

Clinical Utility of Short Dental Implants
Readily identifying situations in which short dental implants are appropriate will set realistic clinical expectations and improve long-term surgical and prosthetic outcomes.
PURCHASE COURSE
This course was published in the June 2021 issue and expires June 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the June 2021 issue and expires June 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Provide a general definition of short and extra short dental implants, as well as potential clinical benefits of these appliances.
- Discuss clinical applications for short and extra short implants.
- Explain survival rates for extra short implants, as well as the potential affect of bone levels in patients with short implants compared to longer implants.
Treatment of the atrophic maxilla and mandible can pose significant anatomical challenges when dental implant prostheses are desired. Guided bone regeneration procedures may be attempted to increase native ridge dimensions and overcome sinus pneumatization for future implant placement. However, variations in dental implant size and shape can minimize the need for traditional site development surgeries that may prove costly and unpredictable, as well as high risk for medically compromised patients.
The actual definition of short implants remains controversial in the literature. Based on known studies, this review will define short dental implants as ≤ 8 mm in length, and extra short will be considered ≤ 6 mm long. While both implant designs represent viable alternatives, they are not immune to biologic and prosthetic complications.1,2 The ability to readily identify situations in which short implants are appropriate will set realistic clinical expectations and improve long-term surgical and prosthetic outcomes.
The design and application of short implants cannot be fully understood without first tracing their origin. The concept of replacing missing teeth goes back millennia and was revolutionized by implant dentistry. While the transition from subperiosteal to endosseous implants dramatically improved their survival rate, it was not until the introduction of titanium that surgeons could truly appreciate osseointegration. Titanium is bioinert and offers high corrosion resistance, lending to optimal bone apposition, chemical stability and a low elastic modulus. The protective titanium oxide layer that forms around the implant surface is still vulnerable to pathogenic bacteria, micromotion and fretting. To counteract these factors, titanium has modifiable surface properties, which have become central to its evolution in recent years.3
Commercially pure titanium implants placed and documented by Brånemark were originally used in the edentulous patient. Multiple parallel implants were placed interforaminally in the mandible and between the anterior walls of the maxillary sinuses. These implants had a machined surface with an external hex connection that were splinted by a metal framework in the definitive restoration because they lacked anti-rotational features.4 The mean vertical bone loss in the first year after installation was 1.2 mm, with 0.2 mm bone loss every year thereafter.5
Many of the current standards for implant success are based on these early implants. The first studies evaluating implant survival in partially edentulous patients showed a greater number of failures in shorter dental implants.6,7 Implants were later adapted to different clinical situations through changes in their design. For example, innovations in the implant-abutment connection support increased prosthetic success when used for single-tooth restorations. These include anti-rotational features and the internalization of the implant connection. While the external hex interface concentrates forces on the abutment screw, thereby increasing the incidence of screw loosening, internalization better distributes occlusal forces along the implant.8
 Platform-switching or platform-shifting moves the microgap of the implant abutment connection further away from the oral environment, minimizing bone loss from harbored biofilms. A meta-analysis showed significantly less bone loss in platform-switched implants, if the difference in the implant-abutment diameter was ≥ 0.4 mm.9 Furthermore, a tapered implant body increases primary stability across all bone types and allows for placement in undercuts, narrow ridges or tight interdental spaces. Threads maximize initial bone-to-implant contact with decreasing pitch by enlarging the implant’s surface area. Microthreads and added texturing further dissipate coronal forces that can reduce crestal bone loss at the implant site.10
Platform-switching or platform-shifting moves the microgap of the implant abutment connection further away from the oral environment, minimizing bone loss from harbored biofilms. A meta-analysis showed significantly less bone loss in platform-switched implants, if the difference in the implant-abutment diameter was ≥ 0.4 mm.9 Furthermore, a tapered implant body increases primary stability across all bone types and allows for placement in undercuts, narrow ridges or tight interdental spaces. Threads maximize initial bone-to-implant contact with decreasing pitch by enlarging the implant’s surface area. Microthreads and added texturing further dissipate coronal forces that can reduce crestal bone loss at the implant site.10
Implant surfaces can also be prepared or roughened through additive or subtractive techniques. Historically, hydroxyapatite coating and titanium plasma spraying were added. Today, the implant topography is “subtracted” by electropolishing or mechanical polishing, blasting or acid etching with different particles, and/or anodizing. Combinations of these techniques have led to greater surface roughness and marginal bone stability on the micro- and nanometer levels, as reported in a systematic review.11 Changes to the implant body or surface, however, do not compensate for all anatomical limitations, such as sinus pneumatization and ridge atrophy. Short dental implants offer a promising alternative for patients who cannot afford to undergo site development surgery for conventional implant placement.
