
Attachment Selection for Implant-Supported Overdentures
These clinical considerations will help providers choose the most appropriate stud attachment systems for removable overdenture therapy.
PURCHASE COURSE
This course was published in the April 2023 issue and expires April 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the April 2023 issue and expires April 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 690
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe stud attachment systems, indications, and related materials for implant-supported removable overdenture treatment.
- Explain the biomechanics of implant stud attachment systems.
- Discuss implant divergence and restorative space requirements for implant overdentures.
Implant overdenture therapy is an effective way to rehabilitate edentulous patients.1 Resilient stud attachment systems provide retention, support and stability to implant overdentures. Careful consideration of the implant attachment system and prosthesis design prior to surgical implant placement will have a strong influence on overall outcomes. With effective planning, the restorative phase and long-term maintenance are not only streamlined, but also more predictable — which, together, support optimal treatment success.
A variety of abutments have been developed for removable implant-supported prostheses. Studies from classical literature compare bar-type, magnetic and ball attachments. Individual stud abutments have gained popularity due to their ease of use and fewer prosthetic complications.2,3 Still, with any attachment system, primary retention decreases from the time of overdenture insertion. This is caused by a lack of implant parallelism, compromised path of prosthesis placement and removal, abutment wear, and insert degradation.4 Novel stud designs aim to improve mechanical retention by modifying the abutment profile and surface coating.5–9 The material composition of the retentive inserts has evolved to impart increased retentive forces at the abutment-attachment interface. This article will discuss the features and indications of currently available stud attachment systems.
PROSTHESIS RETENTION AND IMPLANT DISTRIBUTION
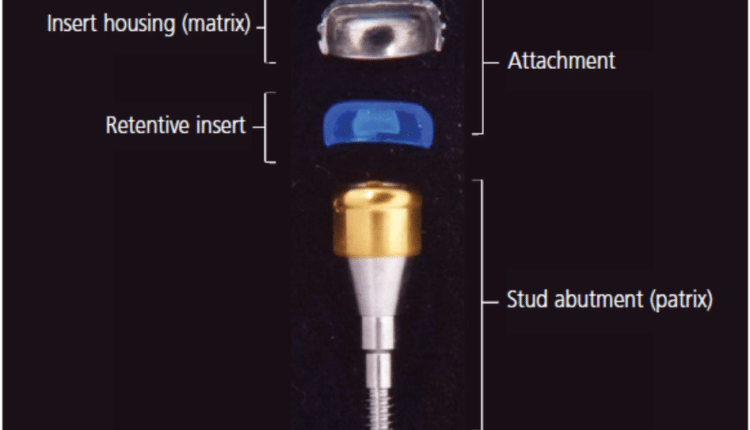
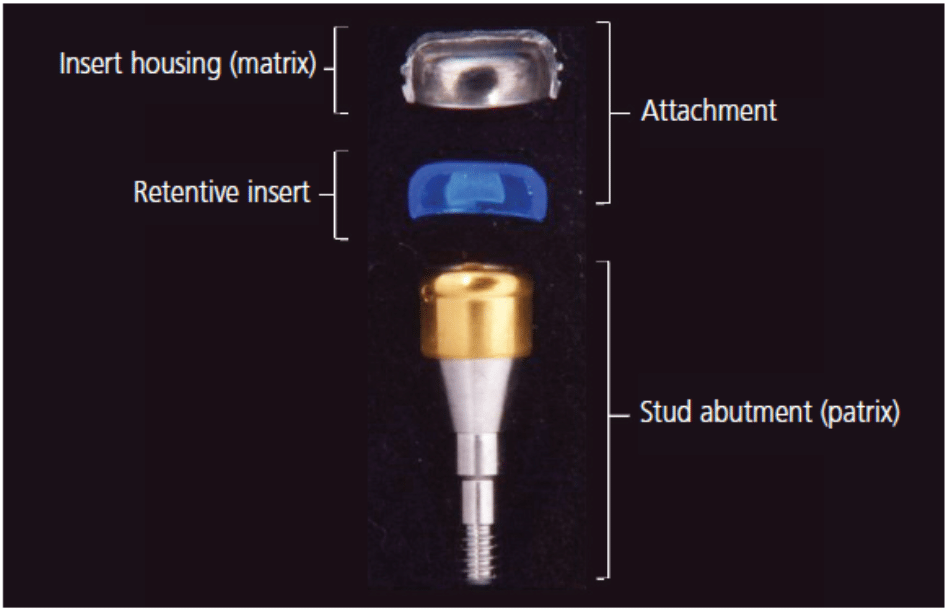
A resilient stud attachment system most often consists of a cap-like housing embedded within the denture base, a retentive insert located within the housing, and a semi-precision abutment secured to the dental implant (Figure 1). The properties of the attachment assembly allow micromovement during prosthesis seating, as the mucosa and underlying soft tissues undergo some degree of deformation. Assuming a well-fitting intaglio surface of the overdenture, excessive forces exerted on the abutment are negated.10
