
 UNDEFINED/ISTOCK/GETTY IMAGES PLUS
UNDEFINED/ISTOCK/GETTY IMAGES PLUS
Alternative Esthetic Clasp For Removable Partial Dentures on Maxillary Incisors or Canines
In restorative dental treatment, the round-rest, distal depression clasp offers an esthetic alternative for patients needing removable partial dentures.
A round-rest, distal depression (RRDD = R2D2) esthetic clasp for maxillary anterior teeth serving as removable partial denture (RPD) abutments was developed in 2001, with the first paper on the technique published in 2009.1 This article will provide an 19-year retrospective reflection on the R2D2 clasp, and present examples of clinical applications for this design.
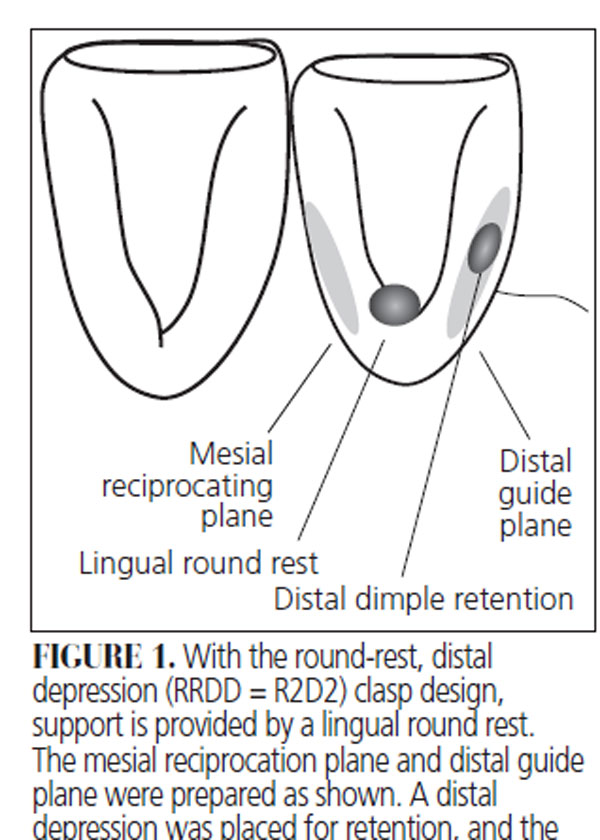
plane were prepared as shown. A distal depression was placed for retention, and the denture tooth was placed against the distal proximal contact.
Patients who require RPDs may find visible metal clasps objectionable, especially on maxillary teeth in the esthetic zone.2 Circumferential (Akers) clasps on maxillary incisors may not be esthetically acceptable to patients. Tooth-colored polymer clasps featuring acetyl and thermo-plastic resins are used for esthetics and ease of fabrication, but these are not readily adjustable and have not demonstrated durability. While extracoronal and intracoronal precision attachments can be esthetic, they are expensive and difficult to fabricate and maintain.3 In restorative dental treatment, I-bar and Akers clasps have been described,4–6 but patients may not like the esthetic outcome. While twin-flex and other esthetic clasps have been designed,7,8 and plunger attachments engaging a distal depression have been used,9 there may not be adequate space to place denture teeth. Rotational path designs for partial dentures10,11 can achieve excellent esthetic results for anterior tooth abutments, but are difficult to adjust.12 Similarly, lingual retention and the elimination of the visible facial clasp arm have been proposed,13,14 but this requires the restorative dentist to fabricate a crown with milled surfaces.15
A maxillary canine retainer with mesial groove reciprocation, mesiolingual rest, and distofacial depression retention has been described,16 but it is not applicable to maxillary incisors. As noted in Booth et al’s17 paper, “Esthetic Clasp Design for Removable Partial Dentures on Premolar Teeth” (available at decisionsindentistry.com), a cosmetic circumferential clasp for premolars with occlusal rest (CCCPO = C3PO) design was developed as an esthetic alternative to a conventional Akers clasp. The C3PO clasp was developed specifically for maxillary premolars to minimize the display of metal components in the esthetic zone (generally, the facial aspects of the mesiobuccal cusp of the maxillary first molar and teeth anterior to it). While the C3PO is appropriate for maxillary premolars and some maxillary canines, it is difficult to adapt to maxillary incisors.
