
A Dark Horse of Restorative Dentistry
Certain clinical considerations are necessary to achieve success with resin bonded fixed partial dentures
The resin bonded fixed partial denture (RBFPD) has been around for nearly a half century. In 1973, Rochette1 reported on bonding gold alloy retainers to mandibular anterior teeth without preparations. Conventional RBFPDs consisted of two retainers that were made of metal-ceramic materials. Earlier designs relied on macromechanical retention by creating perforations in the retainers to lock in the resin tags.2 Later, micromechanical retention was developed by using a type of electrolytic etching at the University of Maryland, hence the name “Maryland bridge.”3 Finally, in the 1990s, all-ceramic materials were introduced.4
Previously, RBFPDs were recommended for only short-term use as they had high complication rates compared to traditional full-coverage fixed partial dentures, with debonding being the most common issue.5,6 In the late 1990s, Kern7,8 discussed the cantilevered all-ceramic RBFPD and followed up with a 15-year survival analysis of this prosthesis with promising results.
The RBFPD’s most significant advantage is the conservative nature of its preparations, making it a popular restoration for children and young adults.9 The disadvantage is that the prosthesis relies exclusively on adhesive bonding for retention. Therefore, the quality and quantity of enamel, alignment, health of the teeth, and occlusion must be favorable.
Clinical Considerations
Patient selection, communication with other specialists, and treatment planning are vital for the success of these restorations. Short-span edentulous spaces in young patients that haven’t completed growth or patients who are not candidates for implant therapy benefit from these restorations.
Optimizing a bond to enamel is crucial. To allow for an optimal bond, preparations should be supragingival, and abutment teeth must have at least 30 mm2 of enamel. The available area of enamel to bond to may be compromised in microdonts, crowded, or rotated teeth.
Occlusion is another consideration that would allow sufficient thickness of the retainer wing and connector between the pontic and retainer. The recommended connector height should be at least 3 mm tall and 2 mm wide.10 Be mindful of patients with a deep bite or malposed teeth. It is also essential to avoid guidance on the pontic during excursive movements.
Metal frame RBFPDs have a major esthetic disadvantage on teeth with thin enamel owing to a grayish discoloring of the abutment teeth. The benefit of all-ceramic frameworks, whether zirconia or lithium disilicate, is they come in tooth shades that yield better esthetic outcomes.
Patients with parafunctional habits or who play contact sports need to wear an occlusal device to protect the restorations. The patient should also be warned about the risk of other parafunctional habits, such as nail or pen biting around the abutment teeth or pontics.
Biomechanical Considerations
A RBFPD with multiple abutments is more likely to fail due to the various vectors of tooth movement during function. This can manifest clinically as one of the retainers debonding, which may be unnoticed by the patient and can increase the risk of caries in the area under the failed retainer. This led to the popularity of the single retainer, cantilever design RBFPD.
Various contemporary materials are used for this prosthesis. The recommended ceramic materials for these types of restorations are lithium disilicate (LS2), which is a silica-based ceramic, and zirconia, which is a nonsilica-based ceramic. Zirconia has a higher flexural strength than LS2, however LS2 has better esthetic properties. Newer generation zirconia boasts improved esthetic properties at the expense of flexural strength.11 Pre-treatment of LS2 is performed with hydrofluoric acid as it is capable of being etched. This, however, cannot be achieved on nonsilica-based ceramics, such as zirconia, whose surface must be roughened by air particle abrasion.
Once the surface of the ceramic is roughened, it is primed with a coupling agent such as silane for silica-based ceramics or a ceramic primer containing methacryoloxydecyldihydrogenphosphate (MDP) for zirconia-based ceramics. Adhesive resin cements are recommended for bonding these restorations after treating the tooth substrate with the appropriate bonding agent following the manufacturer’s recommendations.
Clinical Techniques
The need for tooth preparations is subject to retainer thickness, occlusion, and convenience of seating the restoration. Some advocate for no preparations, while others prefer minimally preparing the teeth to include a slight chamfer, proximal groove, or box, and a pinhole in the center of the lingual fossa. Preparations must be in enamel as bond strengths are higher compared to dentin.

