
 ALEKSANDR GOLUBEV/ISTOCK/GETTY IMAGES PLUS
ALEKSANDR GOLUBEV/ISTOCK/GETTY IMAGES PLUS
Compound Odontoma Presenting As a Diagnostic Challenge
This clinical report investigates an asymptomatic, amorphous, radiopaque mass of disorganized hard tissue that was ultimately diagnosed as a compound odontoma.
PURCHASE COURSE
This course was published in the February 2022 issue and expires February 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the February 2022 issue and expires February 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the radiopaque mass, its presentation, and the proposed etiologies presented in this report.
- Explain the properties and clinical manifestations of each etiology considered in this case.
- Discuss the management and process of differential diagnosis involved with this odontoma.
In what might initially have appeared to be an unremarkable case, an 82-year-old female presented for extraction of tooth #31 after a periapical radiograph (Figure 1) showed the tooth to be unrestorable due to recurrent caries and periradicular pathology from an apparent failing endodontic treatment. Yet the radiograph also showed a well-defined, radiopaque mass in intimate contact with the distal root of tooth #31. The patient was asymptomatic and reported having no prior knowledge of the mass or the length of time it had been present. She declined sending a specimen to an oral pathologist for further examination. All third molars had been extracted earlier in life.
The patient was healthy for her age, with no contraindications for the extraction. Her notable medical history included a knee replacement surgery and a mastectomy without radiation therapy for breast cancer many years prior. Her blood pressure was well controlled with the use of a calcium-channel blocker. She was a patient of record at our clinic for one year.
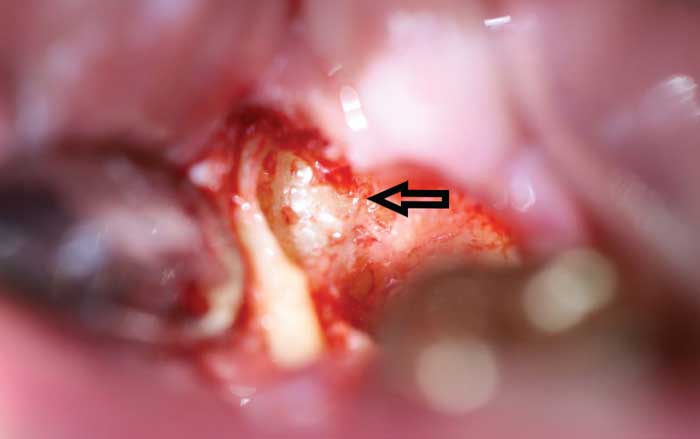
The tooth was extracted without incident, leaving the mass in question partially exposed on the distal aspect of the socket, as expected (Figure 2). The decision was made to remove the mass because it had direct exposure to the socket, making it easily accessible. It was conservatively exposed further (Figure 3) and removed in its entirety without complication (Figure 4).
Two oral surgeons, one periodontist, and one oral radiologist were consulted regarding the etiology of the sample. Together, they proposed three possibilities for the likely sample origin:
- It originated as a supernumerary tooth
- It was root structure, either a retained, migrated root from an extracted third molar, or an abnormal distal root on the second molar
- It was an odontoma
As no consensus was reached, the authors conducted a literature review on each possibility and performed supplemental histological imaging of the sample via scanning electron microscopy (SEM). This case and the differential diagnostic process are presented here in an effort to assist other clinicians who may encounter similar cases in the future.