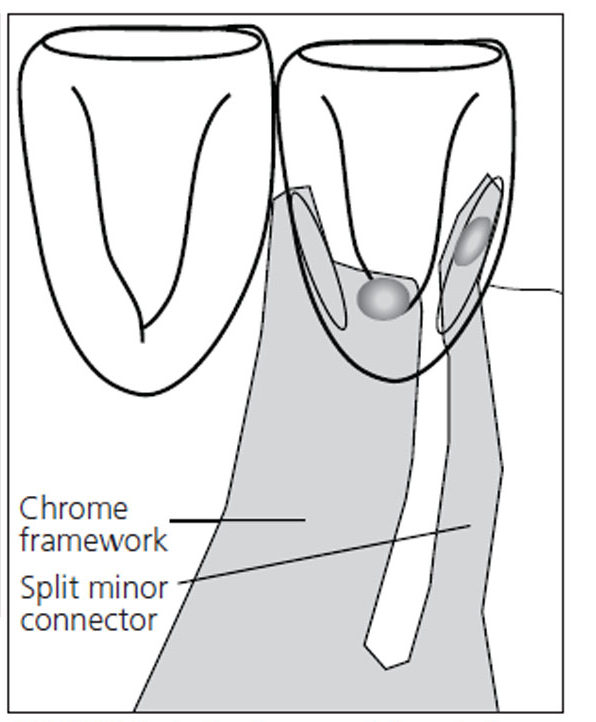
removed, the split minor connector will flex. When the removable partial denture is
completely seated, the distal clasp arm is
passive.
ALTERNATIVE ESTHETIC DESIGN
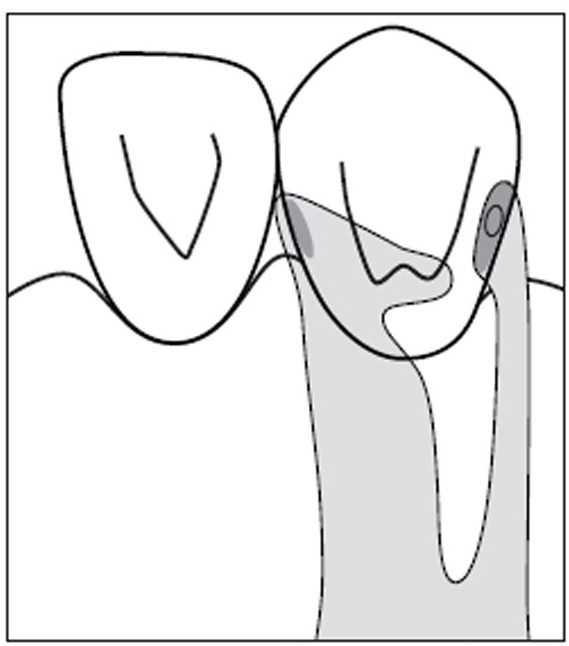
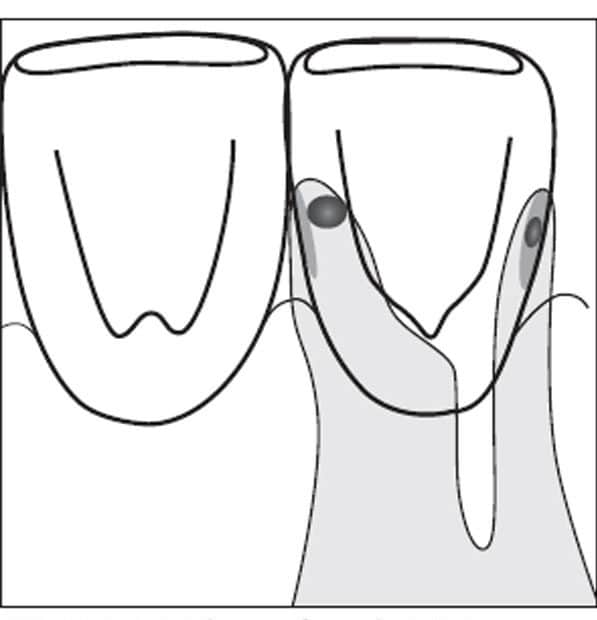
The R2D2 clasp was developed as an esthetic alternative to a conventional clasp for maxillary anterior teeth serving as abutments for an RPD. The R2D2 clasp was designed specifically for maxillary incisors or canines.1 Indications for this clasp include abutments for RPDs when esthetic demands are high, conventional and polymer clasps are cosmetically unacceptable, and the dentist wishes to minimize invasive procedures, thus avoiding the biologic and financial burden of a crown with an intra- or extracoronal attachment-retained RPD. The original design consists of a round rest at the cingulum, a split minor connector that engages a proximal undercut or a dentist-created depression (dimple) of 0.25 mm for retention of a 10-mm-long proximal cast clasp arm at the palatal major connector (Figure 1). The opposing minor connector goes over the prepared proximal marginal ridge into a round lingual rest or cingulum rest. The proximal aspect of the minor connector extends a partial plate of the lingual embrasure to provide reciprocation (if necessary). The occlusal rest is used for support. The bracing and encirclement by the mesiolingual plate and minor connector, the round or cingulum rest, and the distal proximal clasp arm into the dimple offer slightly less than 180-degree encirclement around the tooth, providing stability (Figure 2). Common variations include the use of a chevron-shaped cingulum rest (Figure 3), or moving the round rest to the marginal ridge further away from the edentulous span to help improve bracing and reciprocation (Figure 4).
reciprocation.
