaide LM, Díaz-Parreño SA, Helm A, Bornstein MM, Molinero-Mourelleet P. Medication-related osteonecrosis of the jaws (MRONJ) in cancer patients treated with denosumab VS. zoledronic acid: a systematic review and meta-analysis. Med Oral Patol Oral Cir Bucal. 2020;25:e326-e336.
- Hanley DA, Adachi JD, Bell A, Brown V. Denosumab: mechanism of action and clinical outcomes. Int J Clin Pract. 2012;66:1139-1146.
- Kim HY. Review and update of the risk factors and prevention of antiresorptive-related osteonecrosis of the jaw. Endocrinol Metab (Seoul). 2021;36:917-927.
- Krupa K, Parmar M, Delo LF. Romosozumab. Treasure Island, Florida: StatPearls Publishing; 2022.
- Huang M, Lin Y, Wang C, et al. New insights into antiangiogenic therapy resistance in cancer: Mechanisms and therapeutic aspects. Drug Resist Updat. 2022;64:100849.
- American Dental Association. Oncology Agents and Medication-Related Osteonecrosis of the Jaw. Available at: ada.org/resources/research/science-and-research-institute/oral-health-topics/oncology-agents-and-medication-related-osteonecrosis-of-the-jaw. Accessed August 8, 2023.
- Sacco R, Woolley J, Patel G, Calasans-Maia MD, Yates J. Systematic review of medication related osteonecrosis of the jaw (MRONJ) in patients undergoing only antiangiogenic drug therapy: surgeror conservative therapy? Br J Oral Maxillofac Surg. 2022;60(2):e216-e230.
- Pimolbutr K, Porter S, Fedele S. Osteonecrosis of the jaw associated with antiangiogenics in antiresorptive-naïve patient: a comprehensive review of the literature. Biomed Res Int. 2018;23:8071579.
- Otto S, Aljohani S, Riham Fliefel R, et al. Infection as an important factor in medication-related osteonecrosis of the jaw (MRONJ). Medicina (Kaunas). 2021;57:463.
- Khominsky A, Lim MAWT. “Spontaneous” medication‐related osteonecrosis of the jaw; two case reports and a systematic review. Aust Dent J. 2018;63:441-454.
- Mong-Hun K, Lee DK, Kim CW, Song I, Jun SH. Clinical characteristics and recurrence-related factors of medication-related osteonecrosis of the jaw. J Korean Assoc Oral Maxillofac Surg. 2018;44:225-231.
- Kwoen MJ Park JH, Kim KS, et al. Association between periodontal disease, tooth extraction, and medication‐related osteonecrosis of the jaw in women receiving bisphosphonates: a national cohort‐based study. J Periodontol. 2023;94:98-107.
- McGowan K, McGowan T, Ivanovski S. Risk factors for medication‐related osteonecrosis of the jaws: A systematic review. Oral Dis. 2018;24:527-536.
- Van Poznak CH, Unger JM, Darke AK, et al. Association of osteonecrosis of the jaw with zoledronic acid treatment for bone metastases in patients with cancer. JAMA Oncol. 2021;7:246-254.
- AlRowis R, Aldawood A, AlOtaibi M, et al. Medication-related osteonecrosis of the jaw (mronj): a review of pathophysiology, risk factors, preventive measures and treatment strategies. Saudi Dent J. 2022;34:202-210.
- Blašković M, Blašković D. Medication-related osteonecrosis of the jaw: an overview. Available at: intechopen.com/chapters/퀵. Accessed August 8, 2023.
- Moreno-Rabié C, Gaêta-Araujo H, Oliveira-Santos C, Politis C, Jacobs R. Early imaging signs of the use of antiresorptive medication and MRONJ: a systematic review. Clin Oral Investig. 2020;24:2973-2989.
- Cerrato A, Zanette G, Boccuto M, Angelini A, Valente M, Bacci C. Actinomyces and MRONJ: a retrospective study and a literature review. J Stomatol Oral Maxillofac Surg. 2021;122:499-504.
- He L, Sun X, Liu Z, Qiu Y, Niu Y. Pathogenesis and multidisciplinary management of medication-related osteonecrosis of the jaw. Int J Oral Sci. 2020;12:30.
- Ferneini EM. Medication-related osteonecrosis of the jaw (MRONJ). J Oral Maxillofac Surg. 2021;79:1801-1802.
- Di Fede O, Panzarella V, Mauceri R, et al. The dental management of patients at risk of medication-related osteonecrosis of the jaw: new paradigm of primary prevention. Biomed Res Int. 2018;2018:2684924.
- Tempesta A, Capodiferro S, Simona Di Nanna S, et al. Medication‐related osteonecrosis of the jaw triggered by endodontic failure in oncologic patients. Oral Dis. 2022 Nov 20.
- Wick A, Bankosegger P, Otto S, et al. Risk factors associated with onset of medication-related osteonecrosis of the jaw in patients treated with denosumab. Clin Oral Investig. 2022;26:2839-2852.
From Decisions in Dentistry. September 2023; 1(8):28-31.

