

Addressing Substance Use in Modern Dental Practice
Dentists can integrate evidence-based screening tools to detect substance use disorders, fostering communication and offering referrals to addiction treatment specialists
PURCHASE COURSE
This course was published in the October 2023 issue and expires October 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
In modern dental settings, dentists treat patients with a past and current history of illicit drug use, abuse, or substance use disorder (SUD). Dental patients with a history of substance use (both historical and current) differ significantly from those who are not users. Therefore, treating an actively drug-addicted patient differs from treating a patient who uses or abuses substances regularly but does not present with clinical signs of addiction.
This course was published in the October 2023 issue and expires October 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 130
Educational Objectives
After reading this course, the participant should be able to:
- Discuss the significance of recognizing and addressing substance use disorders (SUDs) in a dental setting.
- Identify evidence-based screening tools for identifying SUDs.
- Describe the public health approach of screening, brief intervention, and referral to treatment in dental practice.
Additionally, addicted patients, patients who developed tolerance due to frequent use, and patients who are recreational users differ significantly from nonusers due to the medical/emotional/behavioral/personality issues of patients with addiction.
Substance use has become widespread across all population groups, regardless of ethnicity, educational level, cultural background, or socioeconomic status. It is a global epidemic. According to Viswanath et al,1 about 8% of Americans and 20% of the global population have SUDs.
While patients with addiction and substance-tolerant patients often exhibit poor general health and poor nutrition, the evidence of ongoing dental issues frequently becomes clinically evident prior to more significant medical problems becoming apparent. These issues include worsening oral hygiene and clinically evident effects of drugs on the oral mucosa, gingiva, and dentition, as well as ignoring one’s dental health.
The dental profession responded to substance use and abuse among dental patients and managing patients with SUDs in the clinical setting with the publication of “Statement on Provision of Dental Treatment for Patients with Substance Use Disorders,” by the American Dental Association (ADA) in 2005.2
As primary healthcare providers, dentists need to know how to use modern, evidence-based screening tools to identify SUDs in dental practice, encourage patients to seek addiction help, and offer appropriate referrals to proper addiction treatment specialists.3
Moreover, to ensure that dental care is delivered safely and predictably, dental providers must identify chemically dependent patients in order to modify dental treatment plans to address substance use issues. Dentists should inquire whether patients have any history of active or historic substance use or are recovering from chemical dependency so treatment can be modified to prevent possible relapse.
Finally, dentists need to recognize patients who are doctor-shopping and present with made-up symptoms to secure narcotic analgesic prescriptions. To meet such challenges, dentists and their staff must be trained in how to handle such delicate and distressing situations. An application of practice-wide comprehensive substance use screening processes and implementation of controlled substance prescription policies, as well as pain management contracts with existing patients will help dental practitioners to address these situations.
Chemical dependency is a disease and, as such, the management of chemical dependency in dental settings requires certain adjustments just like any other medical condition that affects dental care.4
Focus on Substance Use and Misuse
The dental setting offers a unique opportunity for screening for substance misuse through patient medical history forms, intake interview, recare visits, and medical history updates. According to Parish et al,5 oral health professionals who integrated substance misuse screening into their professional responsibilities were more inclined to inquire about misuse with their patients (85.8%), as opposed to those who did not incorporate such screening into their role (68.2%).
Dentists must be aware of all the medical conditions and medications related to a patient’s health. The biologic or psychotropic effects of illicit drugs on dental anesthetics and therapeutics cannot be ignored, especially when prescribing narcotics. To implement substance use and misuse screening in the dental setting, dentists must rely on an evidence-based, clinically tested set of professionally developed diagnostic tools.
Validated Screening Tools
Several validated screening and assessment tools are available that are evidence-based, comprehensive, and well-suited for use in dental settings. These tools can be used as part of an initial clinician-led interview or as a self-assessment tool that allows patients to recognize they may have a substance use problem. Notably, many screening tools, while designed to be self-administered by an adult patient, are not intended to guide self-assessment or take the place of a healthcare provider’s clinical judgment. Instead, they are designed to provide clarity in determining if the patient has substance use problems and, hopefully, serve as a wake-up call to direct the patient toward receiving professional help.
