
 SVITLANA HULKO / ISTOCK / GETTY IMAGES PLUS
SVITLANA HULKO / ISTOCK / GETTY IMAGES PLUS
Dental Implants in Older Adults
Increasingly, clinicians are providing stable function by placing dental implants in patients in their 80s and 90s.
PURCHASE COURSE
This course was published in the February 2023 issue and expires February 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the February 2023 issue and expires February 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 690
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe how implant surface design and hard and soft tissue augmentation can expand applications for dental implant treatment.
- Explain clinical considerations for implant therapy in older adults.
- Discuss how implant placement in older adults can support overall health and quality of life.
The popularity of dental implants has grown rapidly as advances in implant therapy have created many choices for providers when treatment planning for patients with missing teeth. Halpern and Adams1 state the bioactivity of implant surface design, as well as the use of hard and soft tissue augmentation, provide a greater opportunity in the rehabilitation of the edentulous and partially edentulous jaw. Many providers now devote themselves solely to the placement and restoration of dental implants. This has provided patients with additional options and, in general, helped improve their oral function and quality of life.
With modern medical care, many individuals are living longer and healthier lives, and it is not uncommon to see patients that are 85, 90, or even older. Among this population, tooth loss due to periodontal disease, injury and caries is common, and many of these patients wear partial or full dentures. These appliances can cause further bone and tooth loss. As a typical denture becomes loose, the underlying soft tissue develops inflamed areas and eating becomes difficult. Dental implants improve life quality for many older individuals by facilitating better nutritional intake and encouraging a more social and active lifestyle.2 This paper, which includes a case report involving dental implant placement in a 94-year-old, will help illustrate the use of implant therapies in older adults.
The U.S. denture market is anticipated to grow at a compound annual rate of 6.4% from 2022 to 2028.3 Based on todays’ average fees, that equates to a $1.3 billion increase in dental fees. According to the U.S. Census Bureau, by 2030, older adults will outnumber children for the first time in U.S. history.4 These projections translate to an increase in the use of dental implants to support this growing population of patients with dentures. In their study of future implant needs, Elani et al5 reported a large increase in the prevalence of dental implants, from 0.7% in 1999–2000 to 5.7% in 2015–2016. The largest absolute increase in prevalence (12.9%) was among individuals ages 65 to 74, whereas the largest relative increase was 1000% in those ages 55 to 64. In addition, the team projected an increase by 2026 of up to 23%. In support of this growing trend of dental implant placement in older adults, a retrospective study by Takahashi et al6 reported the five-year implant survival rate in elderly patients was 99.0% and the 10-year cumulative survival rate was 98.1%.
DENTURE USE AND NUTRITION
Dentures have historically been the standard of care when treating fully edentulous patients. Replacement of missing teeth is important for the reconstruction of occlusal support and mastication. Although dentures may replace missing teeth, they function at a much-reduced level when compared to natural teeth. This is particularly true in the aging patient. Among this population, esthetics is rarely an issue — but the lack of being able to chew properly and embarrassment of having ill-fitting dentures are another story.
Especially as we age, our nutritional needs become a major factor in overall health. Of course, nutrition starts in the mouth, where masticating food makes it easier to swallow and also initiates digestion due to the amylase enzyme found in saliva. Amylase helps digest larger carbohydrates into smaller forms and reduces starch to a disaccharide-like maltose. Therefore, denture wearing — particularly among those with ill-fitting appliances — can be associated with malnutrition due to the reduced ability to properly masticate. In a 2022 cross-sectional study of older adults in long-term care, Meguro et al7 reported that denture use was directly linked to lip-closure ability and significantly associated with malnutrition. The authors further suggested that wearing dentures for tooth loss and maintaining oral function contributes to this poor nutritional status.
COMORBIDITY CONCERNS
Additionally, many older adults have comorbidities that directly impact the placement and long-term success of dental implants. Unfortunately, the aging process brings with it increased frailty and often involves common chronic conditions. Examples include cardiovascular disease, cancer, respiratory diseases (such as chronic obstructive pulmonary disease and lower respiratory infections), diabetes mellitus, cirrhosis of the liver, osteoarthritis, and conditions that involve neurocognitive impairment, such as depression and Alzheimer’s.
According to Halpern and Adams,1 clinicians should consider several key points when dealing with medically complex dental implant candidates:
- Dental implant therapy in medically complex patients is predicated on a well-thought-out surgical and restorative foundation that promotes both long-term function and improved, health-related quality of life.
- Implant therapy in medically compromised patients involves a multiplicity of presurgical, postsurgical and pharmacologic considerations.
- There is no consensus as to whether medically complex patients’ risk for early or late implant failure exceeds those of healthy patients.
- Additionally, there is no consensus as to whether implant therapy in immunocompromised individuals results in implant survival rates comparable to healthy cohorts.