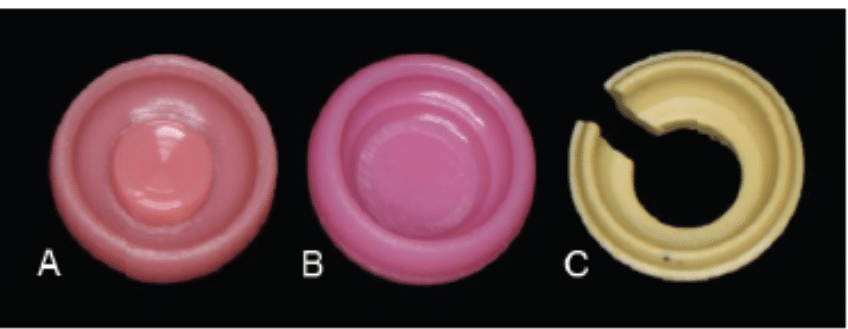
abutments: nylon with dual internal and external engagement features (A); nylon with external retention grooves (B); and polyetheretherketone C-shaped with external engagement design (C).
For edentulous patients who are implant candidates, the two-implant mandibular overdenture opposing a maxillary conventional denture is the first-choice treatment.11 Randomized controlled trials, as well as benchtop studies, have demonstrated that mandibular overdenture retention provided by free-standing abutments is directly proportional to the number and distribution of implants.12,13 Two mandibular implants positioned at either the cuspids or second premolars afford comparable resistance to dislodgment forces.12–14 As the prosthesis engages additional implants, the overdenture becomes less tissue-supported and increasingly implant-borne.12 Research by Scherer et al12 revealed that when engaging four dental implants, utilizing either the lateral incisor and cuspid sites, or the cuspids and second premolars, provided the greatest dislodgement force. When testing anteroposterior dislodgment, the displacement force was greatest in scenarios of four implants positioned in the anterior mandible at the lateral incisor and cuspid positions. Not surprisingly, the least retention was observed when a single implant was placed at the central incisor position. The clinician must bear in mind the presence of cantilevers attributed to unfavorable implant distribution and/or number also renders the attachment-abutment complex highly susceptible to loss of retention.
Conventional inserts for stud attachments provide acceptable retention, particularly when dental implants are parallel to one another. When implants are either intentionally or unintentionally positioned non-parallel to one another and non-perpendicular to the occlusal plane, retentive inserts and abutments may wear rapidly.13,14
Traditional stud abutments require a unique driver for placement and may or may not be detachable after becoming worn. Resilient implant inserts, composed of nylon, silicone, gold or plastic, become distorted over time and eventually require replacement. More recently, many stud abutments can be placed with a standard hex driver.15,16 In the past, the driver access on the coronal surface of stud abutments has been difficult for some patients to keep clear of debris and plaque, resulting in incomplete seating of the restoration and accelerated loss of resilience in the system.17 This has been particularly true when the driver access served a dual purpose by engaging the insert internally (see Figure 2 for common styles of retentive inserts).