These tools are organized by substance type, patient age, and administration method and can be used with patients from adolescence to adulthood, allowing dental practitioners to find the right tool for the practice.6
The tobacco, alcohol, prescription medication, and other substance use (TAPS) tool generates a risk level for each substance class. TAPS is designed for use with adults and combines screening and brief assessment of past 90-day problematic use into one tool. TAPS can be self-administered or completed at the clinician-led interview. TAPS is available online for self-administration.7
TAPS combines screening and brief assessment for commonly used substances focusing on the frequency of substance use in the past 12 months, and facilitates a brief assessment of the past 3 months of problem use. TAPS eliminates the need for multiple screening and lengthy assessment tools.
The drug abuse screening test (DAST-20) is a 20-item, yes/no self-report instrument designed to provide a brief clinical screening and treatment evaluation tool; it can be used with adults and older youth. This tool uses a series of questions focusing on the patient’s potential involvement with drugs other than alcohol. The questionnaire includes any nonmedical drug use, including marijuana, valium, cocaine, amphetamines, lysergic acid diethylamide (LSD), and heroin. Additionally, DAST refers to the use of prescribed or over-the-counter drugs in excess of the recommended dosage, examining substance misuse rather than prescribed use.8
The DAST-10 is a shorter version of the DAST-20. Even though DAST-10 is intended to take less time, the abbreviated version correlates exceptionally well with the longer scale despite the smaller volume of information required to complete it. In addition, each item on the DAST-10 focuses on involvement with drugs other than alcohol, such as nonmedical use of drugs and use of prescribed medications in excess of the recommended dose.
The Michigan alcohol screening test (MAST) is another popular tool consisting of 25 simple yes/no questions. The MAST questionnaire is considered the most effective tool in identifying dependent drinkers with up to 98% accuracy.
MAST focuses on the patient’s self-appraisal of social, family-related, and vocational problems characteristic of heavy drinking and assesses the risks associated with drinking patterns, neglect of responsibilities, loss of control, and other topics. As in previous scenarios, MAST has shortened and modified versions published over time, including the Brief MAST, SMAST, and Mm-MAST.9
All versions of MAST can be used as a part of clinician interviews or as a self-assessment tool. While self-scoring is an excellent mode of use, the test should not be used to self-diagnose.10
The alcohol, smoking and substance involvement screening test (ASSIST) was developed by the World Health Organization as a technical tool designed to assist with the early identification of substance use-related health risks and SUDs in primary healthcare, particularly in community-based primary healthcare settings. As a screening tool, ASSIST was envisioned to identify people using substances with the intent to provide a referral for brief substance use intervention.11
