

Advantages of Advanced Magnification
High-tech magnification systems, including dental operating microscopes and three-dimensional digital stereomicroscopy, provide ergonomic and clinical benefits in the provision of care.
The ability to accomplish the goals of dental care lies within the clinician’s expertise in balancing the art and science of dentistry. Regardless of the discipline, the most important aspect of treatment is the capacity to properly diagnose conditions that require intervention to restore health. Once an accurate diagnosis is made, a clinician must utilize a combination of sight and proper physical orientation to deliver effective care.
One aspect that is often overlooked involves the limitations and complexity of working in a fixed and distorted position. When operating within the confines of the oral cavity, many biomechanical issues are encountered. These challenges often lead to surgical fatigue of the muscles of the head, neck, shoulders and eyes. This article will discuss advances in technology that improve a clinician’s ability to operate in the complex oral environment with improved sight, orientation and ergonomics. Among other specialties, surgical microscopes have long been used in endodontics to aid in both root canal therapy and root end surgical care. Within endodontics, magnification has been shown to increase success in locating canals,1 assist in detecting fracture lines,2 and improve surgical techniques.3 Research evaluating the benefits of using loupes in restorative dentistry demonstrates that 4x to 6x magnification provides better visual acuity for diagnosis and treatment than 2.5x magnification.4 Thus, within all fields of dentistry, research shows that increased magnification improves clinical diagnosis and aids treatment — which ultimately supports better outcomes.
ERGONOMICS AND HEALTH
Ergonomic issues continue to plague medical and dental providers. With the realization that dentists can spend more than 60,000 lifetime hours working in tense and distorted positions, it is understandable that musculoskeletal disorders may arise.5 Even for those who grasp the importance of ergonomics, providers are subject to the postural limitations of the head and neck when operating in the oral environment.
A recent randomized clinical controlled study focusing on scaling of the dentition determined that instruction and education have a positive correlation with improved ergonomics.6 The medical profession is subject to the same ergonomic challenges, with one study stating that ergonomic issues among laparoscopic surgeons have reached an “epidemic” level, with 87% of surgeons describing neck, back and hand pain.7 Correlative studies outside of dentistry have investigated fixed positions with participants holding a steady state while looking at a smartphone. The researchers found that in a maximum flexure position — similar to looking into the mouth during dental care — the splenius capitis and upper trapezius muscles were subject to considerable fatigue.8
Shoulder fatigue associated with static posture was evaluated again during a laparoscopic procedure and measured against a surgeon’s cognitive ability. It was found that muscular fatigue involving the head and shoulders due to static posture considerably decreased operators’ cognitive ability.9 Research within both the medical and dental fields reveals that maintaining an ergonomic position of the head and neck is essential not only for providers’ health, but also for the benefit of patient care.
While the use of conventional Galilean loupes magnifies the field of view and helps improve the clinician’s working position, research suggests there may be ergonomic benefits in using the dental operating microscope. A recent study evaluated prosthodontic residents utilizing 2.5x loupes or an 8x ocular microscope. An analysis of the subjects’ trunk, head, neck and elbow position demonstrated “significant” improvement in clinical posture when using the microscope.10
DIGITAL STEREOMICROSCOPY
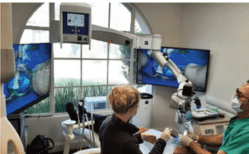
Unlike a standard dental operating microscope, a digital stereomicroscope does not require clinicians to look through the oculars; rather, the device depicts a three-dimensional (3D) view of the surgical field on a large-screen monitor (Figure 1). However, the 3D view requires the operator to wear polarized glasses (similar to the display technology used for most 3D movies). This approach offers several advantages:
- The dentist can work “heads up” — that is, in a comfortable, neutral seated position. The operator learns to manipulate his or her tools by watching the screen, rather than in a bent-over, rigid position.
- The dental assistant can immediately see what the dentist is seeing, either on the same screen or on an auxiliary monitor.
- The patient can also view the live procedure (should the dentist desire this).
- As a computer-based visualization system, the digital platform makes possible the development of tools (i.e., applications) that have the potential to support better surgical outcomes and more efficient care. Potential applications include stereoscopic documentation, image enhancement, fluorescence, teledentistry, and real-time comparison to presurgical 3D cone beam computed tomography models.
The term digital refers to the type of video camera embedded in the system. The surgical field is captured using digital image sensors and then passed on to a processor or computer for real-time display, recording or transmission. A stereoscopic camera generally has two image sensors: one to capture the left image, and one for the right. The nomenclature “digital stereomicroscope” helps distinguish this type of visualization from optical stereomicroscopes, in which the user’s eyes must be placed close to the eyepieces.
