
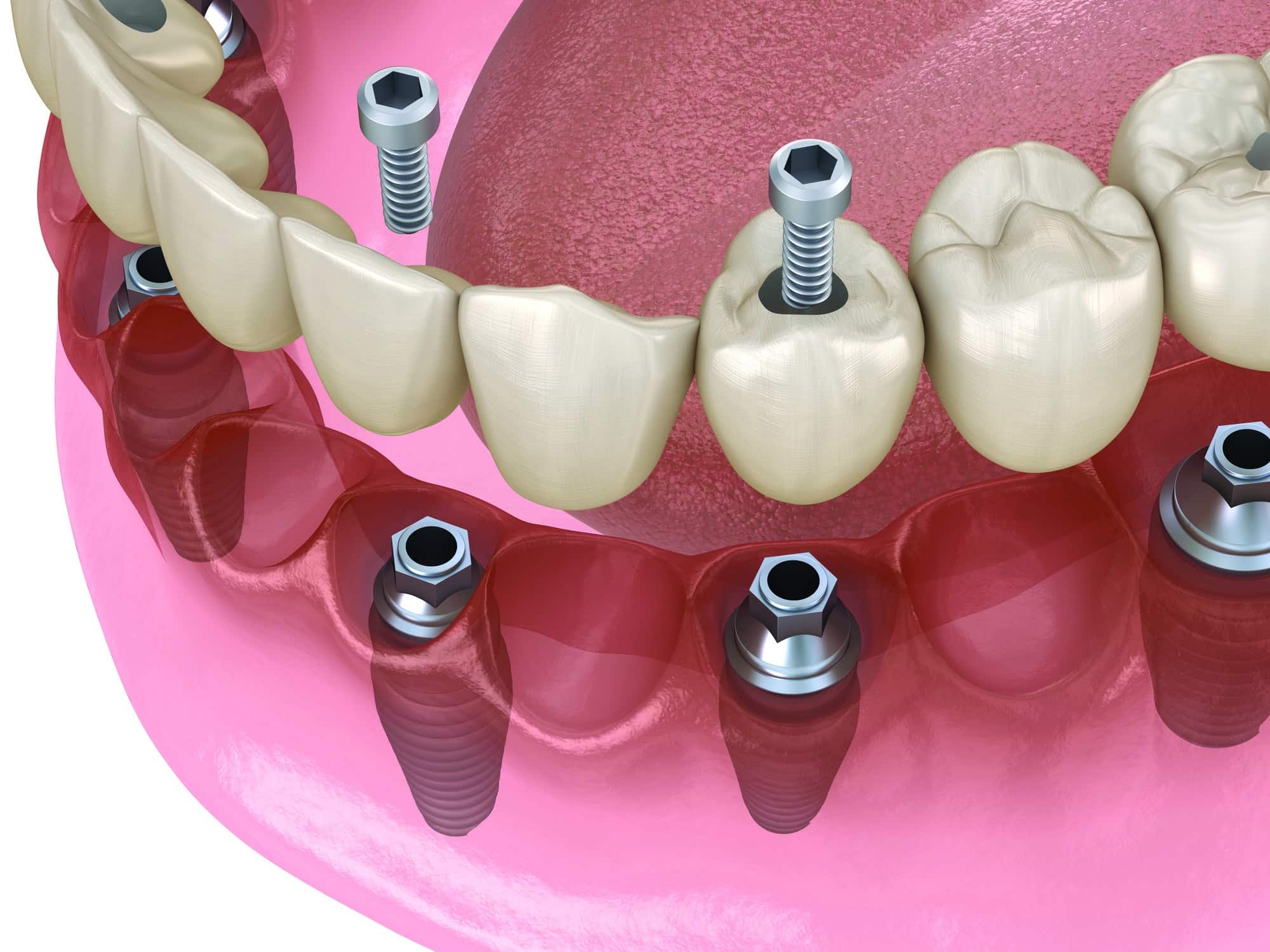
Clinical Considerations for Screw-Retained Dental Implants
Few topics spark more debate than whether to use a screw- or cement-retained restoration. Both approaches are clinically viable but understanding when and why to choose screw retention can dramatically influence long-term outcomes and patient satisfaction.1
Screw-retained restorations offer several advantages. For patients with a history of peri-implant disease or elevated risk of biological complications, screw retention supports more predictable maintenance. The option to remove the prosthesis allows for direct debridement and access to implant surfaces, aiding in disease control and prevention.1 This retrievability will enable clinicians to perform maintenance, address mechanical complications, or adjust prostheses without disturbing the implant-abutment connection. Equally important is the elimination of residual cement, a known contributor to peri-implant inflammation.1,2 By avoiding cement altogether, screw-retained designs reduce the risk of peri-implant mucositis and peri-implantitis.
Mechanically, screw retention enables more favorable load distribution, especially across multiple implants. The direct connection from implant to restoration creates a more predictable path for force transfer, reducing the likelihood of fracture during removal or function. In posterior regions, where occlusal loads are higher and hygiene is more difficult to maintain, the ability to remove the prosthesis without damaging the implant or restoration becomes paramount.3 Similarly, full-arch cases and those with multiple implants often benefit from screw retention, as its passive fit helps reduce mechanical stress and limit bone loss. Cases with less-than-ideal implant angulation also favor screw retention, allowing for better management of emergence profiles without risking cement entrapment in subgingival areas.3
However, these benefits do not come without drawbacks. Esthetics can be compromised, especially in the anterior where screw access holes may be visible. While careful angulation and restorative design can address this, it remains a limitation. Added complexity is also a factor. Achieving passive fit with screw-retained restorations often involves more sophisticated laboratory techniques and multiple clinical visits.2,3 This can increase both chair time and cost.
Clinicians must also manage potential complications including screw loosening, which still occurs in up to 15% of cases.3,4 Screw fractures, while rare, pose a challenge when they occur. Patients may also require more frequent maintenance and may find hygiene around restored access holes slightly more difficult, especially when composite fills are involved.
Ultimately, the decision between screw and cement retention should rest on an individualized risk-benefit analysis. High-risk patients, complex full-arch restorations, and cases where future intervention is likely anticipated typically benefit from screw retention. On the other hand, a single anterior implant with ideal angulation and low biological risk may warrant cement retention, as meticulous cement control is assured during the perioperative period.4
With careful planning, screw-retained restorations remain a cornerstone of modern implant dentistry. Their advantages in retrievability, maintenance, and biological safety make them invaluable when properly executed.
References
- Brandão ML, Bettore MV, Vidigal GM. Peri-implantitis and cement: A systematic review and meta-analysis. J Clin Periodontol. 2019;46:329-347.
- Kraus RD, Espuelas C, Hämmerle CHF, Jung RE, Sailer I, Thoma DS. Five-year randomized controlled clinical study comparing cemented and screw-retained zirconia-based implant-supported single crowns. Clin Oral Implants Res. 2022;33:537-547.
- Prakash J, Ranvijay K, Shenoy M, et al. Clinical success of screw-retained dental implants: a systematic review. J Contemp Dent Pract. 2022;23:118–122.
- Fiorillo L, D’Amico C, Ronsivalle V, Cicciu M, Cervino G. Single dental implant restoration: cemented or screw- retained? a systematic review of multi-factor randomized clinical trials. Prosthesis. 20246(4):871-886.
From Decisions in Dentistry. October/November 2025;11(5):46.
