

Deciding Between Screw- Retained or Cemented Implant Restorations
Seung Kee Choi, DMD, MS, offers a prosthodontist’s perspective on the clinical choice between using screw- or cement-retained implant prostheses.
Dental implants are a widely embraced restorative therapy that is becoming more popular each year. While the specific case may drive the decision of whether the prosthesis should be cemented or screw retained, in many situations clinicians must determine which approach to use. To gain perspective on this key element of treatment planning, we asked Seung Kee Choi, DMD, MS, of the Department of Advanced Oral Sciences and Therapeutics at the University of Maryland School of Dentistry to share his thoughts on the screw-versus-cement decision.
SC: Students often approach me with a master cast for a single implant restoration and ask, “What kind of crown can we do on this implant: cement or screw retained?” After examining the cast, I provide an answer with an explanation, and the cast with the opposing are soon sent to the laboratory for fabrication of the implant restoration. In this short period of time, multiple thoughts race through my mind, but students do not often hear much of what I am thinking. On that note, here is a review of what the thought process might look like when deciding between a cemented or screwed prosthesis. Please note that “restoration” or “restorations” in this review refer to implant restorations ranging from single crowns to three-unit fixed partial dentures.
COMPARISON BETWEEN CEMENT- AND SCREW-RETAINED IMPLANT RESTORATIONS
While limited research indicates no significant difference between cemented and screw-retained implant restorations in terms of failure rates or biological complications, it may be worthwhile to consider the differences between the two types.1,2 For example, one systematic review reported that biological and technical complications were the main issues noted with cemented restorations, while technical complications were a chief concern with screw-retained prostheses (e.g., screw loosening).2 Another study reported patients with screw-retained implant restorations experienced ceramic chipping more frequently than those with cemented prostheses.3 Fortunately, these challenges raised in the literature can be addressed through abutment and/or restoration design, and by meticulously handling the materials and restoration type chosen.
For example, excess cement associated with peri-implantitis should not occur when the cement is properly selected and used. Similarly, ceramic chipping of screw-retained restorations can be minimized by ensuring sufficient ceramic material is present around the screw access hole, evaluating and equilibrating occlusion, and prescribing an occlusal guard, if needed.
Further comparing these two approaches may assist clinicians and patients in the treatment decision — when there is a luxury of choice. However, specific circumstances may not allow the option of either type of implant restoration, making any comparison irrelevant.
IMPLANT ANGULATION
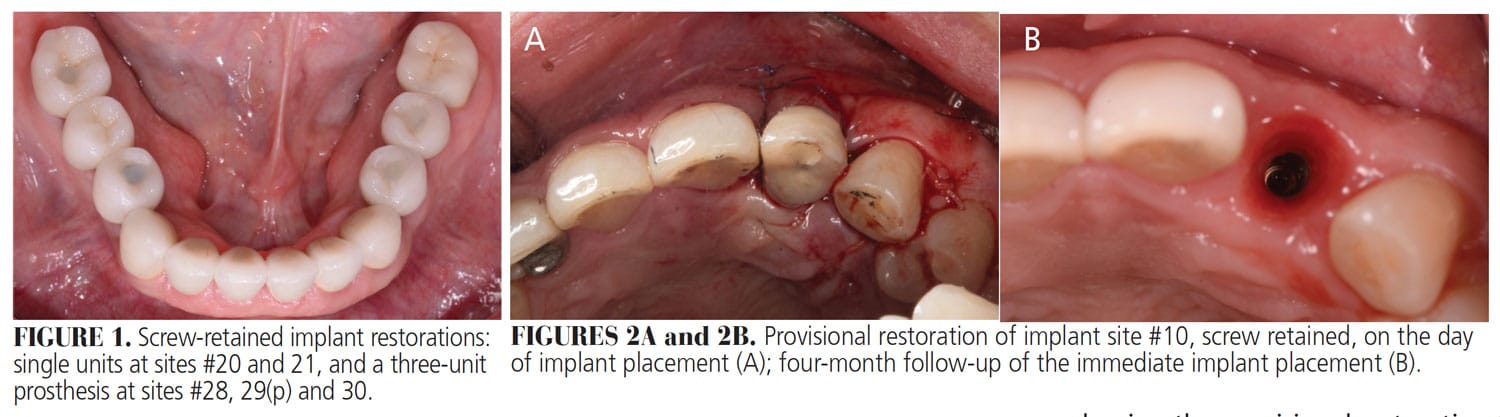
Implant angulation is one of the major factors in this decision. Screw-retained restorations are possible for implants in the posterior region when implant angulation is through the center of the restoration’s occlusal surface (Figure 1). In the anterior region, on the other hand, the implant may often be placed at an angle due to the angulation of the bone not allowing the implants to be placed palatally, away from the incisal edge. As a result, implant angulation leads to positioning the screw access hole through the labial surface of the crown, requiring angle correction in order to design an esthetic restoration. Though angle correction may reach up to (approximately) 30 degrees via angle-correcting implant or abutment design, most angle correction can be predictably addressed with a custom abutment, which would allow the coronal restoration to be retained using cement.