Published studies of long-term dental implant success and survival provide more realistic options for restoration of function and esthetics regardless of age — and, in most cases, medical disabilities. After studying patients between 66 and 93 years of age, Becker et al8 report that older individuals receiving dental implants had excellent implant survival rates, low periodontal disease index scores, minimal changes in interproximal bone health, and outstanding quality of life scores. Additionally, they suggest this cohort can be maintained in good oral health. Therefore, in many cases implants (rather than dentures) are the treatment of choice. For patients affected with head and neck cancer, implants may be the only means to achieve a psychosocial and functional rehabilitation. Given the undoubted benefits of an implant-retained restoration compared to removable alternatives for oncology patients, the use of implants may even be justified when implant survival rates are significantly below those reported for healthy individuals.9 Similarly, patients with hyposalivation can benefit from implant-retained appliances due to the lack of retention of a standard denture9 and frequent sore spots due to reduced salivary production.

DENTAL IMPLANT PLACEMENT IN A 94-YEAR-OLD
In January 2022, a 94-year female presented for an exam, X-rays and replacement of her existing mandibular denture. Her main complaint was that the denture moved when she spoke or during mastication. The patient reported having trouble eating and that she frequently developed sore spots. In addition, the denture would sometimes fall out when she coughed or laughed. An examination of her health history showed she has arthritis, asthma, high blood pressure and thyroid disease. It was noted she is currently taking levothyroxine 125 mcg, lisinopril 30 mg, famotidine 20 mg, atorvastatin 20 mg, fluticasone propion-salmeterol inhaler, bid, clopidogrel 75 mg, and a daily aspirin. The patient indicated she had spoken to an individual who had received implants at the practice, and wanted to know if implants might be a viable approach to retain her mandibular denture.