SUPERNUMERARY TOOTH
Any teeth that are additional to the standard number are classified as supernumerary. These ancillary teeth can be found anywhere in the mouth.1 They are usually classified by when they appear (e.g., during primary or permanent dentition stages), where they appear in the dental arch, or by shape.2 They are found anywhere in the jaws, although some sources show that most are maxillary,3–5 and that up to 95% are found in the premaxilla.6 The morphology of supernumerary teeth can range from a normal appearance to more rudimentary shapes that are conical or tubercular. Proper diagnosis of a supernumerary tooth usually requires thorough clinical and radiographic examination.7 They are typically removed because they have high rates of impaction, which can lead to future complications, including delayed tooth eruption, tooth retention, diastema formation, and increased likelihood of cyst development.8–11
Large scale retrospective and review studies show that rates of supernumerary teeth are generally low, often reported to range between 0.8% to 3%, depending on the sampling population.3–5,11 There is also a tendency for supernumerary teeth to be more common in males than females,2–5,12 though there does not appear to be significant differences between genders in cases involving multiple supernumerary teeth.13 While most affected individuals will develop a single supernumerary tooth,3 developing multiple supernumerary teeth is usually associated with some type of genetic syndrome.4,14
Lubinsky and Kantaputra15 found supernumerary teeth to be strongly associated with eight Mendelian genetic disorders, which are those caused by mutation of a single gene.16 Of these, cleidocranial dysplasia may be most relevant to dentistry due to the many associated dental anomalies, such as retained supernumerary teeth causing delayed or absent root resorption, delayed eruption of the permanent teeth, and increased likelihood of dentigerous cysts, small palate, and malocclusion.17 Other syndromes associated with supernumerary teeth include Gardner syndrome, Ehler-Danlos syndrome, Ellis-van Crevald syndrome, Fabry-Anderson syndrome, Tricho-Rhino-Phalangeal syndrome, and syndromes linked to craniosynostosis.2,14,18,19
ROOT STRUCTURE
Another possibility investigated was that the mass could be a tooth root, either an additional second molar root or a migrated root fragment from a previously extracted third molar. On radiographs, the patient’s sample was clearly visible and possessed what may have been a periodontal ligament space, which is consistent with a root. Extra roots on lower second molars are uncommon in European populations, but reports show a 40% incidence of extra second molar roots in Chinese populations,20 and de Pablo et al21 showed that a third mandibular molar root can be a common variant in indigenous populations as well.
The normal root anatomy of mandibular second molars is similar to the first, with each having one mesial root and one distal. However, extra roots on molar teeth are often undetected on conventional radiographs because of superimposition or because the structure is very narrow.20 This may lead to underreporting of many root variants in the literature. In a study of 149 mandibular second molars, Manning22 found that the majority (76%) presented with the common mesial and distal roots, 22% had only one root, and 2% had three roots.
Few published reports on retained or migrated root tips exist, likely due to the sensitivity of the topic. However, in follow-up reports after third molar coronectomies, Monaco et al23 showed postoperative migration of the roots up to 4 to 5 mm in 80% of cases. This migration is interesting because movement, or eruption, of teeth is primarily driven by the development of the roots.24 However, Patel et al24 suggest that coronectomies may stimulate the periodontium and formation of cementum, thus triggering root migration. Further, histologic evaluation of these retained root fragments showed a vital pulp and no acute or chronic inflammatory infiltrate.24 These root fragments, isolated from the oral cavity and surrounded by bone, can remain asymptomatic in most cases.
The sample presented in this case report met several of the above criteria of a retained root in that there was no apparent inflammation, it remained isolated from the oral cavity until the adjacent tooth was extracted, and it was surrounded by bone.

ODONTOMA
Early work by Howard25 lists an odontoma as a subcategory of supernumerary dentition, although this is not widely accepted today. Rather, odontomas are classified as tumors that generally stop growing once they become fully mineralized — a clinical behavior that varies from many other tumors.26
There are two main categories of odontomas: compound and complex. The compound forms can possess masses of miniature teeth, or radiopaque masses of small, calcified structures, while the complex presentations are a homogenous mass of disorganized dentin and enamel.27 The complex form of odontomas seems to be more prevalent than compound, with most complex forms occurring asymptomatically in the posterior mandible.27 Some reports claim that, from a clinical standpoint, it is unnecessary to distinguish between the two types of odontomas, presumably because treatment for both types is the same: surgical removal.28 Odontomas often cause resorption in the adjacent tooth and may therefore cause oral health problems, even in patients who are asymptomatic.29
In 2014, Gedik and Muftuoglu30 reviewed the literature on odontomas and concluded they typically appear after the first two decades of life, are generally small in size, and, in contrast to the work above, found they occur most often in the anterior maxilla. Others report that odontomas are usually radiopaque and are surrounded by a thin, radiolucent zone corresponding to the follicular zone of a normal tooth.31 Unlike additional tooth roots, they are commonly found on routine radiographs, and though they can be removed with simple surgical techniques, patients who are asymptomatic may decline this option. The case illustrated in this article satisfied most of these common descriptions, and further presented without swelling or known discomfort to the patient.

SAMPLE DESCRIPTION AND ANALYSIS
Upon uneventful extraction of tooth #31, the entity in question was noted partially exposed in the area of the distal root socket (Figure 2). Due to its relatively small size, and the fact it was now exposed (potentially to the oral cavity), the mass was removed quite easily in its entirety (Figure 4). The structure was round and smooth, and was not consistent with bone or supernumerary teeth. However, neither a tooth root structure nor an odontoma could be ruled out.
