
 EVGENIYA PAVLOVA / ISTOCK / GETTY IMAGES PLUS
EVGENIYA PAVLOVA / ISTOCK / GETTY IMAGES PLUS
Dental Management Considerations for Cannabis Users
Dental teams should be able to identify the signs and symptoms of use — and possible abuse — of cannabis and cannabis products.
PURCHASE COURSE
This course was published in the December 2022 issue and expires December 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the December 2022 issue and expires December 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 010
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the legal and recreational use of cannabis and cannabis
products. - Identify the signs of cannabis use and abuse in dental patients.
- Consider possible negative drug interactions in cannabis users
when administering local anesthesia or sedation.
Cannabis is a plant-based drug that has historical use dating back to 500 AD in ancient Egypt, Rome, China and India. More recently, cannabis has gained much attention, as many states have legalized cannabis products in one form or another. As of this writing, 18 states, two territories and the District of Columbia have legalized cannabis for recreational use,1 whereas 36 states and four territories have legalized cannabis for medical use.2 More recently, South Dakota voted to allow recreational use, yet final approval is pending in an ongoing legal battle. By federal law, however, cannabis is classified as an illegal Schedule I substance under the Controlled Substance Act.1 But Congress continues to inch closer to legalizing cannabis at the federal level.
As the legalization of cannabis and cannabis derivatives gains more support, oral healthcare providers are more likely to encounter patients who may have used cannabis products — including smoking or vaping marijuana — prior to dental appointments. While cannabis or marijuana use may have noticeable effects on oral health conditions, practitioners may also notice increased anxieties, paranoia and negative outcomes when administering local anesthetics containing epinephrine or providing general anesthesia.3
Marijuana is just one of many names given to the psychoactive products that originate from the female cannabis plant.4,5 Cannabis serves as an antiemetic and analgesic for the clinical user, while providing mild sedation and serving as a mood enhancer for the recreational user.5 According to the U.S. Centers for Disease Control and Prevention, cannabis is one of the most commonly used illegal drugs, with approximately 22.2 million users.4,6 As cannabis is classified as a Schedule I drug — meaning it is without an accepted medical use and exhibits a high potential for abuse — U.S. researchers are unable to study the effects of other cannabis products. In fact, previously the only federally approved source for research on cannabis was the University of Mississippi’s National Center for Natural Products Research.4,7 In 2016, the U.S. Drug Enforcement Agency updated its interpretation of the 1961 Single Convention on Narcotic Drugs and 1970 Controlled Substance Act, which opened the door for other growers to cultivate marijuana for research.
CHEMICAL COMPOUNDS FOUND IN CANNABIS
Three of the most widely known cannabis products are marijuana, cannabinoids and cannabidiol (CBD). Laboratory-derived synthetic cannabinoids — such as the U.S. Food and Drug Administration (FDA)-approved nabilone, or abusive drugs, (e.g., K2 and spice, which are not FDA approved) — are also commonly used.4 Delta-9-tetrahydrocannabinol (THC) is the most potent psychoactive component.4,5 Extracted from the flowering buds, leaves, stems and seeds of the cannabis plant, THC is the active chemical compound that is responsible for the euphoric high that most users report. The concentration of THC within the cannabis product, as well as the method of use, are correlational to the final user experience.5 The level of THC determines the aggregated effects on the brain and body after use.4,5,8
Over the years, cannabis growers have sought to increase the concentration of THC to produce the desired recreational effects. Hybridization, combined with more sophisticated extraction techniques, may elevate concentrations of THC to as high as 90%, which is approximately 212% higher than THC levels common in marijuana used during the 1960s.4,8,9 Marijuana extracts used in dabbing and edibles may have THC concentrations of 50% to 90%.8