The clinical reports presented here will review use of the R2D2 clasp to eliminate the display of metal on the labial surface of maxillary incisors or canine teeth used as abutments for RPDs. This design is an alternative to an Akers clasp (Figure 5 and Figure 6), with the benefit of a good esthetic outcome. The R2D2 also serves as an alternative to a rotational path design, with the advantage of less technical complexity.
CLINICAL REPORT: PATIENT 1
A patient missing the maxillary left canine, first and second premolar, and first molar presented to the clinic at the University of the Pacific Arthur A. Dugoni School of Dentistry. The patient did not want implant-supported restorations. Prior to RPD therapy, the patient’s chief complaint, and medical, dental and social history were reviewed and determined noncontributory. Head and neck, paraoral, oral and radiographic evaluations were done, with no significant findings. The patient had undergone caries risk assessment, periodontal, restorative soft- and hard-tissue evaluations, and no clinical or radiographic caries were detected. Adjunctive periodontal therapy and evaluation of initial therapy were completed, with prescription of a regular interval for periodontal evaluation and maintenance.

denture with Akers clasps on the incisors. This
clasp design may not be esthetically
acceptable for some patients.
The patient had an existing maxillary all-acrylic-resin RPD that was determined to be lacking in support, stability and retention. Financial considerations were a major concern. The patient also did not want to display any metal clasps on teeth visible in the esthetic zone. Four options for an RPD were presented: a crown with precision attachment RPD, conventional Akers clasp RPD, rotational path RPD, or an R2D2 design. The patient chose the R2D2 design for esthetic reasons and ease of placement. The diagnostic casts were surveyed and a maxillary RPD was designed, using a broad palatal strap as the major connector, occlusal rests and embrasure clasps on the molars on the right side, an R2D2 clasp on the maxillary left lateral incisor, and an Akers clasp on the maxillary left second molar.