A thorough knowledge of bonding chemistry and material properties of the RBFPD are crucial for long-term success of these restorations. Following the manufacturer’s instructions, pre-treatment of the restoration, and preparing the enamel for bonding under isolation are the first steps. A resin cement adhesive is used to bond the restoration to the tooth. Excess cement is removed and occlusion is adjusted to complete the bonding protocol. Hygiene and maintenance instructions are provided, along with stressing the risk of debonding and returning to the practice as soon as it happens.

If the retainer debonds, the options are to remake or rebond the restoration. If there is an apparent reason for the restoration to debond, such as trauma, and the restoration is intact, rebonding is possible. However, once a RBFPD has debonded, it is more likely to fail again if case selection was inappropriate. The RBFPD design, patient occlusion, and parafunctional habits should be carefully re-evaluated.

Case Report
A 14-year-old girl presented to a private practice in New York City with bilateral maxillary lateral incisor agenesis (Figure 1). She recently completed 4 years of orthodontic treatment, including palatal expansion. Her medical history was unremarkable. Her dental history included extraction of primary dentition, orthodontic therapy, dental sealants, and routine dental maintenance.

Oral and radiographic examinations revealed oligodontia (missing teeth: maxillary second premolars, maxillary lateral incisors, mandibular right first premolar, and mandibular second premolars). The anterior teeth had a shade of A3 with which she was unhappy. The periodontal tissue was normal and healthy.


The edentulous alveolar ridges were deficient in the buccal-lingual dimension (Figure 2). The anterior spacing and dentofacial esthetics were appropriate. The occlusal scheme was canine guidance. The definitive treatment plan included vital tooth bleaching, alveolar ridge augmentation, gingivoplasty, and two lithium disilicate glass-ceramic RBFPDs.
The periodontist performed an alveolar ridge augmentation. Papilla sparing incisions were made followed by full thickness flap reflection. Following cortical perforations, grafting was performed using a xenograft bone matrix combined with a platelet-derived growth factor, volume-stable collagen matrix, and platelet-rich fibrin membranes. The flap was coronally advanced in order to obtain primary closure (Figure 3). After 4 weeks of uneventful healing, the patient completed in-office tooth bleaching. After 8 weeks of total healing, gingivoplasty was done to develop pontic sites (Figure 4). A thermoformed retainer with ovate pontics made of bis-acryl resin was utilized to develop the soft tissue.


Two weeks later, the central incisors were prepared for the RBFPDs (Figure 5). The central incisors were selected as the abutment teeth due to the large proximal contact area, the ability to hide the wing, increased bonding surface, and to maintain the natural canine guidance occlusal scheme. The abutment preparations were minimally invasive and confined to the enamel. The preparation design consisted of a light incisal shoulder, flat proximal box, pinhole, and a light cervical chamfer as described by Kern.7
The proximal box was lingual to the transitional line angles. The impression was made with a polyether impression material. The previously fabricated thermoformed retainer was used as a provisional. The impressions were poured with Class IV stone and full anatomical wax-ups were made.

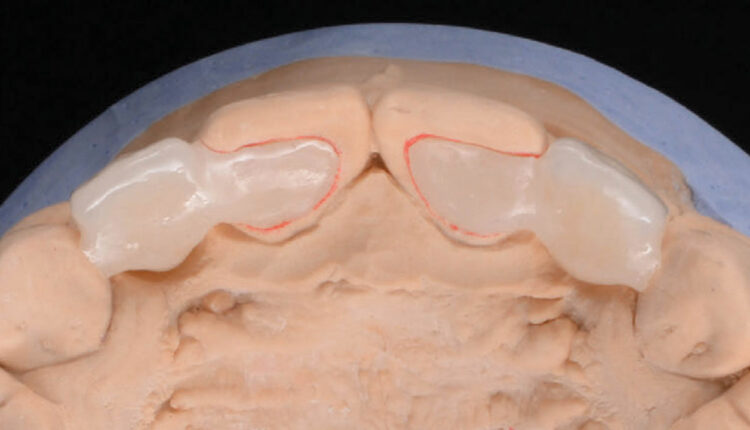
The RBFPDs were pressed out of low translucency lithium disilicate glass-ceramic using the lost-wax technique (Figure 6). The RBFPDs were cut back and veneered with a nanofluorapatite glass ceramic (Figure 7). Extra seating struts were made on the canines to facilitate correct placement and orientation of framework during laboratory fabrication and clinical try-in. These struts were removed prior to final delivery.

