

Clinical Applications of Soft Tissue Augmentation Around Implants
Keratinized mucosa plays a vital role in dental implant health, impacting oral hygiene, inflammation, and perI-implant complications.
PURCHASE COURSE
This course was published in the March 2024 issue and expires March 2027. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
The importance of keratinized mucosa around implants has been a controversial topic in the dental literature. The necessity of having adequate soft tissue to maintain health and decrease the incidence of implant complications is better understood today. Most studies have focused on the presence of keratinized mucosa, and findings suggest that its absence is associated with higher plaque accumulation, inflammation, and crestal bone loss.1
This course was published in the March 2024 issue and expires March 2027. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 690
Educational Objectives
After reading this course, the participant should be able to:
- Explain the association between the absence of keratinized mucosa and increased risks of plaque accumulation, inflammation, and crestal bone loss around dental implants.
- Discuss the significance of soft tissue grafting in improving the phenotype, oral hygiene procedures, and esthetics associated with implant therapy.
- Identify the optimal amount and thickness of keratinized mucosa required for maintaining peri-implant health, along with the timing, types, and techniques of soft tissue grafting procedures.
When the peri-implant soft tissue is composed of alveolar mucosa instead of keratinized mucosa, patients may be more prone to sensitivity during oral hygiene procedures. This leads to patients becoming less likely to perform proper oral hygiene. At the same time, clinical signs of inflammation (bleeding on probing, erythema, edema, and/or suppuration) have a more pronounced presentation in thin tissue compared to thick peri-implant tissue, although histologically, the extent of inflammation is similar.2,3 Finally, the absence of keratinized mucosa is usually found when there has been tooth loss and ridge resorption, as well as a significant decrease in vestibular depth. Inadequate vestibular depth hinders brushing access and further complicates oral hygiene performance.4
Peri-implant mucositis is defined as an inflammatory lesion of the soft tissues surrounding an endosseous implant and the absence or loss of supporting bone or continuing marginal bone loss.5 Plaque accumulation, clinical attachment loss, and soft tissue dehiscence are more likely to occur around implants that lack sufficient keratinized mucosa.6,7 All these may increase the patient’s risk for peri-implantitis. Furthermore, sites presenting with a thin peri-implant phenotype are more susceptible to developing peri-implant soft tissue recession in the presence of inflammation. Therefore, to decrease the occurrence of these biological complications, adequate soft tissue — both in terms of quantity and quality — must be achieved.
Goals of Soft Tissue Grafting Procedures Associated With Implant Therapy
Soft tissue grafting is necessary to improve the phenotype, facilitate oral hygiene procedures, and improve or correct the pink esthetics of implant prostheses by increasing the soft tissue thickness.8 After tooth extraction, the edentulous ridge resorbs significantly.9,10 Although alveolar ridge preservation procedures can help maintain the bone dimensions needed to place an implant, the volumetric shrinkage may still be significant.11
In esthetically demanding cases, which is most often when maxillary incisors, canines, and premolars are involved in high lip line patients, the resulting soft tissue deficiencies can be an esthetic concern (Figure 1 above). The aim of soft tissue grafting procedures, in conjunction with implant placement, is to either increase soft tissue thickness or re-establish the vestibule by widening the keratinized mucosa.
Amount of Keratinized Mucosa Required
As mentioned earlier, keratinized mucosa is desired but not indispensable for adequate peri-implant health. Nevertheless, there is a lack of consensus in the literature regarding its width and thickness. Most studies have established ≥ 2 mm as an “adequate” amount of keratinized mucosa because this is the amount required to prevent recession and inflammation, as well as facilitate adequate oral hygiene measures.12,13
A secondary parameter to consider is the horizontal thickness of the peri-implant mucosa. Schwarz et al14 found a mean mucosal thickness of 1.1 mm around healthy implants. Additionally, greater horizontal mucosal thickness is associated with less facial recession and fewer complications related to the translucency of the shade of the implant/abutment.15,16 Therefore, a mucosal thickness of ≥ 2 mm is considered thick and desirable.
Timing for Soft Tissue Grafting
Soft tissue grafting can be performed before, during, or following implant placement. If possible, it should be done at the time of implant placement to minimize the number of surgical procedures. Unless there is a need for papillary reconstruction where multiple surgeries may need to be performed, all soft tissue grafting procedures can be performed with a one-stage implant placement protocol.