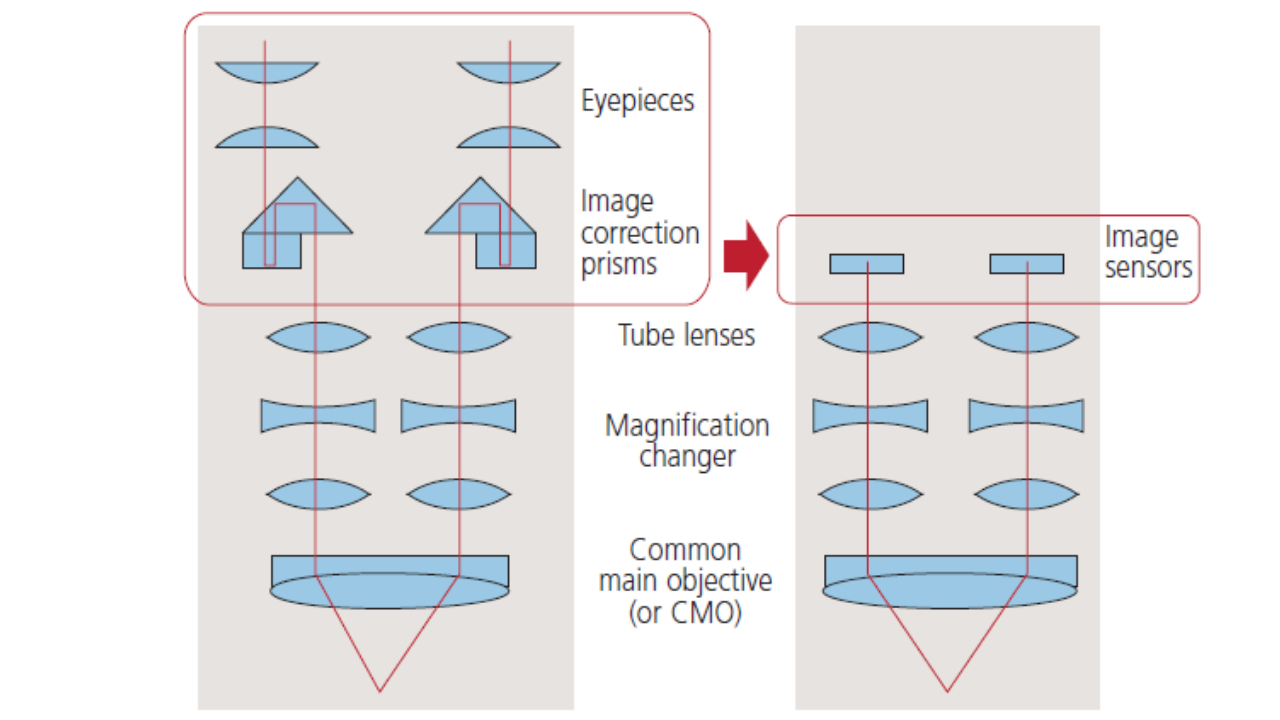
In digital stereomicroscopy, the two eyepieces are replaced by the two image sensors — as illustrated in Figure 2, which also shows the optical design of a common type of dental microscope (called common main objective, or CMO). The sensors are either embedded into the head (an integrated design) or contained in a stereoscopic camera that replaces the eyepiece module of an existing microscope (i.e., an add-on design).
In either case, two images come out of the head or camera: a left-eye and a right-eye view — the same two images the viewer would see looking through the eyepieces. Because of the optical design of the CMO microscope, the perspectives of the two views are different. (The left and right images are taken from the two sides of the CMO lens.) This is analogous to normal stereoscopic vision, in which humans “see in stereo” due to the difference in perspective between the two eyes.
These two images are transmitted to a stereoscopic 3D display, of which there are various types. Most dental operatories and surgical operating rooms are equipped with the flat-panel monitor and polarized glasses previously described.
IMAGE QUALITY IN A DIGITAL STEREOMICROSCOPE
Although this technology was invented in the 1990s,11 it was first introduced in the surgical marketplace in 2005 and has been successfully used for ophthalmic, neuro, vascular, spine and otolaryngology surgeries. In addition to its use for surgical education (to produce instructional 3D videos, for example), many surgeons work from the screen, even for procedures that require extremely high-res image quality, such as retinal surgery.12

Digital stereomicroscopy is also used in dentistry, and several companies have marketed devices. Figure 1 shows a clinician working on a dental microscope where a stereo camera module has replaced the eyepieces. In Figure 3, the clinician is using an integrated microscope. Note that in both cases the doctor is practicing with the head upright.