The RBFPDs were tried in to verify fit and esthetics. Color modification and shade matching were done to match the characteristics of the adjacent teeth. The esthetics were approved by the patient and parents. The abutment teeth were cleaned with pumice and acid etched with 37% phosphoric acid. The RBFPDs were etched with hydrofluoric acid and silanated per the manufacturer’s recommendations.
The restorations were then adhesively bonded to the abutment teeth using resin cement under strict isolation. The occlusion was verified, and final radiographs were taken. Clear aligner retainers were fabricated for orthodontic retention. Esthetic and functional parameters were verified during follow-up visits and the patient was placed on 6-month hygiene recare schedule. Figures 8 through 10 show the final result at the 8-week follow-up visit.
RBFPDs are conservative, economical, and time-saving fixed restorations that are used to restore anterior and posterior short-span edentulous sites. Patients in all age groups can benefit from these restorations as interim or definitive treatments. In addition, current research has shown that these restorations have a high success rate over 10 years.
Acknowledgment
The authors would like to thank the ceramist Simon Wong, MDT, and the treating periodontist Hector Sarmiento, DMD.
References
- Rochette AL. Attachment of a splint to enamel of lower anterior teeth. J Prosthet Dent. 1973;30:418–423.
- Howe DF, Denehy GE. Anterior fixed partial dentures utilizing the acid-etch technique and a cast metal framework. J Prosthet Dent. 1977;37:28–31.
- Livaditis G, Thompson VP: Etched castings: an improved retentive mechanism for resin-bonded retainers. J Prosthet Dent. 1982;47:52.
- Kern M, Knode H, Strubb JR. The all-porcelain, resin-bonded bridge. Quintessence Int. 1991;22:257–262.
- Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JY. Clinical complications in fixed prosthodontics. J Prosthet Dent. 2003;90:31–41.
- Thoma DS, Sailer I, Ioannidis A, Zwahlen M, Makarov N, Pjetursson BE. A systematic review of the survival and complication rates of resin-bonded fixed dental prostheses after a mean observation period of at least 5 years. Clin Oral Implants Res. 2017;28:1421–1432.
- Kern M, Gläser R. Cantilevered all-ceramic, resin-bonded fixed partial dentures: a new treatment modality. J Esthet Dent. 1997;9:255–264.
- Kern M. Fifteen-year survival of anterior all-ceramic cantilever resin-bonded fixed dental prostheses. J Dent. 2017;56:133–135.
- Durey KA, Nixon PJ, Robinson S, Chan MF. Resin bonded bridges: techniques for success. Br Dent J. 2011;211:113–118.
- Kern M. Resin-Bonded Fixed Dental Prostheses: Minimally Invasive–Esthetic–Reliable. Batavia, Illinois: Quintessence Pub Co; 2019.
- Sulaiman TA. Materials in digital dentistry—a review. J Esthet Restor Dent. 2020;32:171–181.
key takeaways
- Advances made in resin bonded fixed partial denture (RBFPD) technology made since 1973 include the transition from macromechanical to micromechanical retention and the introduction of all-ceramic materials.
- Success with RBFPDs hinges on careful patient selection, communication among specialists, and thorough treatment planning, particularly emphasizing the conservative nature of enamel preparations.
- A single retainer, cantilever design is preferred over multiple abutments to minimize failure risks.
- Lithium disilicate and zirconia offer different flexural strengths and esthetic properties in RBFPD applications.
- A comprehensive understanding of bonding protocols, enamel preparation, and post-bonding care is needed ensure the long-term success of these restorations.
From Decisions in Dentistry.November/December 2023; 9(10):13-14,16-17