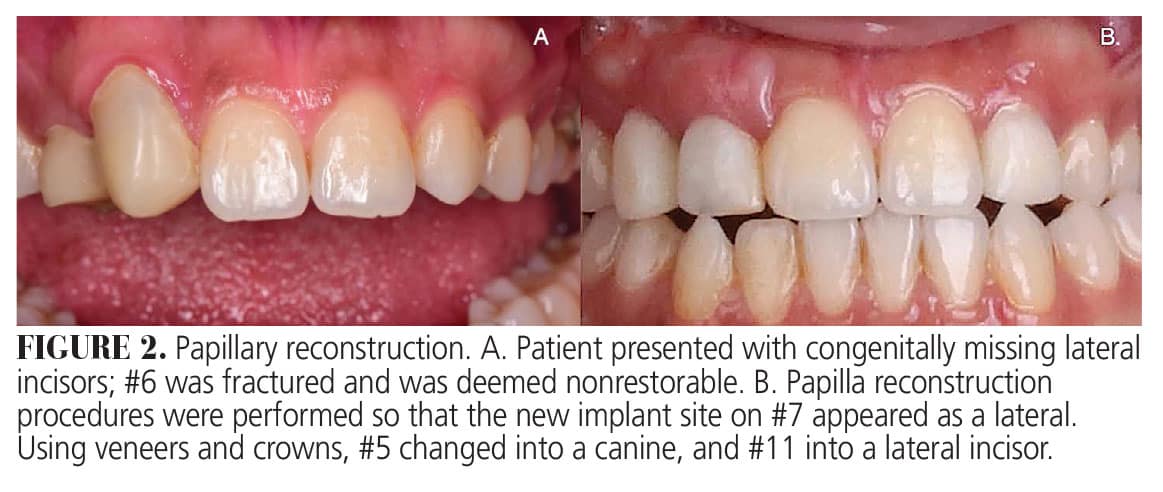 Combining the implant placement and the soft tissue grafting following a one-stage protocol makes it possible to significantly reduce the number of surgeries and the total burden of treatment associated with the procedure. In fact, to improve the patient benefit, addressing existing pathology on adjacent sites during the same surgery is possible (Figure 2).
Combining the implant placement and the soft tissue grafting following a one-stage protocol makes it possible to significantly reduce the number of surgeries and the total burden of treatment associated with the procedure. In fact, to improve the patient benefit, addressing existing pathology on adjacent sites during the same surgery is possible (Figure 2).
Types of Procedures
Depending on the indications of the affected site, the goals of soft tissue augmentation may differ. Generally, two types of procedures are the most utilized:
- Bilaminar techniques with subepithelial or de-epithelialized connective tissue grafts
- Onlay grafting techniques with free epithelialized gingival grafts.17
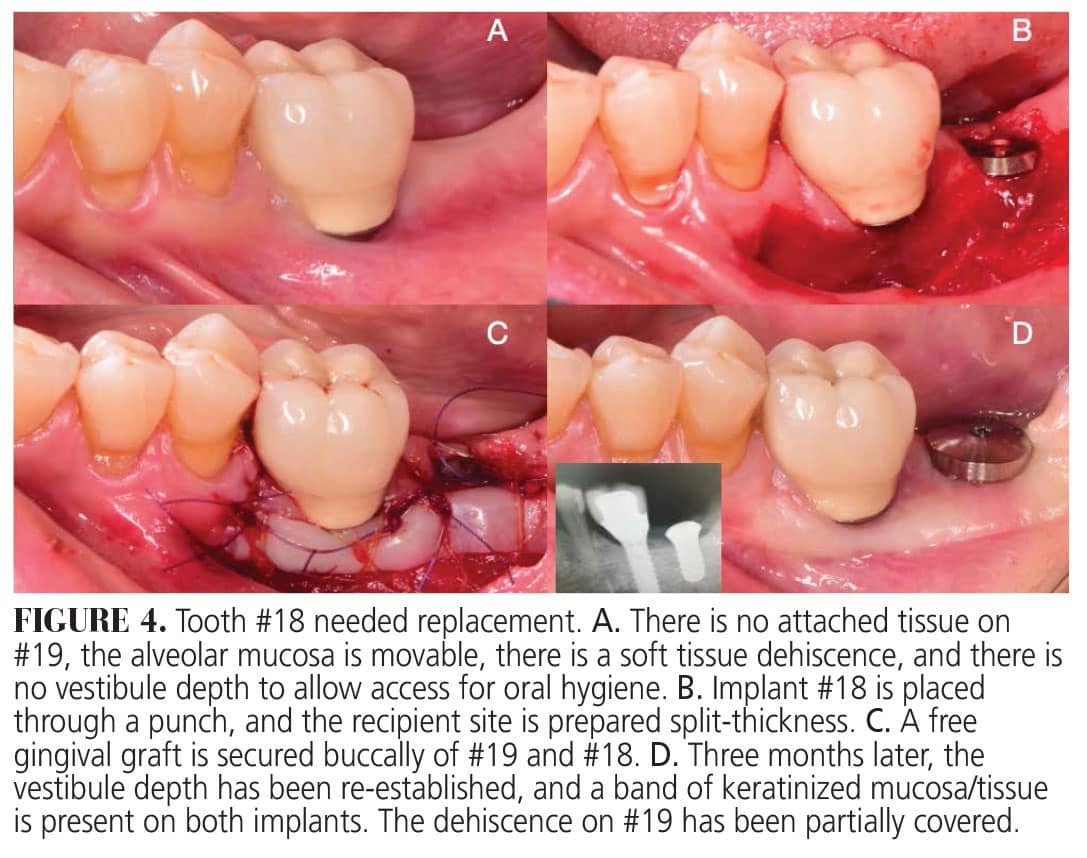
 In bilaminar techniques, a graft is placed underneath the mucosa to increase the thickness of the site without increasing the width of keratinized tissue. These techniques usually provide superior esthetic results. Onlay grafting procedures generally involve the use of free epithelialized grafts, which are secured to the recipient site to increase the width of keratinized mucosa (Figures 3 and 4).
In bilaminar techniques, a graft is placed underneath the mucosa to increase the thickness of the site without increasing the width of keratinized tissue. These techniques usually provide superior esthetic results. Onlay grafting procedures generally involve the use of free epithelialized grafts, which are secured to the recipient site to increase the width of keratinized mucosa (Figures 3 and 4).
![]() Types of Grafts
Types of Grafts
 Types of Grafts
Types of GraftsIn bilaminar techniques, grafts heal in a closed environment and different biomaterials may be used. In these techniques, a graft is used to increase the tissue thickness. Autogenous grafts include connective tissue grafts harvested from the palate or the tuberosity.17 Nonautogenous alternatives may be implemented to reduce patient morbidity by eliminating the need for a donor site.18 Soft tissue grafts of allogenic (human) origin include acellular dermal matrices; xenogenic (animal) origin includes collagen matrices that may or may not be cross-linked. In terms of increasing soft tissue thickness, all types of grafts are effective. However, for long-term stability, allografts and autogenous grafts perform similarly and are superior to xenografts.19