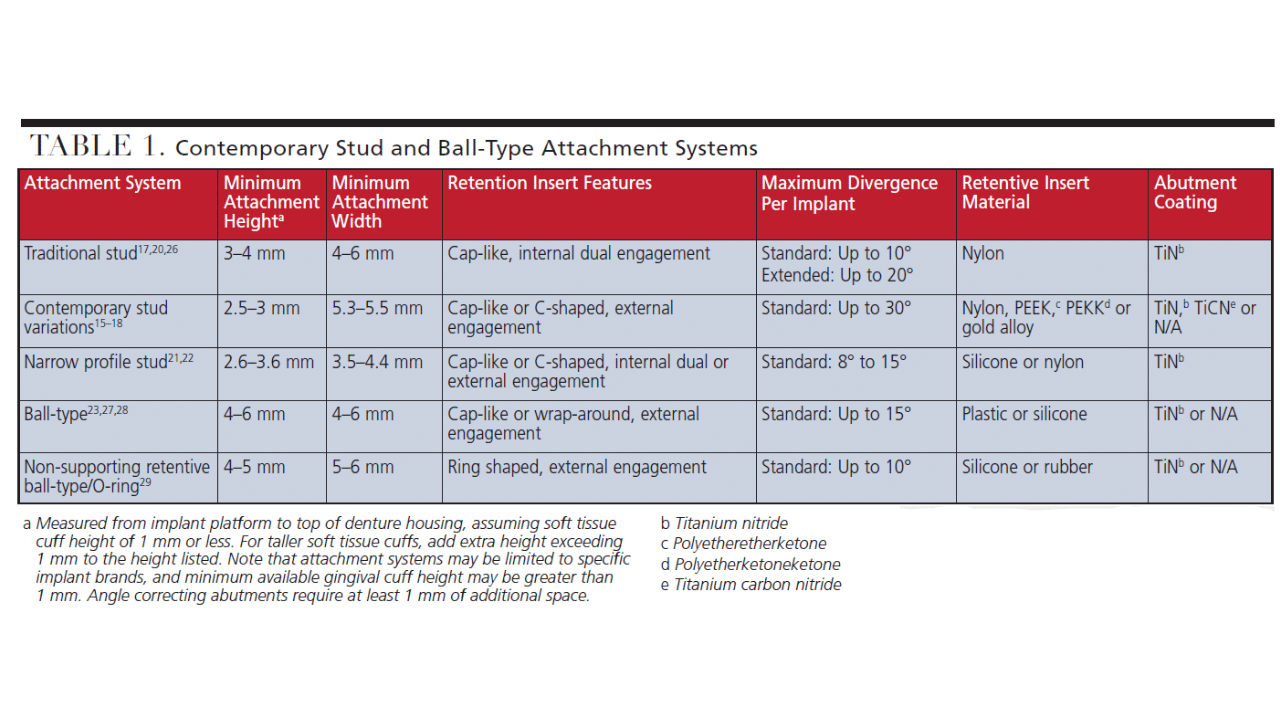
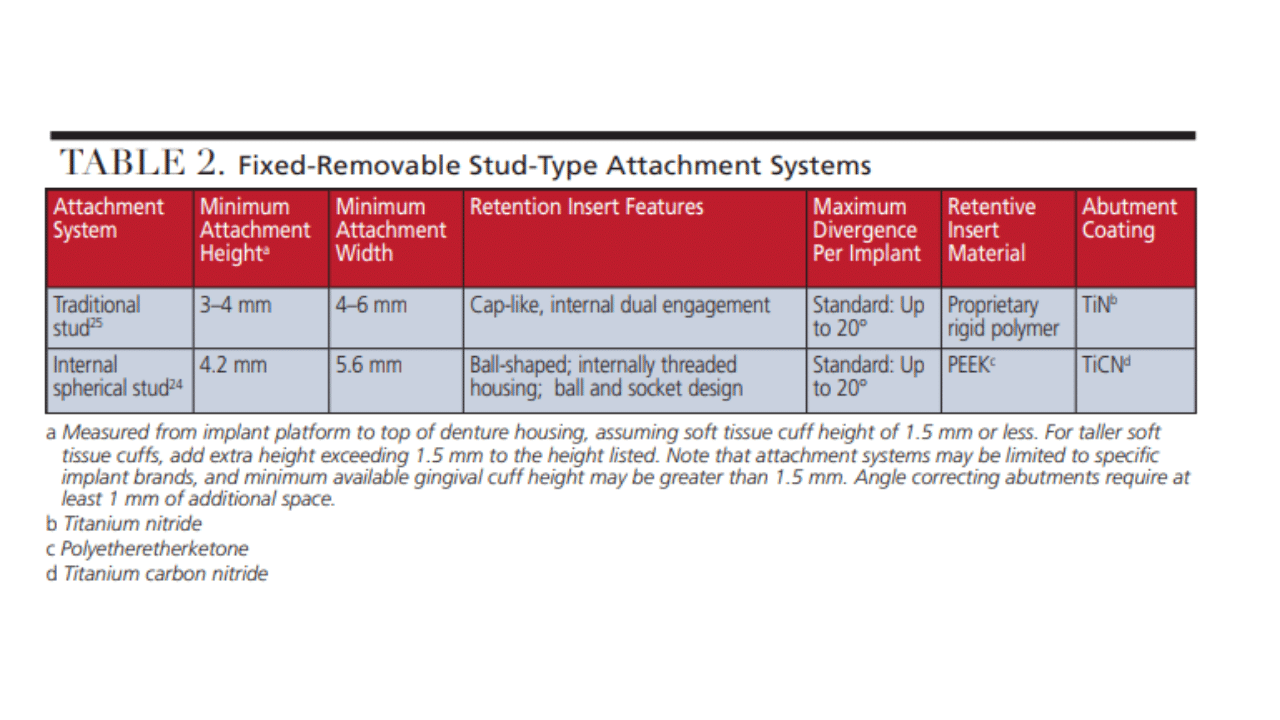
Making the screw access smaller so a hex driver can be used, designing externally engaging inserts, or utilizing a unique lateral access for the driver are some ways that manufacturers have sought to improve the functional life of these components.15,16,18 Manufacturers have utilized titanium nitride (titanium, argon and nitrogen) and, more recently, titanium carbon nitride coatings on abutments to reduce abrasive damage and wear.15,16,19 Traditional stud attachment dimensions are moderate, as compared to narrow profile abutments or the taller ball-type abutments, as described in Table 1.20–23
Contemporary attachment systems offer reduced vertical matrix and insert height, as well as a variety of insert materials composed of nylon, silicone, polyetheretherketone (PEEK), or polyetherketoneketone (PEKK). High-performance thermoplastic polymers, such as PEEK and PEKK, are increasingly used in retentive inserts to not only provide longer-lasting retention, but also create a “fixed-type” removable restoration. Fixed removable restorations use standard resilient attachment systems with stronger polymer components so the restoration is effectively “fixed” for the patient. The resulting cement-free prosthesis may only be removed by clinicians with a specialized armamentarium.24,25 While most systems require a metal housing to be picked up within the prosthesis, some resilient components can be placed without a housing.26
Regardless of the material used, the resilience of the standard insert in most attachment systems allows for 10° to 20° of implant divergence. Other systems rely on improved insert flexibility — such as that found in nylon and silicone attachment assemblies — to allow for increased angle correction. However, this comes at a cost to the longevity of the insert. Failure to replace worn inserts can result in wear and damage to the abutment and prosthesis.13 Only one system offers a prefabricated, one-piece angle correcting option with its 15° abutment. Angle correction accomplished via this abutment makes it more reasonable to use an insert composed of a high-performance polymer, such as PEEK, with the goal of less frequent replacement.16
Several systems allow for stock or custom-cast two-piece angle correction components.17,20,21,26 Alignment gauges can help clinicians determine which angle correcting abutments are needed. For two-piece angle correcting abutments, the first abutment (or base) is screwed into the implant, and the second angle correcting abutment is screwed into the base abutment. Some classical attachment systems require definitive cementation of the angle correcting abutment into the base abutment.18,20,21 Since the two-piece abutment is not intended to be removed for replacement, this design becomes problematic when abutments need to be replaced due to wear.