CEMENT AND PERI-IMPLANTITIS
Studies have found an association between peri-implantitis and excess cement in implant restorations.4,5 There may be multiple factors involved. For example, loading the implant crown with cement rather than thinly coating the intaglio of the crown may cause excess cement to descend subgingivally. If the abutment margin is placed subgingivally, this excess cement below the margin may not be removed entirely.6 To make matters worse, once set, cements (such as resin cement) would be almost impossible to remove if trapped below the abutment margin.
Proper cementation techniques to reduce excess cement around the implant have been well documented in the literature.7 Custom abutment designs would be preferred over stock abutments since margin placement can be controlled with the former. With proper abutment form, cements (such as zinc phosphate) may be sufficient for retention and conducive for removal of any excess material.
![FIGURE 3. Screw access hole obturated with composite resin; the angle-correcting abutment design allowed both retrievability and an esthetic outcome of this implant restoration at site #10.]() IMMEDIATE IMPLANT PROVISIONAL RESTORATION
IMMEDIATE IMPLANT PROVISIONAL RESTORATION

Though an implant may be unsuitable for screw-retained restoration due to the angulation of the bone in the maxillary anterior region, a screw-retained provisional for an immediately placed implant may be preferred (Figures 2A and 2B, and Figure 3). Any cement trapped in the subgingival area of an immediately provisionalized implant could result in inflammation, leading to poor soft and hard tissue healing. Excess cement also may be difficult to detect and remove in the surgical site due to bleeding and swollen soft tissue. Technically, shaping the provisional restoration to properly develop the peri-implant soft tissue may be better handled with screw-retained prostheses, as cementation does not allow providers to easily remove the provisional to change its contour.
RESTORATIVE SPACE
A cemented implant restoration requires approximately 7 mm of restorative space since two components, the abutment and coronal restoration, are involved.8 A screw-retained restoration, on the other hand, may be used if the space is even less than 4 mm — especially if the patient can accept an all-metal restoration (e.g., in non-esthetic areas).8
CLOSING THOUGHTS
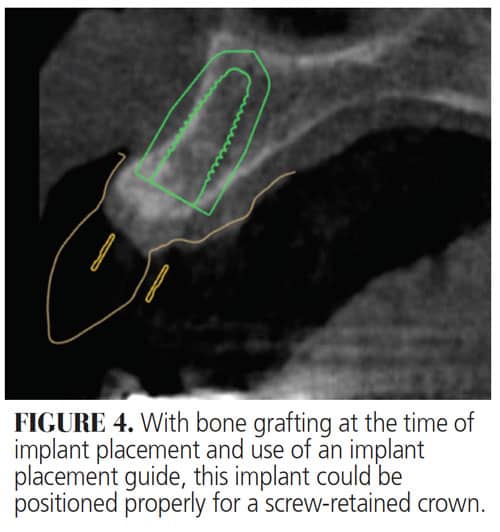
Cemented and screw-retained restorations are equally viable approaches in implant dentistry. Providers should be able to decide on the type of restoration during implant planning based on cone beam computed tomography since the existing hard tissue plays a vital role in determining implant angulation (Figure 4).
Supported by careful diagnosis and treatment planning, and armed with a thorough understanding of the advantages and disadvantages of each approach, implant providers should be able to reach a calculated decision of whether to use screw retained or cemented restorations. Equally important are abutment and prosthesis design, as well as the clinician’s handling of materials and restorations during delivery. Ultimately, from case assessment through surgical and restorative care, good decision-making and a proper and seamless workflow will help ensure successful outcomes in implant therapy.
The author has no conflicts to disclose.
REFERENCES
- Wittneben JG, Millen C, Brägger U. Clinical performance of screw- versus cement-retained fixed implant-supported reconstructions — a systematic review. Int J Oral Maxillofac Implants. 2014;29(Suppl):84–98.
- Millen C, Brägger U, Wittneben JG. Influence of prosthesis type and retention mechanism on complications with fixed implant-supported prostheses: a systematic review applying multivariate analyses. Int J Oral Maxillofac Implants. 2015;30:110–124.
- Nissan J, Narobai D, Gross O, Ghelfan O, Chaushu G. Long-term outcome of cemented versus screw-retained implant-supported partial restorations. Int J Oral Maxillofac Implants. 2011;26:1102–1107.
- Agar JR, Cameron SM, Hughbanks JC, et al. Cement removal from restorations luted to titanium abutments with simulated subgingival margins. J Prosthet Dent. 1997;78:43–47.
- Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 2009;80:1388–1392.
- Linkevicius T, Vindasiute E, Puisys A, Peciuliene V. The influence of margin location on the amount of undetected cement excess after delivery of cement‐retained implant restorations. Clin Oral Implants Res. 2011;22:1379–1384.
- Wadhwani C, Piñeyro A. Technique for controlling the cement for an implant crown. J Prosthet Dent. 2009;102:57–58.
- Carpentieri J, Greenstein G, Cavallaro J. Hierarchy of restorative space required for different types of dental implant prostheses. J Am Dent Assoc. 2019;150:695–706.
From Decisions in Dentistry. June 2021;7(6)12,14.