Autogenous grafts in the form of epithelialized free gingival grafts harvested from the palate are considered the gold standard for increasing the keratinized mucosal width. Xenogenic collagen or acellular dermal matrices have also been used to reduce morbidity. In terms of increasing the width of keratinized mucosa, autogenous free gingival grafts produce the best results, followed by acellular dermal matrix and collagen matrix.19
Soft Tissue Grafting to Increase Thickness
Bilaminar techniques can be used to change the phenotype by increasing the thickness of the mucosa around implants. Typically, an increase in keratinized mucosa is not expected when using bilaminar techniques around implants.20 However, clinical research on the necessity of keratinized mucosa primarily consists of retrospective studies, which have significant limitations in their interpretation. The characteristics of the underlying connective tissue may be more important with regard to brushing sensitivity. Having an underlying connective tissue of adequate thickness, consisting of dense collagen that is bound to the periosteum, compared to the connective tissue of the alveolar mucosa that is loose and rich in elastic fibers, may be more valuable than having a superficial layer of keratinization. Therefore, the crucial factor is to obtain an increased soft tissue thickness to achieve volume and natural esthetics. Additionally, in clinical experience, augmented sites are associated with less sensitivity despite the lack of keratinization.
Peri-Implant Health Outcomes
Using onlay grafting procedures to increase the width of keratinized mucosa leads to less brushing sensitivity, which results in lower plaque scores and probing depth reduction.21 If the procedure is performed in sites with an existing peri-implant soft tissue dehiscence, partial coverage may be achieved by a phenomenon called mucosal creeping (postoperative migration of the gingival margin in a coronal direction around implants).22 On the other hand, bilaminar techniques not only improve the esthetics and compensate for volume deficiencies, but they also increase the stability of the crestal bone levels around implants.23
Healing of Soft Tissue Augmentation Around Implants
The healing process of soft tissue grafts around teeth has been extensively studied; however, not as much around implants. Numerous seminal studies have described the three initial healing phases of free epithelialized gingival grafts:24,25
- The initial phase, which lasts 0 to 2 days, is the “stage of plasmatic circulation,” in which the nutrition of the graft occurs via plasmatic perfusion from the recipient bed. The outer epithelial layer will degenerate, and the dead superficial epithelial cells will slowly slough away.