Alternative solutions, in the form of tighter-fitting retentive inserts or adjustable gold inserts, were developed to ameliorate worn abutments. Utilization of a two-piece abutment system for angle correction typically increases the vertical restorative space needed by at least 1.0 to 1.5 mm. As is true with classical ball-type attachments, contemporary ball or spherical abutments most often rely on attachment component positioning to correct any lack of implant parallelism during prosthesis fabrication or insertion.23,24,27–29 Devices such as spacers, paralleling jigs, or paralleling rods may be custom fabricated or purchased to facilitate correct positioning of the portion of the attachment housed within the prosthesis.27,30
EVALUATING RESTORATIVE SPACE
A critical factor in the provision of implant overdentures is ensuring adequate vertical restorative space. The classification system proposed by Ahuja and Cagna31 details the limited selection of overdenture attachments for cases with less than 12 mm of available space (when measured from the soft tissue crest of the residual edentulous ridge to the proposed occlusal plane). As a general rule for implant overdentures, 2 mm should be allocated for the denture base acrylic resin and 3 mm for the prosthetic teeth.32,33 Often indicated for implant overdentures, a metal framework would require another 1 mm of space.33 As evidenced by Table 1, the vertical space occupied by overdenture attachment systems ranges from 2.5 to 6 mm.
Prior to placing implants and fabricating definitive implant-supported prostheses, it is imperative to confirm the presence of adequate restorative space via prosthetically driven implant planning. The wax trial denture may be assessed for vertical space using handheld calipers (Figure 3A), or by making distance measurements in the three-dimensional implant planning software, following the dual scan protocol, as shown in Figure 3B. Furthermore, multiple planning software packages allow for the superimposition of virtual implant attachments to visualize angulation and restorative space relative to the implant platform. Performing a diagnostic work-up focused on esthetic and functional prosthetic tooth position, followed by prosthetically driven treatment planning using the dual cone beam scan protocol, allows for the optimization of implant and attachment positioning in overdenture therapy.34

Occlusal Considerations for Stud-Retained Overdentures

While there is minimal scientific evidence regarding occlusal schemes for overdentures, the occlusion is ultimately influenced by prosthesis stability, which is determined by the number and distribution of dental implants. The literature borrows concepts from conventional complete denture occlusion, and therefore these philosophies may be erroneous when directly applied to implant-borne restorations — which vary greatly from conventional dentures in terms of mechanics.35 When restoring one or both arches, centric relation is typically indicated. To enhance stability upon excursions and minimize excess occlusal force to the premaxilla area, lingualized balanced occlusion may be indicated for mandibular overdentures when opposing a conventional complete denture.36,37
When opposing at least 10 units of natural dentition/fixed restorations or a maxillary implant-borne prosthesis, two-implant mandibular overdentures should also exhibit a balanced occlusal scheme.37 In scenarios involving four or more well-distributed implants in each arch (as shown in Figure 4) or opposing a fixed complete denture or 10 units of natural dentition/fixed restorations, the overdenture should exhibit sufficient stability; thus, mutually-protected occlusion should be established.37,38 For cases involving the application of fixed removable attachments, manufacturer instructions recommend the distal cantilever should extend no more than one molar.24,25
CONCLUSION
With advanced technologies driving overdenture attachment development, the need to thoroughly understand indications and considerations for retention systems cannot be overstated. Given the plethora of systems to choose from, presurgical planning of both the implants and prosthetic components is of utmost importance to a predictably successful outcome.
References
- Kern JS, Kern T, Wolfart S, Heussen N. A systematic review and meta-analysis of removable and fixed implant-supported prostheses in edentulous jaws: Post-loading implant loss. Clin Oral Implants Res. 2016;27:174–195.