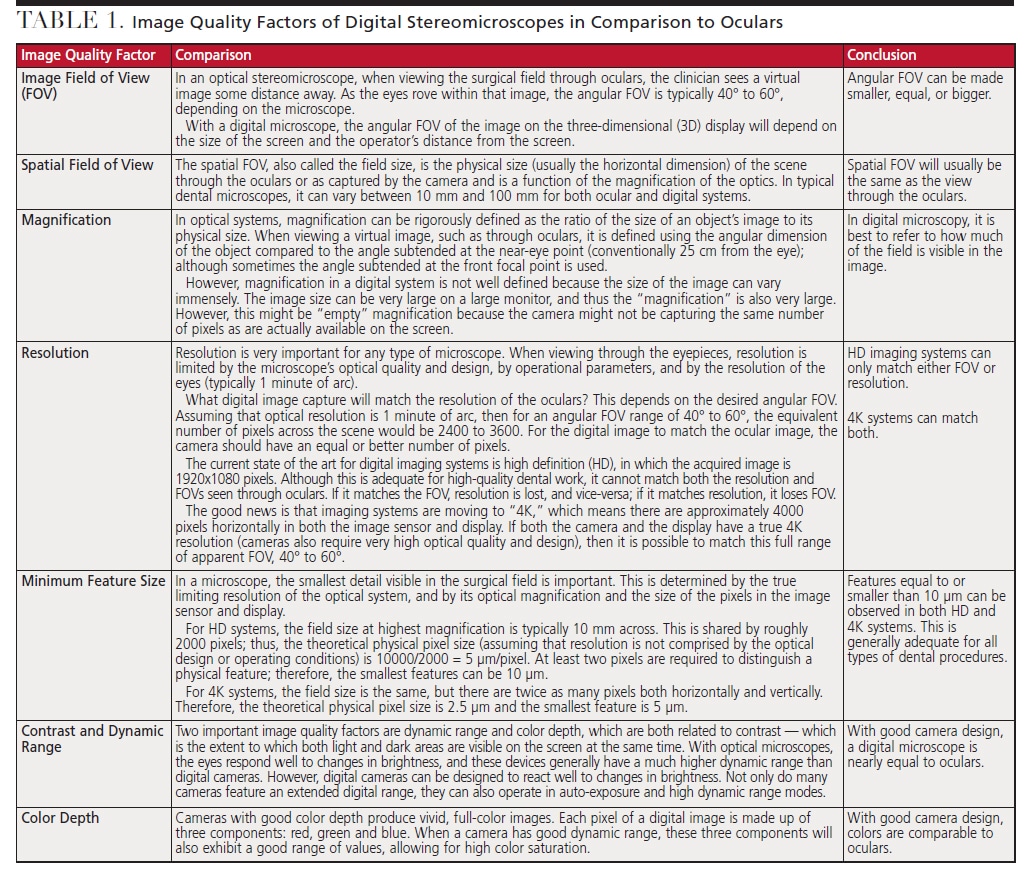
Of course, this technology would not be acceptable if the view of the surgical field on the stereoscopic 3D display was inadequate for clinical practice. As summarized in Table 1, image quality is determined by a number of factors. (The table’s comparison of the digital image with the view through the oculars results from studies by the second author using an add-on type of digital stereomicroscope.)
ADVANTAGES OF HEADS-UP PRACTICE
As previously discussed, a chief benefit of this technology is that it allows clinicians to maintain an ergonomically neutral operating position. With the understanding that fatigue of any kind has quantitatively been demonstrated to affect cognitive ability, musculoskeletal stress either during a procedure or throughout the day may compromise surgical performance and, thus, outcomes.
Stereomicroscopy, first developed for neuro and ophthalmic surgery, offers a noticeable ergonomic advantage over other magnification technologies. A 2012 study quantitatively measured posture using a traditional optical microscope and two-dimensional (2D) and 3D heads-up displays. The biomechanical analysis of the neck position revealed the traditional microscope resulted in neck joint loads twice as high as the heads-up displays in both 2D and 3D microscopes.13 The literature appears to show that a heads-up position improves clinical posture and decreases muscle strain on the head and neck. A secondary question of similar, if not higher, priority relates to the clinician’s ability to adjust from an ocular image to a display-based 3D system. A feasibility study evaluating a see-through stereoscopic head-mounted display system used by 15 otolaryngology surgeons found the see-through stereoscopic head-mounted image did not result in greater eye fatigue than an ocular microscope.14
FUTURE OF MAGNIFICATION TECHNOLOGY
The advantage of technology is that it continually allows for new applications of standard principles that change the delivery of care. Visual acuity is a clinical necessity, but with a digital 4K image the potential exists to manipulate a standard ocular view by providing new sources of real-time feedback to aid in both diagnostic and surgical techniques. By merging cone beam technology with a digital stereomicroscope image, a clinician could potentially have an overlay of the surgical field on the same display, creating a digital surgical guide.