Increases in THC levels also elevate addiction risk. Research shows that one in 10 cannabis users become addicted, with an increase in risk if the patient begins using prior to age 18.6 Mental health experts report an increased risk of psychosis or schizophrenia in some users based on the duration and frequency of use. This risk increases with family history of mental illnesses (genetic vulnerability) or when use begins at a younger age when the frontal lobe of the brain is not fully developed.6,8 In fact, a Swiss study found that heavy use of marijuana by the age of 18 increases the risk of schizophrenia by six times and shows positive relationships between use and schizophrenia even 15 years following use.10
The second most active ingredient found in cannabis is CBD, which does not impair cognition or induce psychotic effects.8,11 While research is ongoing, CBD has shown to be effective as a therapeutic drug for epilepsy and anxiety disorders.11 In therapeutic doses, CBD demonstrates efficacy as an analgesic, muscle relaxant, anticonvulsant, anxiolytic and antipsychotic. Furthermore, CBD has demonstrated anti-inflammatory and antioxidant properties. Scientific research has not caught up with the demand for CBD in medicine, leaving healthcare providers without sufficient information regarding the most effective therapeutic doses.11
In the United States, CBD is sold as a supplement and can be purchased in many forms, including lotions, tinctures, sublingual sprays, liquids, pills and edibles. However, like many other herbal supplements, none of these carry FDA approval; thus, no controls are in place to monitor the safety and purity of the ingredients contained in CBD mixtures. Many users believe CBD is safe because it is a natural substance, but it can cause liver damage, reproductive toxicity and infertility in animals.11 The FDA has approved one CBD medication, Epidiolex, for use in seizure disorders associated with Lennox-Gastaut syndrome and Dravet syndrome in patients older than 1 year.12 Recently, the FDA removed the Schedule V listing for Epidiolex due to the safety rating and minimal potential for abuse.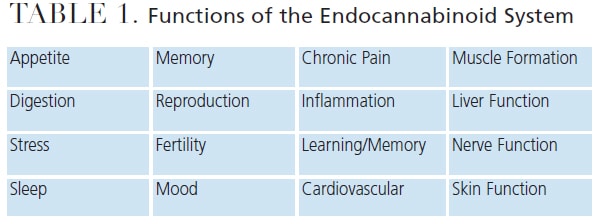
PHARMACOLOGY AND MECHANISM OF ACTION
Predicting the outcome of cannabis use is challenging, as the concentration of THC and method of delivery impact results. When cannabis products are inhaled (as in smoking or vaping), the user will experience a more rapid onset and increase in THC concentration in the body. As cannabinoids are rapidly distributed in vessel-rich areas, many effects are felt within seconds to minutes of inhalation — although they could also be delayed up to two hours.4
In 1992, Hanus identified the endocannabinoid system (ECS), which is responsible for a range of functions (Table 1) that contributes to the body’s ability to maintain homeostasis. Endocannabinoids are endogenous cannabinoids that are naturally produced.13,14 Hanus identified two main endocannabinoid receptors — CB1 and CB2 — located throughout the body; CB1 receptors are specific to the central nervous system, while CB2 receptors are specific to the peripheral nervous system. He also identified the enzymes responsible for breaking down endocannabinoids within the ECS system.13,14
Once ingested or inhaled, cannabinoids act on both receptors. Whereas THC can bind to both the CB1 and CB2 receptors (which causes both desirable and undesirable effects),11,15 CBD does not produce a high or negative effects; thus, investigators continue to explore how CBD interacts with the ECS.13–15 Researchers believe that CBD prevents endocannabinoids from breaking down.15
When THC binds to CB1 receptors in cardiovascular tissues, the central nervous system, and peripheral vascular tissues, it causes an increase in blood pressure and heart rate (Table 2). Research shows an increase in myocardial infarctions and cardiac arrhythmias with greater frequency of use.16 In fact, studies indicate a possible fivefold increase in the risk of a myocardial infarction in the first hour following the inhalation of cannabis.4 This multifactorial risk results from an increased heart rate and peripheral vasodilation, which causes compensatory orthostatic hypotension, combined with an increase in cardiac output and high oxygen demand.4 In the central nervous system, THC decreases cerebrovascular blood flow, raising the risk of a cerebral vascular accident or transient ischemic attack.16 Sudden cardiac deaths have occurred following use.3,17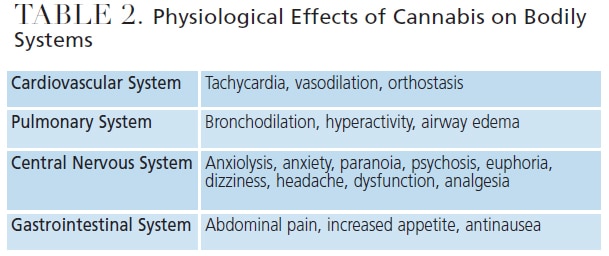