- Prasad S, Faverani LP, Santiago Jr JF, Sukotjo C, Yuan JC. Attachment systems for mandibular implant-supported overdentures: A systematic review and meta-analysis of randomized controlled trials. J Prosthet Dent. September 14, 2022. Epub ahead of print.
- Nagy U, Guedat C, Giannopoulou C, Schimmel M, Muller F, Srinivasan M. Microbiological evaluation of Locator Legacy attachments: a cross-sectional clinical study. Clin Exp Dent Res. 2019;5:476–484.
- Choi JW, Yun BH, Jeong CM, Huh JB. Retentive properties of two stud attachments with polyetherketoneketone or nylon insert in mandibular implant overdentures. Int J Oral Maxillofac Implants. 2018;33:1079–1088.
- Shah K, Yilmaz B, McGlumphy E. Fabrication of a mandibular implant-supported overdenture with a new attachment system: A review of current attachment systems. Int J Prosthodont. 2017;30:245–247.
- Baba NZ, Al-Harbi FA, AlRumaih HS, AlShehri A. A novel extended range attachment system to retain implant overdentures: A clinical report. J Prosthodont. 2019;28:3–9.
- de Souza RF, Jabbar AA, Jafarpour D, et al. Single-implant overdentures retained by a novel attachment: A mixed methods crossover randomized clinical trial. JDR Clin Trans Res. September 20, 2022. Epub ahead of print.
- Wichmann N, Kern M, Taylor T, Wille S, Passia N. Retention and wear of resin matrix attachments for implant overdentures. J Mech Behav Biomed Mater. 2020;110:103901.
- Srinivasan M, Kalberer N, Maniewicz S, Müller F. Implant overdentures retained by self-aligning stud-type attachments: A clinical report. J Prosthet Dent. 2020;123:6–14.
- The Glossary of Prosthodontic Terms. 9th Ed. J Prosthet Dent. 2017;117:e1–e105.
- Gotfredsen K, Wiskott A, Working Group 4. Consensus report — reconstructions on implants. The third EAO consensus conference 2012. Clin Oral Implants Res. 2012;23(Suppl 6):238–241.
- Scherer MD, McGlumphy EA, Seghi RR, Campagni WV. Comparison of retention and stability of implant-retained overdentures based upon implant number and distribution. Int J Oral Maxillofac Implants. 2013;28:1619–1628.
- Elsonbaty MA, Alshimy AM, Abdul-Monem MM, Neena AF. Evaluation of retention and wear of a titanium-formed stud overdenture attachment with different interimplant angulations after simulated clinical use: an in vitro study. J Prosthet Dent. 2022;128:205.e1–205.e10.
- Matthys C, Vervaeke S, Besseler J, De Bruyn H. Five-year study of mandibular overdentures on stud abutments: Clinical outcome, patient satisfaction and prosthetic maintenance — influence of bone resorption and implant position. Clin Oral Implants Res. 2019;30:940–951.
- Locator R-Tx Removable Attachment System. Available at: https://www.zestdent.com/media/pdf/Brochures/Zest-anchors/R-Tx%20Technique%20Manual_L8024-TM%20REV%20E.pdf. Accessed March 10, 2023.
- Straumann Novaloc Attachment System for Hybrid Dentures: Basic Information. Available at: https://www.straumann.com/content/dam/media-center/straumann/en/documents/brochure/technical-information/Ⳣ.115-en_low.pdf. Accessed March 10, 2023.
- Locator Attachment System Technique Manual. Available at: https://www.zestdent.com/media/pdf/L8030-TM_LOCATOR_TECH%20MANUAL_Rev_D.pdf. Accessed March 10, 2023.
- +CM Loc. The Anchor System. Available at: https://multimedia.getresponse.com/getresponse-B89z/documents/䴬.pdf?_ga=2.253099209.1736153229.1539195035-1412930966.1539195035. Accessed March 10, 2023.