ASSIST is a questionnaire that screens for all levels of the problem or risky substance use in adults, providing a comprehensive assessment tool of eight questions covering tobacco, alcohol, cocaine, cannabis, amphetamine-type stimulants, inhalants, sedatives, hallucinogens, opioids, and other drugs.
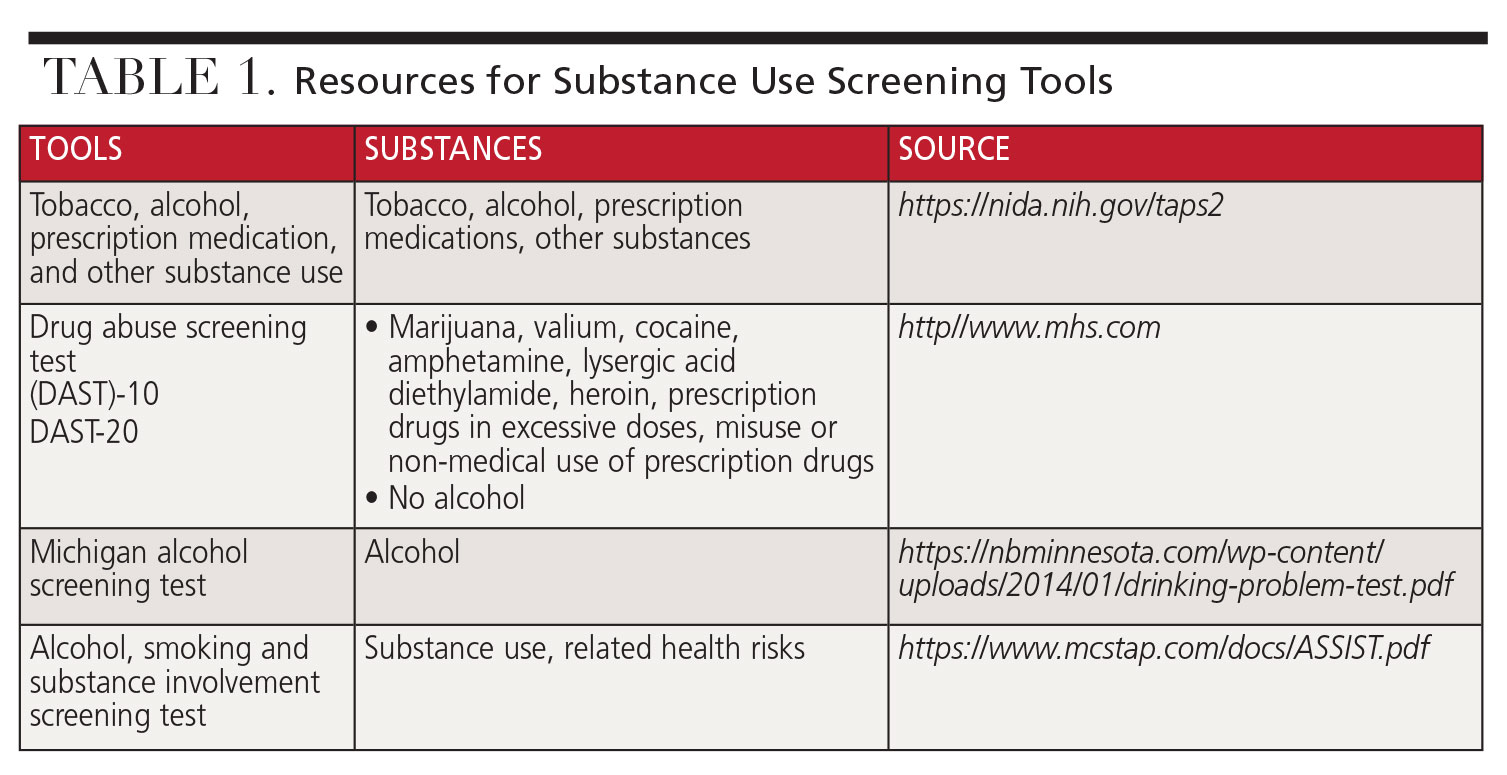 Multiple sources are available to access these screening tools. The National Institute on Drug Abuse is an excellent source: nida.nih.gov/nidamed-medical-health-professionals/screening-tools-resources/chart-screening-tools.12 See Table 1 (page 39) for more resource information.
Multiple sources are available to access these screening tools. The National Institute on Drug Abuse is an excellent source: nida.nih.gov/nidamed-medical-health-professionals/screening-tools-resources/chart-screening-tools.12 See Table 1 (page 39) for more resource information.
Integration Into the Dental Setting
Substance dependence, drug abuse, and addiction are complex medical issues requiring a broad understanding of these problems in terms of medical and dental patient management. Dental professionals should obtain adequate knowledge in recognizing the symptoms of drug abuse. The use of evidence-based screening and diagnostic tools in a dental setting is as essential as it is in modern medical practice.
Some studies suggest that dental patients who misuse illicit drugs are strongly reluctant to disclose information about their behaviors due to fears of possible breach of privacy, social stigma, legal implications, or even legal prosecution.13
In contrast to seemingly negative attitudes reported by some studies, patient surveys noted by other research projects demonstrate that patients are generally amenable to receiving medical screenings chairside in the dental setting for such conditions as human immunodeficiency virus, heart disease, and diabetes.14
These findings suggest that substance use/misuse screening has its rightful place in the dental setting, especially when it coincides with a complete diagnosis and improved dental care. Therefore, such a screening process should become part of the dental screening routine and must be a well-developed, two-way communication between a patient and a dental provider.
Implementation of substance use screening is a gradual process. It is unreasonable to expect dental patients to accept substance use questionnaires without questioning the rationale for such a request. Adding some basic questions to traditional office initial intake and recare medical history update forms may open the communication lines between the patient and the provider. Once a substance use/misuse problem is detected, the dentist may confidentially suggest to the patient that additional self-assessment questionnaires are available, encouraging reflection on personal substance use habits. Additionally, dentists should build a resource base so patients can be referred to substance use treatment practitioners.