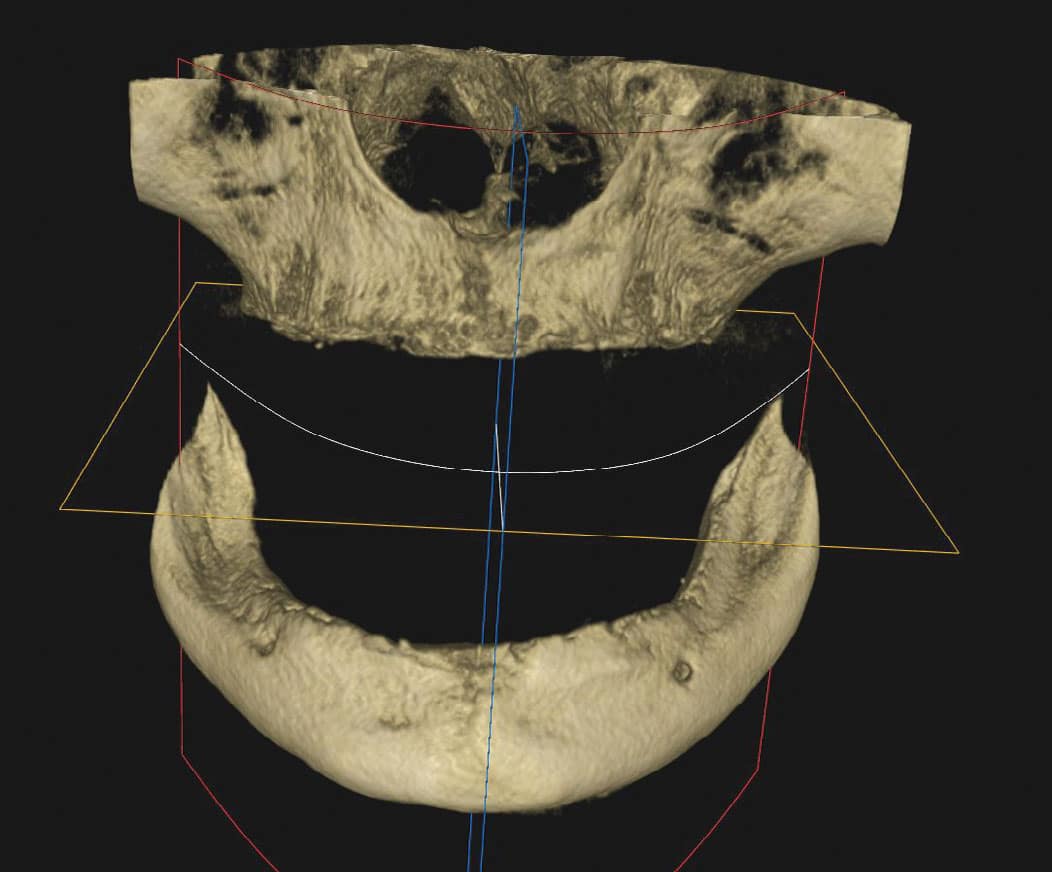
Physical examination of the patient revealed a very loose mandibular denture. Cone beam computed tomography (CBCT) was used to determine the quality and quantity of bone present so a definitive treatment plan could be established (Figure 1). After review of the CBCT scan and residual mandibular bone volume, it was determined that 3.5×10 mm implants could be placed in the anterior mandibular ridge, which should provide stability and adequate function. The patient was presented with three treatment plan options: (1) new maxillary and mandibular dentures; (2) an implant-retained mandibular denture, along with relining of her existing maxillary denture; and (3) an implant-supported fixed mandibular denture, along with relining of her existing maxillary denture. In addition to these options, the patient was given a detailed explanation of each procedure, associated healing time, the expected result, and fees for each option.
After questions and discussion, she chose the second option. Due to her age and medical history, a decision was made to use a treatment plan that included a punch procedure instead of the more common full-flap technique. This minimally invasive surgical approach was possible due to the presence of sufficient keratinized gingival tissue and bone volume in the implant recipient sites.10 This would minimize any trauma associated with reflecting a full tissue flap to expose the mandibular osseous tissue and avoid excess bleeding that might arise due to her long-term aspirin regimen. The patient said she understood the treatment plan and was ready to move forward as soon as possible. She was provided with prescriptions for amoxicillin 500 mg, ibuprofen 800 mg, and codeine/acetaminophen 30/300 mg to manage any possible post-placement pain. The patient was instructed to start the antibiotic and ibuprofen 24 hours prior to the punch procedure, and subsequently scheduled for implant placement.
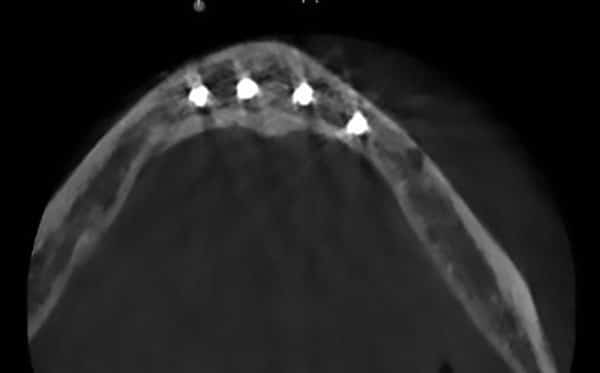
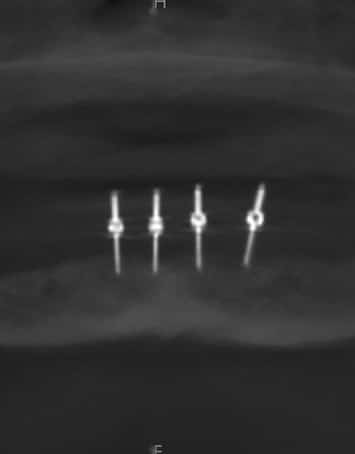
In approximately two weeks, the patient returned to have the implants placed. After reviewing the scheduled treatment, she was given four cartridges of 2% lidocaine in the area of teeth #21 to 29. Using a tissue punch, the tissue at the height of the residual mandibular ridge was removed in the approximate areas where teeth #22, 25, 26 and 28 were previously located. A curet was used to remove any tissue tags. After an initial pilot hole was obtained, guide pins were inserted to verify the angulation of each site (Figure 2). Next, osteotomies were performed at all four sites. Figure 3 and Figure 4 represent the area of tooth #25 and the typical volume/shape of the mandible in each of the final implant locations. The clinical team placed 3.5×10 mm implants in each location with a 3 mm attachment cuff height (Figure 5). Figure 6 represents an oblique CBCT slice revealing the final implant locations within the mandibular osseous structure. Figure 7 represents the quality of the soft tissue immediately following implant placement, which shows excellent tissue adaption, color, and lack of any residual trauma.
Finally, the existing mandibular denture was hollowed out to accept the implant cuffs and metal housing that would be used to secure any retentive devices. Acrylic was placed in the denture and the housings were captured in a picked-up impression (Figure 8). A complete relining of the maxillary and mandibular dentures was done with the new attachment hardware in place. No sutures were necessary and there was no bleeding at any of the implant sites. She returned the following day and everything appeared to be within normal limits. She was then scheduled to return in two weeks for follow-up and instructed to call if she had any questions or if there were any issues with her soft tissue, the implants or dentures.