- The next phase is the “stage of vascularization,” which lasts 2 to 8 days. New capillaries will form throughout the recipient bed and graft, establishing circulation between the two.
- The final phase is the “stage of organic union,” which lasts 4 to 10 days. An organic union between the connective tissue bed and the graft is established to achieve a fibrous attachment.
After this, tissue maturation will follow for several months.
Subepithelial autogenous grafts heal differently. They receive their blood supply from the periosteal bed connective tissue and the overlying flap. Blood vessels invade the graft by 1 week.26 By 14 days, the graft is completely revascularized, and, by day 28, the vasculature has regained its typical pattern. By 2 months of healing, the grafted tissue has matured with intermediate characteristics of the donor and recipient sites.27
Dental Implant Maintenance
Compliance with supportive periodontal and peri-implant therapy is crucial to achieving longevity of teeth and implants. Therefore, in cases where patients comply with their maintenance interval and maintain healthy peri-implant tissues by using appropriate oral hygiene techniques, the width and thickness of keratinized mucosa may not be as relevant.
Nevertheless, an implant surrounded by alveolar mucosa and/or having a shallow vestibule will make proper oral hygiene difficult due to discomfort, which leads to plaque accumulation and inflammation.28 The amount of keratinized mucosa may be more important for patients with irregular and erratic maintenance compliance.29 With that premise, Monje and Blasi30 found that the presence of < 2 mm of keratinized mucosa around dental implants on erratic maintenance compliers seems to be associated with peri-implant disease.30 Therefore, for those patients, surgical intervention to enhance the quality and quantity of the peri-implant soft tissues may be recommended to ensure the longevity of their implants.
Conclusions
Several factors contribute to the long-term success of dental implants. The quality and quantity of the peri-implant tissues is a critical factor. It seems that at least 2 mm of keratinized mucosa is desired to allow for adequate oral hygiene and, in that way, reduce plaque, inflammation, and crestal bone loss.
Several surgical techniques have been described to enhance the peri-implant tissues. Free epithelialized gingival grafts are the gold standard for increasing the keratinized mucosa. Nevertheless, bilaminar techniques using autogenous, allogenic, or xenogenic grafts have been used to enhance the thickness, volume, and esthetics of the tissues surrounding dental implants.
It is essential to assess each patient individually and determine the best treatment approach.
References
- Sanz M, Schwarz F, Herrera D, et al. Importance of keratinized mucosa around dental implants: consensus report of group 1 of the DGI/SEPA/Osteology Workshop. Clin Oral Implants Res. 2022;33(Suppl 23):47–55.
- Wennstrom J, Lindhe J. Plaque-induced gingival inflammation in the absence of attached gingiva in dogs. J Clin Periodontol. 1983;10:266–276.
- Wennstrom J, Lindhe J, Nyman S. Role of keratinized gingiva for gingivai health clinical and histologic study of normal and regenerated gingivai tissue in dogs. J Clin Periodontol. 1981;8:311–328.
- Halperin-Sternfeld M, Zigdon-Giladi H, Machtei EE. The association between shallow vestibular depth and peri-implant parameters: a retrospective 6 years longitudinal study. J Clin Periodontol. 2016;43:305–310.
- Heitz-Mayfield LJA, Salvi GE. Peri-implant mucositis. J Periodontol. 2018;89:S257-S266.
- Perussolo J, Souza AB, Matarazzo F, Oliveira RP, Araújo MG. Influence of the keratinized mucosa on the stability of peri-implant tissues and brushing discomfort: A 4-year follow-up study. Clin Oral Implants Res. 2018;29:1177–1185.
- Grischke J, Karch A, Wenzlaff A, Foitzik MM, Stiesch M, Eberhard J. Keratinized mucosa width is associated with severity of peri-implant mucositis. A cross-sectional study. Clin Oral Implants Res. 2019;30:457–465.
- Bienz SP, Pirc M, Papageorgiou SN, Jung RE, Thoma DS. The influence of thin as compared to thick peri-implant soft tissues on aesthetic outcomes: a systematic review and meta-analysis. Clin Oral Implants Res. 2022;33:56–71.
- Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003;23:313–323.