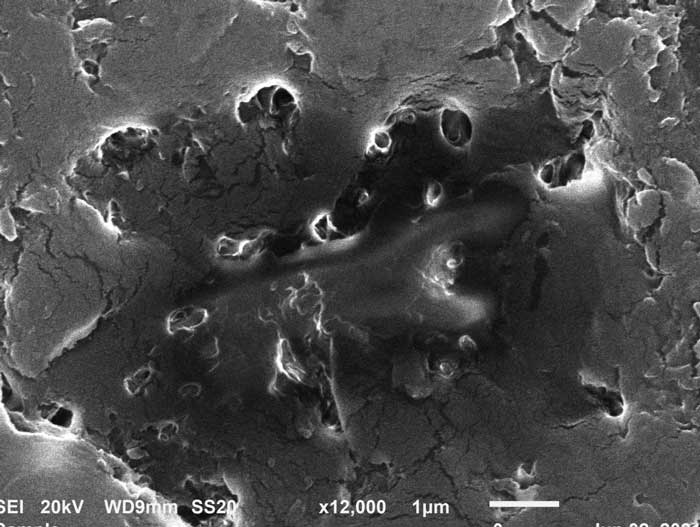
To provide additional information, the sample was serially dehydrated, embedded in acrylic, and thin-sectioned to expose the internal histology. It was then gold sputter-coated, mounted on slides and evaluated via SEM imaging. The images revealed a mass with a small, irregular hollow core surrounded by hard tissue, whose structure was largely disorganized and highly variable (Figure 5). Some sampled regions had features similar to the malformed dentin tubules reported elsewhere.32 However, no SEM images had characteristics that could conclusively identify the sample as being composed of enamel, dentin or cementum.
CONCLUSION
Based on the absence of a smooth, organized root morphology, and no regular openings of dentinal tubules, the authors confirmed the mass was not a supernumerary tooth. Because thin-sectioning and imaging did not reveal a vital pulp or clear pulp chamber, it was also concluded that it was not a piece of dissociated root. The anatomical location and morphological and histological properties of the sample were most consistent with a compound odontoma, as it was an asymptomatic, amorphous, radiopaque mass of disorganized hard tissue that developed in the posterior mandible. In addition, it bore no morphological resemblance to a tooth.33,34
However, its etiology was somewhat unique from prior reports in that it was not detected before age 30, and it did not appear to be associated with a specific syndrome. This could be because odontomas are also associated with environmental or genetic causes, including early life trauma to the primary dentition, genetic mutations, or familial ancestry.27
REFERENCES
- Garvey MT, Barry HJ, Blake M. Supernumerary teeth — an overview of classification, diagnosis and management. J Clin Dent Assoc. 1999;65:612–616.
- Yassin OM, Hamori E. Charasteristics, clinical features and treatment of supernumerary teeth. J Clin Pediatr Dent. 2009;33:247–250.
- Demiriz L, Durmuslar MC, Misir AF. Prevalence and characteristics of supernumerary teeth: a survey on 7348 people. J Int Soc Prev Community Dent. 2015;5(Suppl 1):S39–S43.
- Ata-Ali F, Ata-Ali J, Penarrocha-Diago M. Prevalence, etiology, diagnosis, treatment and complications of superumerary teeth. J Clin Exp Dent. 2014;6:e414–e418.
- Kumar DK, Gopal KS. An epidemiological study on supernumerary teeth: A survey on 5,000 people. J Clin Diag Res. 2013;7:1504–1507.
- Rao PVV, Chidzonga MM. Supernumerary teeth: literature review. Cent Afr J Med. 2001;47:22–26.
- Grimanis GA, Kyriakides AT, Spyropoulos ND. A survey on supernumerary molars. Quin Int. 1991;2:989–995.
- Cammarata-Scalisi F, Avendano A, Callea M. Main genetic entities associated with supernumerary teeth. Arch Argent Pediatr. 2018;116:437–444.
- Pippi R. Odontomas and supernumerary teeth: Is there a common origin? Int J Med Sci. 2014;11:1282–1297.
- Cawson R, Odell E. Cawson’s Essentials of Oral Pathology and Oral Medicine. Edinburgh: Churchill Livingstone; 2008:115.
- Nazargi Mahabob M, Anbuselyan GJ, Senthil Kumar B, Raja S, Kothari S. Prevalence rate of supernumerary teeth among non-syndromic South Indian populations: An analysis. J Pharm Bioallied Sci. 2012;4(Suppl 2):S373–S375.