FOLLOW-UP
The patient returned in two weeks and reported that everything was fine. She experienced no postsurgical discomfort and had not used any of the prescribed pain medications. The patient indicated being satisfied with the outcome. She was reminded to schedule bimonthly visits for the next six months.

In August 2022, the patient revisited for one of her routine follow-ups. Upon examination, the soft tissue appeared to be within normal limits. Neither mobility nor inflammation were noted, and she presented with minimal pocket depths. It was apparent the patient was doing an excellent job with her home care and denture cleaning, as well as her hygiene around the exposed implant attachment cuffs. She reported having no issues or discomfort, and that she was able to masticate without problems.

In September 2022, at eight months post-implant placement, she presented for a routine check-up, and reiterated that she was satisfied with her implant-retained dentures and function. An examination revealed the soft tissue around the four implants was within normal limits. The exam found no discoloration of the soft tissue, inflammation, or bleeding upon probing. The charted notes recorded less than 1 mm probing depth beyond the cuff and no mobility (Figure 9). A review of her maxillary and mandibular dentures was unremarkable and indicated once again that she was following the oral hygiene instructions provided by the office. Figure 10 shows an extraoral view of the dentures in place.
At the one-year post-implant placement visit in January 2023, another CBCT scan was scheduled as part of a routine follow-up examination.

CONCLUSION
Clinicians’ comfort levels in treating patients of advanced age have always been an issue in the dental office. Many practitioners will surmise that a patient may be too old or medically compromised to consider dental implants as part of a treatment plan. This is no longer the case. As this clinical report demonstrates, depending on the provider’s training, skill and confidence, older adults with many medical conditions can take advantage of recent advances in oral healthcare, including dental implants.
With the appropriate patient and proper treatment planning, adults in their 90s can still benefit from implant therapy.2 The resulting stability of the final appliance and marked improvement in the patient’s ability to masticate can improve quality of life, both mentally and physically. In addition, the improvement in digestion and nutrition facilitated by implant treatment can help support overall health and well-being.
References
- Halpern LR, Adams DR. Medically complex systemic disease and dental implant success/survival. Dent Clin N Am. 2021;65:1–19.
- How Old Is Too Old for Dental Implants? Available at: https://www.facialart.com/떋/葑/how-old-is-too-old-for-dental-implants/. Accessed January 6, 2023.
- Fortune Business Insights. Dentures Market Size, Share and COVID-19 Impact Analysis, By Type (Complete, and Partial), By Usage (Removable and Fixed), By End User (Dental Hospitals and Clinics, Dental Laboratories, and Others), and Regional Forecast, 2021–2028. Available at: https://www.fortune businessinsights.com/dentures-market-103337. Accessed January 6, 2023.
- Vespa J, Armstrong DM, Medina L. Demographic Turning Points for the United States: Population Projections for 2020 to 2060. Available at: https://www.census.gov/library/publications/떔/demo/p25-1144.html. Accessed January 6, 2023.
- Elani HW, Starr JR, Da Silva JD, Gallucci GO. Trends in dental implant use in the U.S., 1999–2016, and projections to 2026. J Dent Res. 2018;97:1424–1430.
- Takahashi T, Kihara M, Oki K, et al. Prognosis of implants with implant-supported fixed dental prostheses in the elderly population: A retrospective study with a 5- to 10-year follow-up. Healthcare (Basel). 2022;10:1250.
- Meguro A, Ohara Y, Iwasaki M, et al. Denture wearing is associated with nutritional status among older adults requiring long-term care: A cross-sectional study. J Dent Sci. 2022;17:500–506.
- Becker W, Hujoel P, Becker BE, Wohrle P. Dental implants in an aged population: evaluation of periodontal health, bone loss, implant survival, and quality of life. Clin Implant Dent Relat Res. 2016;18:473–479.
- Schimmel M, Srinivasan M, McKenna G, Muller F. Effect of advanced age and/or systemic medical conditions on dental implants survival: A systematic review and meta-analysis. Clin Oral Implants Res. 2018;29(Suppl 16):311–330.
- Dedhia DK, Rajaram V, Mahendra J, Parameswari D, Khanna S. Flapless soft tissue punch technique for implant placement — A case report. Int J Oral Health Dent. 2020;6:232–235.
From Decisions in Dentistry. February 2023;9(2)28-31.