IMPLICATIONS FOR DENTAL CARE
Drug interactions with cannabis or CBD products may be difficult to predict. Oral health professionals should learn the signs and symptoms of active intoxication — paranoia, anxiety, tachycardia, hallucinations, hyperactivity and euphoric highs — as cannabis users will often not self-report.3 The use of non-FDA-approved synthetic cannabinoids has been connected with unexplained persistent bleeding, which may impact surgical interventions, such as extractions, grafting or periodontal therapy.4
With the increased heart rate and cardiorespiratory effects of THC, the use of local anesthetic containing epinephrine could be life-threatening in this population.3,17 Tachycardia and acute hypertension may occur if drugs with sympathomimetic activity, such as epinephrine, are introduced to a recent cannabis user. This is because the vasoconstrictor present in epinephrine fights against the vasodilation that occurs after inhalation of cannabis as the body’s systems struggle to return to homeostasis. Postponing treatment of a patient who appears to be intoxicated is prudent.3 All risks must be assessed prior to the initiation of any dental procedures.
As cannabis and anesthesia both affect the central nervous system, consideration should be given prior to prescribing anxiolytics or providing sedation procedures for a patient with a suspected or known history of cannabis use. Research has shown that patients who use cannabis products regularly require higher doses of sedatives and pain medications.4,18 Sedatives, such as benzodiazepines, barbiturates, nonbenzodiazepine hypnotics, and opioids or narcotics, reduce brain activity.3,4 These sedatives, which are often used to control pain and address anxiety and sleep disorders, are commonly used in general anesthesia procedures.4
In dentistry, providers may prescribe a mild sedative to relax patients with known dental phobias or anxiety disorders. Anxious patients may use cannabis in an attempt to “settle their nerves” without knowing the consequences and possible reactions of using both a sedative and cannabis. Additionally, when sedation or general anesthesia is provided for orthognathic surgeries, dental providers must understand the possible inherent risk associated with anesthesia medications and cannabis use. Postural hypotension and tachycardia have been noted in humans after any THC exposure.4 Research shows an increased risk for patients who have used cannabis prior to surgery, especially if it was smoked or vaped.3,4,17,18
Negative outcomes with general anesthesia administration following cannabis use are caused by bronchodilation and decreased airway resistance.4 Given the possibility of known or unknown drug interactions, dental providers should not provide additional pharmaceuticals for cannabis users. With cannabis use becoming more widespread, more research is needed to determine drug interactions. If emergency dental treatment is required, nitrous oxide is a safer alternative for pain management.3
Research shows that cannabis users have a higher tolerance to anesthesia, cross-tolerance for anesthesia agents, an increased risk of myocardial infarction, and may have increased airway reactivity.4 In addition, patients who routinely use cannabis products may require increased pain medications following treatment or surgery.4 A study by the American Osteopathic Association showed that marijuana users required an increased volume of common anesthesia medications during endoscopy procedures. The findings demonstrated that, on average, 14% more fentanyl, 20% more midazolam, and 200% more propofol was needed for patients with a history of routine cannabis use.18
CANNABIS EFFECTS ON ORAL TISSUES AND STRUCTURES
Cannabis consumption is associated with poor oral health, especially if concomitant use of tobacco, alcohol or other substances is combined with less frequent dental visits.19 Smoking or vaping cannabis causes xerostomia, which contributes to the acceleration of dental caries.19
Gingival enlargement, chronic inflammation, hyperkeratosis, leukoplakia and erythroplakia have been identified in patients who smoke cannabis. When cannabis is combined with tobacco, research has shown an increase in oral and neck cancers.19 Periodontitis, candidiasis and other dental sequela have also been reported in chronic cannabis users.