Benefits of Screening
Screening for substance use is a process of evaluation for the possible presence of a problem, with answers to the questions being a simple yes or no. On the other hand, assessment is a process for defining the nature of the problem, establishing a diagnosis, and developing a specific treatment plan.
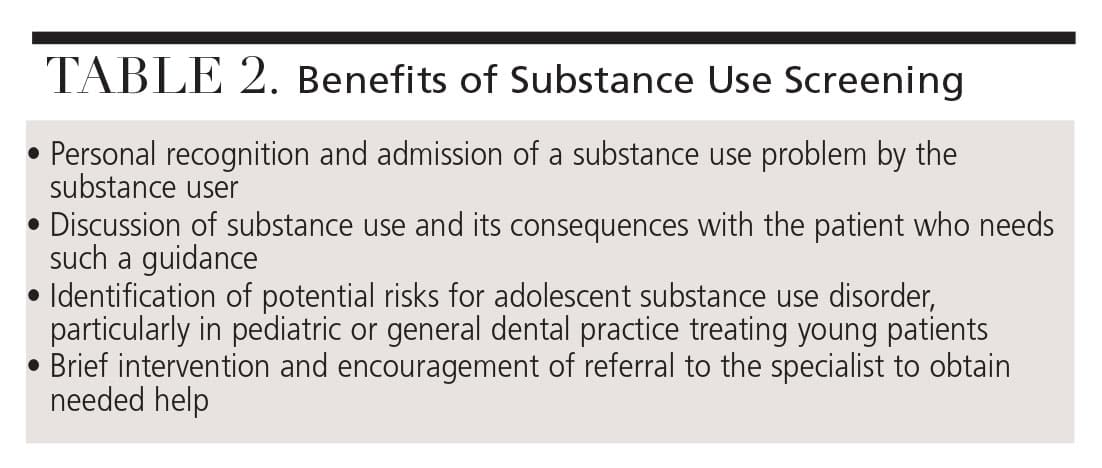 While the rationale of introducing substance use/misuse screening in the dental setting is to determine the presence of the problem, the benefits of introducing screening into dental practice go beyond simple yes or no determinations. Table 2 lists the benefits of substance use screening tools.
While the rationale of introducing substance use/misuse screening in the dental setting is to determine the presence of the problem, the benefits of introducing screening into dental practice go beyond simple yes or no determinations. Table 2 lists the benefits of substance use screening tools.
Substance use comes with many serious negative consequences, including involvement with the criminal justice system, social structure breakdown, family and relationship problems, and health and mental health issues. These consequences are equally detrimental for both adults and adolescents, justifying screening efforts in pediatric dental practices as well as general dental settings serving adult and adolescent patients.
According to Levy et al,15 the prevalence of marijuana use among 8th, 10th, and 12th graders (combined) in 2016 was nearly 23%. In addition, approximately 20% of adolescents reported alcohol use in the past month.16
A Public Approach to Substance Use
Screening, brief intervention, and referral to treatment (SBIRT) is a public health initiative to deliver early intervention and treatment services for individuals at risk of developing SUDs and those who have already experienced SUDs.
SBIRT can be delivered in many clinical settings and today is adapted for use in primary care settings, hospital emergency departments, and medical practices, enabling the screening of large numbers of individuals and presenting opportunities to engage with treatment for patients in need of an immediate and intensive treatment as well as those with less severe SUDs who may benefit from brief interventions. Implementation of the SBIRT initiative in the dental setting is both justified and necessary.17
Conclusion
Parish notes21 that while more than three-quarters of American dentists inquire about substance misuse with their patients, about two-thirds do not perceive such screening as compatible with their professional role. Yet, dentists frequently encounter patients with SUDs and are uniquely situated to recognize SUDs as well as make appropriate referrals to treatment centers.