- Rajab LD, Hamdan MAM. Supernumerary teeth: a review of the literature and a survey of 152 cases. Int J Paediatr Dent. 2002;12:244–254.
- Alvira-Gonzalez J, Gay-Escoda C. Non-syndromic multiple supernumerary teeth: meta-analysis. J Oral Pathol Med. 2012;41:361–366.
- Yague-Garcia J, Berini-Aytes L, Gay-Escoda C. Multiple supernumerary teeth not associated with complex syndromes: A retrospective study. Med Oral Patol Oral Cir Buccal. 2009;14:E331–E336.
- Lubinsky M, Kantaputra PN. Syndromes with supernumerary teeth. Am J Med Genet A. 2016;170:2611–2616.
- Mendelian inheritance. Available at: https://en.wikipedia.org/wiki/mendelian_inheritance. Accessed January 12, 2022.
- Hupp JR, Ellis E, Tucker MR. Contemporary Oral and Maxillofacial Surgery. 7th ed. New York: Elsevier; 2018.
- Kantaputra P, Miletich I, Ludecke HJ, et al. Tricho-rhino-phalangeal syndrome with supernumerary teeth. J Dent Res. 2008;87:1027–1031.
- Rice DP. Clinical features of syndromic craniosynostosis. Front Oral Biol. 2008;12:91–106.
- Scott GR, Irish JD, Martinon-Torres M. A more comprehensive view of the Denisovan 3-rooted lower second molar from Xiahe. Proc Natl Acad Sci USA. 2020;117:37–38.
- de Pablo OV, Estevez R, Sanchez MP, Heilborn C, Cohenca N. Root anatomy and canal configuration of the permanent mandibular molar: a systematic review. J Endod. 2010;36:1919–1931.
- Manning S. Root canal anatomy of mandibular second molars. Part I. Int Endod J. 1990;23:34–39.
- Monaco G, De Santis G, Pulpito G, Gatto M, Vignudelli E, Marchetti C. What are the types and frequencies of complications associated with mandibular third molar coronectomy? A follow-up study. J Oral Maxillofac Surg. 2015;73:1246–1253.
- Patel V, Sproat C, Kwok J, Beneng K, ThavaraJ S, McGurk M. Histological evaluation of mandibular third molar roots retrieved after coronectomy. Br J Oral Maxillofac Surg. 2014;52:415–419.
- Howard RD. The unerupted incisor. A study of the postoperative eruptive history of incisors delayed in their eruption by supernumerary teeth. Dent Pract Dent Rec. 1967;17:332–341.
- Neville BW, Damm DD, Allen C, Chi AC. Oral and Maxillofacial Pathology. 4th ed. Philadelphia: Saunders; 2016.
- de Oliveira BH, Campos V, Marcal S. Compound odontoma — diagnosis and treatment: three case reports. Pediatr Dent. 2001;23:151–157.
- Buchner A, Merrell P, Carpenter W. Relative frequency of central odontogenic tumors: A study of 1,088 cases from northern California and comparison to studies from other parts of the world. J Oral Maxillofac Surg. 2006;64:1343–1352.
- Hidalgo-Sanchez O, Lico-Berrocal M, Martinez-Gonzales J. Metaanalysis of the epidemiology and clinical manifestations of odontomas. Med Oral Patol Oral Cir Bucal. 2008;13:E730–E734.
- Gedik R, Muftuoglu S. Compound odontoma: diffferential diagnosis and review of the literature. West Indian Med J. 2014;63:793–795.
- Langlais RP, Miller CS, Gehrig JS. Color Atlas of Common Oral Diseases. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2017.
- Martinez Martinez M, Sanchez Romero C, Rumayor Pina A, Palma Guzman JM, Paes de Almeida O. Pigmented ameloblastic fibro-odontoma: clinical, histological, and immunohistochemical profile. Int J Surg Pathol. 2015;23:52–60.
- Iatrou I, Vardas E, Theologie-Lygidakis N, Leventis M. A retrospective analysis of the characteristics, treatment and follow-up of 26 odontomas in Greek children. J Oral Sci. 2010;52:439–447.
- Marchetti C, Piacentini C, Menghini P, Reguzzoni M. Observations on the enamel of odontomas. Scanning Microsc. 1993;7:999–1007.
From Decisions in Dentistry. February 2022;8(2):26-28,31.