CONCLUSION
As states continue to legalize marijuana for a variety of uses, it is likely oral health professionals will encounter patients who may be under the influence of cannabis. In addition to increased mental health concerns, the dental team should be able to identify the signs and symptoms of use — and possible abuse — of cannabis products. This is especially true in situations in which dental patients require additional pain management techniques, such anxiolytics, local anesthetics with epinephrine, or general anesthesia. Additionally, there could be legal implications with informed consent, especially for irreversible procedures. Patients with acute cannabis intoxication have shown impairments with both memory and perception, which could influence their ability to give informed consent for treatment.
As licensed healthcare providers, dental professionals have the right and responsibility to know the type of cannabis product that has been used, route of administration, and frequency of use. In order to obtain this information, clinicians must have these discussions with patients. Oral healthcare teams should include a drug screening component in their initial health assessment to help identify the risk of possible drug interactions.
REFERENCES
- Hartman M. Cannabis overview. Available at: https://www.ncsl.org/research/civil-and-criminal-justice/marijuana-overview.aspx. Accessed October 25, 2022.
- National Conference of State Legislatures. State Medical Cannabis Laws. Available at: https://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx. Accessed October 25, 2022.
- Rechthand MM, Bashirelahi N. What every dentist needs to know about cannabis. Gen Dent. 2016;64:40–43.
- Alexander J, Joshi GP. A review of the anesthetic implications of marijuana use. Proc (Bayl Univ Med Cent). 2019;32:364–371.
- Whiting P, Wolff P, Deshpande S, et al. Cannaboids for medical use: a systematic review and meta-analysis. JAMA. 2015;323:2456–2473.
- U.S. Centers for Disease Control and Prevention. Marijuana and Public Health. Available at: https://www.cdc.gov/marijuana/index.htm. Accessed October 25, 2022.
- University of Mississippi. The Marijuana Project. Available at: https://pharmacy.olemiss.edu/marijuana/about/. Accessed October 25, 2022.
- Di Forti M, Morgan C, Dazzan P, et al. High potency cannabis and the risk of psychosis. Br J Psychiatry. 2009;156:448–491.
- Meehan-Atrash J, Luo W, Strongin R. Toxicant formation in dabbing: the terpene story. J Am Chem Soc. 2017;2:6112–6117.
- Luzi S, Morrison P, Powell J, Di Forti M, Murray R. What is the mechanism whereby cannabis use increases risk of psychosis. Neurotox Res. 2008;14:105–112.
- National Center for Biotechnology Information. Cannabidiol. Available at: https://pubchem.ncbi.nlm.nih.gov/compound/Cannabidiol. Accessed October 25, 2022.
- U.S. Food and Drug Administration. FDA approves first drug composed of an active ingredient derived from marijuana to treat rare, severe forms of epilepsy. Available at: https://www.fda.gov/news-events/press-announcements/fda-approves-first-drug-comprised-active-ingredient-derived-marijuana-treat-rare-severe-forms. Accessed October 25, 2022.
- Tantimonaco M, Ceci R, Sabatini S, et al. Physical activity and the endocannabinoid system: an overview. Cell Mol Life Sci. 2014;71:2681–2698.
- Mechoulam R, Lumir H, Pertwee R, Howlett A. Early phytocannabinoid chemistry to endocannabinoids and beyond. Nat Rev Neuro. 2014;15757–15764.
- Raypole C. A simple guide to the endocannabinoid system. Available at: https://www.healthline.com/health/endocannabinoid-system. Accessed October 25, 2022.
- Subramaniam V, Menezes A, DeSchutter A, Lavie C. The cardiovascular effects of marijuana. Are the potential adverse effects worth the high? Mo Med. 2019;116:146–153.
- Goyal H, Awad H, Ghali J. Role of cannabis in cardiovascular disorders. J Thorac Dis. 2017;9:2079–2209.
- Twardowski M, Link M, Twardowski N. Effects of cannabis use on sedation requirements for endoscopic procedures. J Am Osteopat Assoc. 2019;119:307–311.
- American Dental Association. Cannabis: Oral Health Effects. Available at: https://www.ada.org/resources/research/science-and-research-institute/oral-health-topics/cannabis-oral-health-effects. Accessed October 25, 2022.
From Decisions in Dentistry. December 2022;8(12)26-29.