with a maxillary removable partial denture
and R2D2 clasps on the lateral incisors. This
clasp design may be acceptable to patients
who place a high priority on esthetics.
TOOTH PREPARATION
The guide planes on the distal of the lateral incisor and mesial of the second molar abutments were prepared using a parallel chamfer tip carbide bur. The second molar mesial marginal ridge was lowered 1.2 mm for the minor connector into the occlusal rest, which was placed with a No. 8 round bur. The contralateral molars were prepared for an embrasure clasp with 1.5 mm occlusal clearance and a 2.5 mm mesial distal dimension (lowering the marginal ridges in the interproximal embrasure between the second premolar and first molar); the occlusal rests were also refined. All occlusal rests were evaluated for minimum 1.5 mm occlusal clearance, and the areas to receive the retention clasp arms were evaluated for adequate height of contour. If the required undercut (0.25 mm) was not available, tooth modification was performed by either odontoplasty or preparation of a depression or dimple to create an undercut with a No. 6 round bur. A ball burnisher was placed in the round rest seat and dimple depression to verify adequate preparation.

edentulous.
On the left lateral incisor, a round cingulum rest was prepared with a #4 round bur to a depth of 0.75 mm. The reciprocating plane on the mesiolingual surface of the incisor was prepared with a thin parallel chamfer tip carbide bur from the mesiolingual line angle, and stopped just short of the mesial proximal contact. The guiding plane on the distolingual surface of the tooth was prepared from the distolingual line angle, stopping just short of the distal proximal contact area. In the middle of this surface, a distal depression (dimple) 0.5 mm deep was prepared with a No. 4 round bur, 1 mm above the gingival margin and 1 mm lingual to the proximal contact (Figure 7). A ball burnisher was placed in the round rest seat and distal depression to verify adequate preparation.

DENTURE FABRICATION
After completion of oral preparations, an irreversible hydrocolloid impression was made. The definitive cast was prepared in dental stone ISO type 5, tripodized, surveyed and designed. The following dimensions were specified to the laboratory for the R2D2 appliance: The minor connector and mesiolingual plate were 3 mm wide mesiodistally and 0.5 mm thick occlusogingivally, respectively, to provide adequate rigidity. Distal to the minor connector, a 1 mm wide split was placed in the casting. A proximal clasp (2 mm wide tapering to 1 mm) engaged the distal depression. This small minor connector was 10 mm from the major connector to the center of the depression to allow adequate flexibility (Figure 8). The flexibility of the minor connector engaging the distal depression can be altered by increasing its length or by thinning the dimensions of the arm. A cast chrome RPD framework was fabricated, tried intraorally and adjusted. The retentive values of this clasp design were comparable to an Akers clasp or wrought wire.17–19 After maxillomandibular jaw relation records were completed, denture teeth were arranged and evaluated intraorally. Next, the denture base was processed and finished.

After the denture was inserted, the patient was followed for routine maintenance for 19 years, and reported good service from the R2D2 RPD (Figure 9). The patient was pleased with the functional and esthetic outcome from the prosthesis.
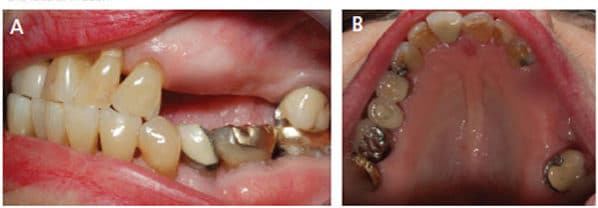
CLINICAL REPORT: PATIENT 2
A patient missing the maxillary left first and second premolars, and first molar presented to the University of the Pacific Arthur A. Dugoni School of Dentistry clinic (Figures 10A and 10B). The RPD for this patient was generally similar to Patient 1. The molars were prepared for conventional Akers and embrasure clasps, while the canine received an R2D2 with the round rest prepared in the mesial marginal ridge (Figure 4). Compared to a cingulum round rest location, the major advantage is improved reciprocation and bracing. The patient was followed for 16 years and was pleased with the functional and esthetic outcome (Figures 11A and 11B).