An introduction of standardized screening measures that have been validated and used in healthcare settings opens the door to conversations that dentists can use to explore the sensitive topic of substance misuse and initiate specialty referrals accordingly.18
The overwhelming majority of dental practitioners recognize the effects of SUDs on dental patients, but the importance of screening for substance use in a dental setting is largely undervalued. This can probably be attributed to a lack of clinical training and under-appreciation of diagnostic capabilities of substance use disorders in the dental environment. In contrast, some research demonstrates that if the obstacles to SUD screening posed by reimbursement issues, need for training, and lack of support were reduced, oral health professionals may be more apt to discuss substance use among patients.19
Brief and effective clinical interviewing is a critical element in identifying patients’ substance use risk factors. While many dental practitioners may perceive identifying patient substance use as a clinical finding that falls beyond the scope of dental training and practice, it is difficult to justify not doing this in modern dental settings.
References
- Viswanath A, Barreveld AM, Fortino M. Assessment and management of the high-risk dental patient with active substance use disorder. Dent Clin North Am. 2020;64:547-558.
- American Dental Association. Statement on the Provision of Dental Treatment for Patients With Substance Use Disorders. Available at: ada.org/about/governance/current-policies. Accessed September 17, 2023.
- Giddon DB. Should dentists become ‘oral physicians’? Yes, dentists should become “oral physicians.” J Am Dent Assoc. 2004;135:438–439.
- Sainsbury D. Drug addiction and dental care. N Z Dent J. 1999;95:58-61.
- Parish CL, Pereyra MR, Pollack HA, et al. Screening for substance misuse in the dental care setting: findings from a nationally representative survey of dentists. Addiction. 2015;110:1516-1523.
- McNeely J, Wright S, Matthews AG, et al. Substance-use screening and interventions in dental practices: Survey of practice-based research network dentists regarding current practices, policies and barriers. J Am Dent Assoc. 2013;144:627–638.
- National Institute of Health. Tobacco, Alcohol, Prescription medication, and other Substance use (TAPS) Tool. Available at: nida.nih.gov/taps2/#/. Accessed September 17, 2023.
- National Institute on Drug Abuse. Instrument: Drug Abuse Screening Test. Available at: cde.nida.nih.gov/instrument/e9053390-ee9c-9140-e040-bb89ad433d69#:~:text=The%20Drug%20Abuse%20Screen%20Test%20%28DAST-10%29%20was%20designed,the%20degree%20of%20consequences%20related%20to%20drug%20abuse. Accessed September 17, 2023.
- Skinner HA. The drug abuse screening test. Addict Behav. 1982;7:363–371.
- National Institute of Health. Michigan Alcoholism Screening Test (MAST) . Available at: pubs.niaaa.nih.gov/publications/AssessingAlcohol/InstrumentPDFs/葶_MAST.pdf. Accessed September 17, 2023.
- World Health Organization. The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST). Available at: who.int/publications/i/item/-2. Accessed September 17, 2023.
- National Institute on Drug Abuse. Screening and Assessment Tools Chart. Available at: nida.nih.gov/nidamed-medical-health-professionals/screening-tools-resources/chart-screening-tools. Accessed September 17, 2023.
- McDaniel TF, Miller D, Jones R, Davis M. Assessing patient willingness to reveal health history information. J Am Dent Assoc. 1995;126:375–379.
- Greenberg BL, Kantor ML, Jiang SS, Glick M. Patients’ attitudes toward screening for medical conditions in a dental setting. J Public Health Dent. 2012;72:28–35.
- Levy S, Weiss R, Sherritt L, et al. An electronic screen for triaging adolescent substance use by risk levels. JAMA Pediatrics. 2014; 168: 822-828.
- Kelly SM, Gryczynski J, Mitchell SG, Kirk, A, O’Grady KE, Schwartz RP. Validity of brief screening instrument for adolescent tobacco, alcohol, and drug use. Pediatrics. 2014;133:819–826.
- Rahm AK, Boggs JM, Martin C, et al. Facilitators and barriers to implementing screening, brief intervention, and referral to treatment (SBIRT) in primary care in integrated health care settings. Subst Abus. 2015;36:281–288.
- Parish CL, Pereyra MR, Pollack HA, et al. Screening for substance misuse in the dental care setting: findings from a nationally representative survey of dentists. Addiction. 2015;110:1516–1523.
- McNeely J, Wright S, Matthews AG, et al. Substance-use screening and interventions in dental practices: a survey of practice-based research network dentists regarding current practices, policies, and barriers. J Am Dent Assoc. 2013;144:627–638.
From Decisions of Dentistry. October 2023; 9(9):36,39-41