- Del Castillo R, Chochlidakis K, Galindo-Moreno P, Ercoli C. Titanium nitride coated implant abutments: from technical aspects and soft tissue biocompatibility to clinical applications. A literature review. J Prosthodont. 2022;31:571–578.
- Stern ERA Implant Abutment. Available at: https://www.sterngold.com/amfile/file/download/file/쁢/product/롋/. Accessed March 10, 2023.
- Stern ERA Standard and Micro Overdenture. Available at: https://www.sterngold.com/amfile/file/download/file/붺/product/떧/. Accessed March 10, 2023.
- OT Equator: Direct attachment for implant retained overdenture. Available at: https://www.rhein83.com/en/portfolio/ot-equator/. Accessed March 10, 2023.
- Clix Ball Implant Abutment. Available at: https://www.preat.com/product-information/attachments/implant-abutments/clix-ball-implant-abutment. Accessed March 10, 2023.
- LOCATOR F-Tx Fixed Attachment System Technique Manual. Available at: https://www.zestdent.com/media/pdf/Brochures/Zest-anchors/za-fixed-attachment-L8031-locator-ftx-manual-tm.pdf. Accessed March 10, 2023.
- Locator Fixed Attachment System Technique Manual. Available at: https://zestdent-cms.s3.us-west-2.amazonaws.com/L8034-TM_LOCATOR+FIXED+Technique+Manual_FINAL4_NoCropsLowRes+(1).pdf. Accessed March 10, 2023.
- Stern SNAP and SNAP Angled Overdenture Abutments. Available at: https://www.sterngold.com/amfile/file/download/file/터/product/뵜/. Accessed March 10, 2023.
- Preci-Ball/Clix Paralleling Mandrel. Available at: https://www.ceka-preciline.com/cp_en/preci-ball-clix-paralleling-mandrel-1201-p. Accessed March 10, 2023.
- Sphero Block Implant Abutment (Micro 1.8mm). Available at: https://www.preat.com/product/sphero-block-implant-abutment-micro-1-8mm. Accessed March 10, 2023.
- ORA Complete Attachment. Available at: https://www.sterngold.com/ora-complete-attachment. Accessed March 10, 2023.
- Sphero Directional Rings. Available at: https://www.preat.com/product/sphero-directional-rings. Accessed March 10, 2023.
- Ahuja S, Cagna DR. Classification and management of restorative space in edentulous implant overdenture patients. J Prosthet Dent. 2011;105:332–337.
- Alsiyabi AS, Felton DA, Cooper LF. The role of abutment-attachment selection in resolving inadequate interarch distance: a clinical report. J Prosthodont. 2005;14:184–190.
- Vahidi F, Pinto-Sinai G. Complications associated with implant-retained removable prostheses. Dent Clin North Am. 2015;59:215–226.
- Resnik R. Dual CBCT scanning technique for completely edentulous arches. Dent Today. 2016;35:50–53.
- Rilo B, da Silva JL, Mora MJ, Santana U. Guidelines for occlusion strategy in implant-borne prostheses. A review. Int Dent J. 2008;58:139–145.
- Kim Y, Oh TJ, Misch CE, Wang HL. Occlusal considerations in implant therapy: clinical guidelines with biomechanical rationale. Clin Oral Implants Res. 2005;16:26–35.
- Rocha COM, Longhini D, Pereira RP, Lima ALO, Bonafé FSS, Arioli Filho JN. Masticatory efficiency in complete denture and single implant-retained mandibular overdenture wearers with different occlusion schemes: A randomized clinical trial. J Prosthet Dent. September 10, 2021. Epub ahead of print.
- Ismail HA, Yousief SA, Mahrous AI, Shaban AA, Azzeghaiby SN, Aljehani D. Clinical and radiographic evaluation of median lingualized occlusion in implant retained mandibular complete overdenture. J Int Oral Health. 2015;7(Suppl 1):5–8.
From Decisions in Dentistry. April 2023;9(4):26-29.