CLINICAL REPORT: PATIENT 3
A patient missing bilaterally the maxillary canine, first and second premolar, and first molar presented to the University of the Pacific Arthur A. Dugoni School of Dentistry clinic. The existing RPD featured Akers clasps on the lateral incisors (Figures 12A and 12B), and the patient wanted a more modern design. The new RPD was designed with two R2D2 clasps, two Akers clasps and a horseshoe palatal major connector (Figure 13). The contrast between the previous all-Akers RPD and newer Akers with R2D2 design was remarkable (Figures 14A through 14D).

DISCUSSION
These case reports were culled from more than 500 R2D2 clasp assemblies made since 2001 in the predoctoral student clinic at the University of the Pacific Arthur A. Dugoni School of Dentistry. Patients were generally pleased with the esthetic and functional outcome. Students and instructors appreciated the conservative nature of tooth preparation and minimally invasive restorative services compared to surveyed, milled crown or precision attachments. Unlike rotational path RPDs, retention of the R2D2 clasp is adjustable.

The R2D2 clasp is a little more technically demanding than an Akers cast circumferential clasp. The dentist must plan the design of the RPD very carefully and perform detailed tooth modifications with a clear understanding of clasp function. The laboratory must also fabricate the framework with care and precision, because any technical deviation may cause loss of retention. The R2D2 design also allows more conservative tooth preparation than other esthetic clasp assemblies that require milled crown fabrication and precision attachment-retained RPDs.20–30
While this clasp can achieve the recommended minimum 180-degree encirclement of the abutment, the R2D2 clasp is not recommended for abutment teeth with excessive mobility. In addition, because there is no stress release, this design is not recommended as the terminal abutment for a distal extension RPD. Rather, the R2D2 is an alternative to the Akers or rotational path design, with the advantage of improved esthetics.

SUMMARY
As detailed in this report, the R2D2 is an esthetic clasp for maxillary incisors and canines. To recap, the clasp assembly consists of a round rest or cingulum rest on the lingual surface of the abutment tooth, and a short bracing plate or minor connector opposite the edentulous span for reciprocation. It also uses a 10-mm-long clasp engaging a proximal undercut or dimple for retention. Featuring adjustable retention, the design satisfies the criteria for esthetics, retention, support and stability for a tooth-borne maxillary RPD.
Acknowledgements: The authors thank Jeffrey P. Miles, DDS, an associate professor at the University of the Pacific Arthur A. Dugoni School of Dentistry, for the illustrations in Figure 3 and Figure 4.
Figures 1, 2, 7, 8 and 9 reproduced from Tran C, LaBarre E, Landesman HM. A removable partial denture using an esthetically designed round-rest distal clasp on maxillary anterior abutment teeth: a clinical report. J Prosthet Dent. 2009;102:286–289. Reproduction was approved by the Editorial Council for The Journal of Prosthetic Dentistry on May 14, 2019.
REFERENCES
- Tran C, LaBarre E, Landesman HM. A removable partial denture using an esthetically designed round-rest distal clasp on maxillary anterior abutment teeth: a clinical report. J Prosthet Dent. 2009;102:286–289.
- Hansen CA, Iverson GW. An esthetic removable partial denture retention for the maxillary canine. J Prosthet Dent. 1986;56:199–203.
- Becerra G, MacEntee M. A classification of precision attachments. J Prosthet Dent. 1987;58:322–327.
- Krol AJ. Clasp design for extension-base removable partial dentures. J Prosthet Dent. 1973;29:408–415.
- Kratochvil FJ. Influence of occlusal rest position and clasp design on movement of abutment teeth. J Prosthet Dent. 1963;13:114–124.