Video capture of the surgeon’s view has the potential to provide a live 3D feed to clinicians viewing remotely, who could then offer real-time consultation. The apertures of the cameras allow for ideal visualization under different lighting scenarios, including increased brightness to the field during visualization and decreased light during composite curing or when using light-sensitive materials. These cameras could be adapted to visualize light-sensitive markers that could be applied to the surgical field and allow for caries detection or identification of pathogenic biological markers. As scientific understanding of virology and transmission evolve, a heads-up display may allow for the separation of the patient and clinician to decrease exposure in the surgical space. These are just a few examples of how digital stereomicroscopy may change the landscape of not only oral care, but the provision of healthcare in general.
KEY TAKEAWAYS
- Within all fields of dentistry, research suggests that magnification improves clinical diagnosis and aids treatment — which ultimately supports better outcomes.
- Muscular fatigue of the head and shoulders has been shown to decrease operators’ cognitive ability.9
- In digital stereomicroscopy, the two eyepieces are replaced by the two image sensors, as illustrated in Figure 2.
- Unlike a standard dental operating microscope, a digital stereomicroscope does not require clinicians to look through the oculars; rather, the device depicts a three-dimensional (3D) view of the surgical field on a monitor.
- However, the 3D view requires the operator to wear polarized glasses (similar to the display technology used when viewing most 3D movies).
Michael J. Tulkki, DDS, MS, has no commercial conflicts of interest to disclose. Michael Weissman, PhD, discloses that he is CEO, chief technology officer, and a stockholder of SB3D Technologies in Santa Barbara, California
REFERENCES
- De Carvalho M, Zuolo M. Orifice locating with a microscope. J Endod. 2000;6:532–534.
- Mines P. Use of the microscope in endodontics: a report based on a questionnaire. J Endod. 1999;25:755–758.
- Kim S. Modern endodontic surgery concepts and practice: a review. J Endod. 2006;32:601–623.
- Doppalapudi NB. Benefits of utilization of magnification in dentistry: a review. Dent Res Oral Health. 2020;3:121–128.
- Gupta A. Ergonomics in dentistry. Int J Clin Pediatr Dent. 2004;7:30–34.
- De Santana Sampaio Castilho AV, Crosato EM, De Carvalho Sales-Peres SH, et al. Effectiveness of ergonomic training on decreasing awkward postures during scaling procedures: a randomized clinical trial. Int J Environ Res Public Health. 2021;18:11217.
- Park A, Lee G, Seagull FJ, Meenaghan N, Dexter D. Patients benefit while surgeons suffer: an impending epidemic. J Am Coll Surg. 2010;210:306–313.
- Choi J-H, Jung M-H, Yoo K-T. An analysis of the activity and muscle fatigue of the muscles around the neck under the three most frequent postures while using a smartphone. J Phys Ther Sci. 2016;28:1660–1664.
- Stephenson M, Ostrander AG, Norasi H, Dorneich MC. Shoulder muscular fatigue from static posture concurrently reduces cognitive attentional resources. Hum Factors. 2020;62:589–602.
- Liu XQ, Liao Y, Yang Y, Zhou JF, Tan JG. Effects of loupes and microscope on the prosthodontist’s posture from ergonomic aspects. Beijing Da Xue Cue Bao Ti Xue Ban. 2020;52:948–951.
- Rod SR. Stereoscopic On-Screen Surgical Microscope Systems. Available at: https://www.freepatentsonline.com/﹊.html. Accessed April 11, 2023.
- Eckardt C, Paulo EB. Heads-up surgery for vitreoretinal procedures: An experimental and clinical study. Retina. 2016;36:137–147.
- Yu D, Sackllah M, Woolley C, Kasten S, Armstrong T. Quantitative posture analysis of 2D, 3D, and optical microsurgery tasks. Work. 2012;41(Suppl 1):1944–1947.
- Kim CH, Ryu SY, Yoon JY, et al. See-through type 3D head-mounted display based surgical microscope system for microsurgery: A feasibility study. JMIR Mhealth Uhealth. 2019;7:e11251.
From Decisions in Dentistry. May 2023;9(5):10,13-14,16.