- Iasella JM, Greenwell H, Miller RL, et al. Ridge preservation with freeze-dried bone allograft and a collagen membrane compared to extraction alone for implant site development: a clinical and histologic study in humans. J Periodontol. 2003;74:990-999.
- Avila-Ortiz G, Chambrone L, Vignoletti F. Effect of alveolar ridge preservation interventions following tooth extraction: a systematic review and meta-analysis. J Clin Periodontol. 2019;46:195–223.
- Avila-Ortiz G, Gonzalez-Martin O, Couso-Queiruga E, Wang HL. The peri-implant phenotype. J Periodontol. 2020;91:283–288.
- Ravidà A, Arena C, Tattan M, et al. The role of keratinized mucosa width as a risk factor for peri-implant disease: a systematic review, meta-analysis, and trial sequential analysis. Clin Implant Dent Relat Res. 2022;24:287–300.
- Schwarz F, Claus C, Becker K. Correlation between horizontal mucosal thickness and probing depths at healthy and diseased implant sites. Clin Oral Implants Res. 2017;28:1158–1163.
- Lops D, Stellini E, Sbricoli L, Cea N, Romeo E, Bressan E. Influence of abutment material on peri-implant soft tissues in anterior areas with thin gingival biotype: a multicentric prospective study. Clin Oral Implants Res. 2017;28:1263–1268.
- Mailoa J, Arnett M, Chan HL, George FM, Kaigler D, Wang HL. The association between buccal mucosa thickness and periimplant bone loss and attachment loss: a cross-sectional study. Implant Dent. 2018;27:575–581.
- Zucchelli G, Tavelli L, McGuire MK, et al. Autogenous soft tissue grafting for periodontal and peri-implant plastic surgical reconstruction. J Periodontol. 2020;91:9-16.
- Tavelli L, McGuire MK, Zucchelli G, et al. Extracellular matrix-based scaffolding technologies for periodontal and peri-implant soft tissue regeneration. J Periodontol. 2020;91:17-25.
- Tavelli L, Barootchi S, Avila-Ortiz G, Urban IA, Giannobile WV, Wang HL. Peri-implant soft tissue phenotype modification and its impact on peri-implant health: a systematic review and network meta-analysis. J Periodontol. 2021;92:21–44.
- Liñares A, Rubinos A, Puñal A, Muñoz F, Blanco J. Regeneration of keratinized tissue around teeth and implants following coronal repositioning of alveolar mucosa with and without a connective tissue graft: an experimental study in dogs. J Clin Periodontol. 2022;49:1133–1144.
- Oh SL, Ji C, Azad S. Free gingival grafts for implants exhibiting a lack of keratinized mucosa: extended follow-up of a randomized controlled trial. J Clin Periodontol. 2020;47:777–785.
- Parra C, Capri D. Peri-implant mucosal creeping: two case reports. Int J Periodontics Restorative Dent. 2018;38:227–233.
- Puzio M, Hadzik J, Błaszczyszyn A, Gedrange T, Dominiak M. Soft tissue augmentation around dental implants with connective tissue graft (CTG) and xenogenic collagen matrix (XCM). 1-year randomized control trail. Ann Anat. 2020:230:151484.
- Sullivan HC, Atkins JH. Free autogenous gingival grafts: principles of successful grafting. Periodontics. 1968;6:121–129.
- Oliver RC, Loe H, Karring T. Microscopic evaluation of the healing and revascularization of free gingival grafts. J Periodontal Res. 1968;3:84–95.
- Guiha R, Khodeiry S El, Mota L, Caffesse R. Histological evaluation of healing and revascularization of the subepithelial connective tissue graft. J Periodontol. 2001;72:470–478.
- Perotto S, Romano F, Cricenti L, Gotti S, Aimetti M. Vascularization and innervation of connective tissue grafts in the treatment of gingival recessions: a histologic and immunohistochemical study. Int J Periodontics Restorative Dent. 2017;37:551–558.
- Souza AB, Tormena M, Matarazzo F, Araújo MG. The influence of peri-implant keratinized mucosa on brushing discomfort and peri-implant tissue health. Clin Oral Implants Res. 2016;27:650–655.
- Wilson TG, Glover ME, Schoen J, Baust C, Jacobs T. Compliance with maintenance therapy in a private periodontal practice. J Periodontol. 1984;55:469–473.
- Monje A, Blasi G. Significance of keratinized mucosa/gingiva on peri-implant and adjacent periodontal conditions in erratic maintenance compliers. J Periodontol. 2019;90:445–453.
From Decisions in Dentistry. March 2024; 10(2):32-35