- Eliason CM. RPA clasp design for distal extension removable partial dentures. J Prosthet Dent. 1983;49:25–27.
- Belles DM. The Twin-Flex clasp: an esthetic alternative. J Prosthet Dent. 1977;77:450–452.
- McMillan AS, Hunter N. An esthetic denture clasp for maxillary canine teeth. J Prosthet Dent. 1997;78:330.
- Donovan TE, Derbabian K, Kaneko L, Wright R. Esthetic considerations in removable prosthodontics. J Esthet Restor Dent. 2001;13:241–253.
- King GE. Dual-path design for removable partial dentures. J Prosthet Dent. 1978;39:392–395.
- Krol AJ, Jacobson TE, Finzen FC. Removable Partial Denture Design: Outline Syllabus. 5th ed. San Rafael: Indent; 1999:73–91.
- Donovan T. Use of the rotational path removable partial denture concept in a Kennedy Class II patient: a case report. J Esthet Restor Dent. 2008;20:294–298.
- Pardo-Mindan S, Ruiz-Villandiego JC. A flexible lingual clasp as an esthetic alternative: a clinical report. J Prosthet Dent. 1993;69:245–246.
- DeRossi A, Albuquerque RF Jr, Bezzon OL. Esthetic options for the fabrication of removable partial dentures: a clinical report. J Prosthet Dent. 2001;86:465–467.
- Brudvik JS, Palacios R. Lingual retention and the elimination of the visible clasp arm. J Esthet Restor Dent. 2007;19:247–254.
- McCartney JW. The MGR clasp: an esthetic extracoronal retainer for maxillary canines. J Prosthet Dent. 1981;46:490–493.
- Booth M, Tran C, Noble WH. Esthetic clasp design for removable partial dentures on premolar teeth. Decisions in Dentistry. 2019;5(7):36–39.
- Frank RP, Nicholls JI. A study of the flexibility of wrought wire clasps. J Prosthet Dent. 1981;45:259–267.
- Frank RP, Brudvik JS, Nicholls JI. A comparison of the flexibility of wrought wire and cast circumferential clasps. J Prosthet Dent. 1983;49:471–476.
- Ahmad I, Sherriff M, Waters NE. The effect of reducing the number of clasps on removable partial denture retention. J Prosthet Dent. 1992;68:928–933.
- HajjaJ MS. Modified equipoise clasp: an esthetic option for removable dental prostheses. J Prosthodont. 2019:28:724–727.
- Pheonix R, Cagna D, DeFereest C. Stewart’s Clinical Removable Partial Prosthodontics. Available at: http/://www.quintpub.com/PDFs/bo_k_preview/B4856.pdf. Accessed March 6, 2020.
- Reagan SE, Rold TM. Practical, esthetic options for retention of removable partial dentures: a case report. Quintessence Int. 1996;27:333–340.
- Budtz-Jorgensen E, Bochet G, Grundman M, et al. Aesthetic considerations for the treatment of partially edentulous patients with removable dentures. Pract Periodontics Aesthet Dent. 2000;12:765–772.
- Khan SB, Geerts GA. Aesthetic clasp design for removable partial dentures: a literature review. SADJ. 2005;60:190–194.
- Goodman JJ. The Equipoise removable restoration. Trends Tech Contemp Dent Lab. 1991;8:45–48.
- Hundal M. Esthetic cast direct retainers for distal extension removable partial dentures. J Oral Hygiene Health. 2014;2:134.
- de Kok M, Thomas CJ. Clinical study of the modified Equipoise clasp. Aust Prosthodont J. 1990;4:53–57.
- Brudvik JS, Reimers D. The tooth-removable partial denture interface. J Prosthet Dent. 1992;68:924–927.
- Brudvik JS, Shor A. The milled surface as a precision attachment. Dental Clin North Am. 2004;48:685–708.
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. April 2020;6(4):22–25.