APPLICATIONS FOR SHORT IMPLANTS
Because most loading forces are concentrated at the alveolar crest, implant length should have lesser effects on marginal bone and tissue stability. Short and extra short implants have shown minimal differences in survival over time. A systematic review of extra short implants noted a mean survival rate of 94.1%, with a maximum bone loss of 0.53 mm after five years.2
Shorter implants are advantageous in cases of sinus pneumatization. Patients with limited finances, sinus pathology, or moderate to severe obstructive sleep apnea requiring nighttime appliances may not be candidates for sinus augmentation procedures. In comparing extra short implants placed in native bone to 11- to 15-mm implants placed after sinus augmentation in the posterior maxilla, no significant differences in patient-level implant survival rates were reported (98.1% and 100%, respectively). There were also no significant differences in marginal bone loss, probing depths, and bleeding on probing after five years post-loading.12 In the atrophic maxilla or mandible, the cost, complication rate, and lack of predictability of vertical ridge augmentation may not be justified if placing a short implant is a viable option.13
This evidence supports fixed implant solutions to patients with anatomical restrictions. A recent meta-analysis demonstrated survival rates of 90% to 100% for fixed dental prostheses supported by extra short implants in the posterior mandible and maxilla.14 A potentially overlooked application of short implants is in the assistance of complete and partial removable dental prostheses in the severely resorbed residual ridge. This prosthetic design allows occlusal forces to be distributed and shared between the load-bearing areas of the residual ridge and surrounding surfaces. This type of load distribution leads to fewer implant and prosthetic complications when compared to short implants supporting a fixed prosthesis.15

POTENTIAL COMPLICATIONS SECONDARY TO SHORT IMPLANTS
Although short dental implants have similar clinical parameters to their longer counterparts, they are not without complication. Biologic complications from placing implants in anatomically compromised areas include nerve compression or injury, sinus communication or mandibular fracture. Careful planning, issuing postoperative instructions, and postprocedural follow-up must be performed in order to decrease the risk of surgical misadventures.
Compared to longer implants, bone loss around an extra short implant is potentially more detrimental. For example, 2 mm of bone loss around a 6-mm implant translates to a greater percentage of bone loss when compared to 2 mm of bone loss around a 10-mm implant. This may lead to a short implant becoming hopeless at an earlier point in time.
Short implants typically have greater crown-to-implant ratios. While there is not a direct relationship between crown-to-implant ratio and marginal bone loss, it has been directly correlated with an increase in prosthetic complications, such as screw loosening or screw fracture.16,17 Nonaxial or horizontal forces lead to rotation of the implant restoration around a fulcrum located at the level of the implant platform.18 A taller crown serves as a vertical cantilever and magnifies nonaxial occlusal forces at the implant-abutment connection. To more advantageously occupy excessive restorative space, providers may consider the use of a tissue-level implant with machined necks or collars that can translate the platform of the implant 0.5 to 2.8 mm coronal to the crest of the bone (depending on the manufacturer). This decreases the length of the vertical cantilever, which reduces the magnification of off-axis forces at the level of the prosthetic screw. The use of a tissue-level implant is often contraindicated in the esthetic zone, however, where the development of a customized emergence profile is crucial and visibility of an implant collar would be considered a prosthetic failure.
In cases in which a large crown-to-implant ratio is inevitable, careful occlusal management prevents the transmission of nonaxial forces to the implant-abutment connection. This is accomplished by eliminating occlusal contacts with the implant restoration in excursion. Canine teeth, however, require contact in excursive movements to provide a functional occlusal scheme, so prosthetic splinting has been suggested to harmonize crown-to-implant ratios.14 Splinting multiple implants distributes potentially unfavorable forces across multiple fixtures, which reduces the force transmitted to a single prosthetic interface.
CASE REPORT
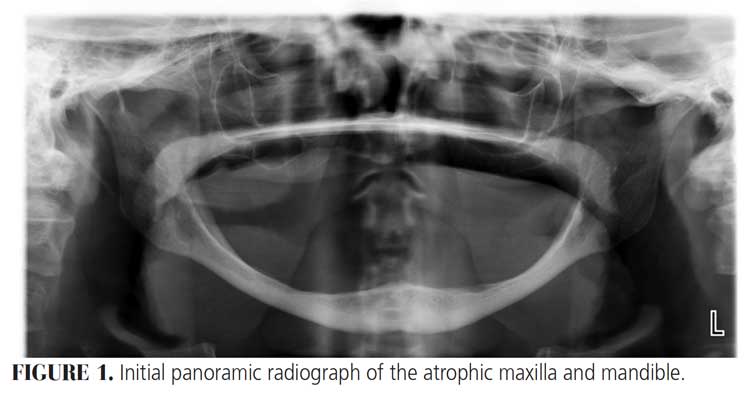
The following case illustrates the use of short dental implants in the atrophic mandible. A 73-year-old female presented to the graduate periodontics clinic at the University of Texas Health Science Center at San Antonio School of Dentistry interested in replacing her existing dentures (Figure 1 through Figure 9). She had a medical history significant for hypertension, osteopenia and acid reflux.
The patient presented with poor anatomical expectations for the retention, stability and support of a mandibular complete denture secondary to retruded tongue posture and an unfavorable lateral throat form. For more than 25 years, she had been using maxillary and mandibular dentures with inadequate stability, support and retention. The initial examination revealed diminished occlusal vertical dimension and autorotation of the mandible from wear of the denture teeth that gave her the appearance of a protruded mandible.
After a thorough evaluation and review of various techniques and materials, a comprehensive treatment plan was developed, and consent was obtained. Surgical procedures were performed using IV conscious sedation. The treatment plan included:
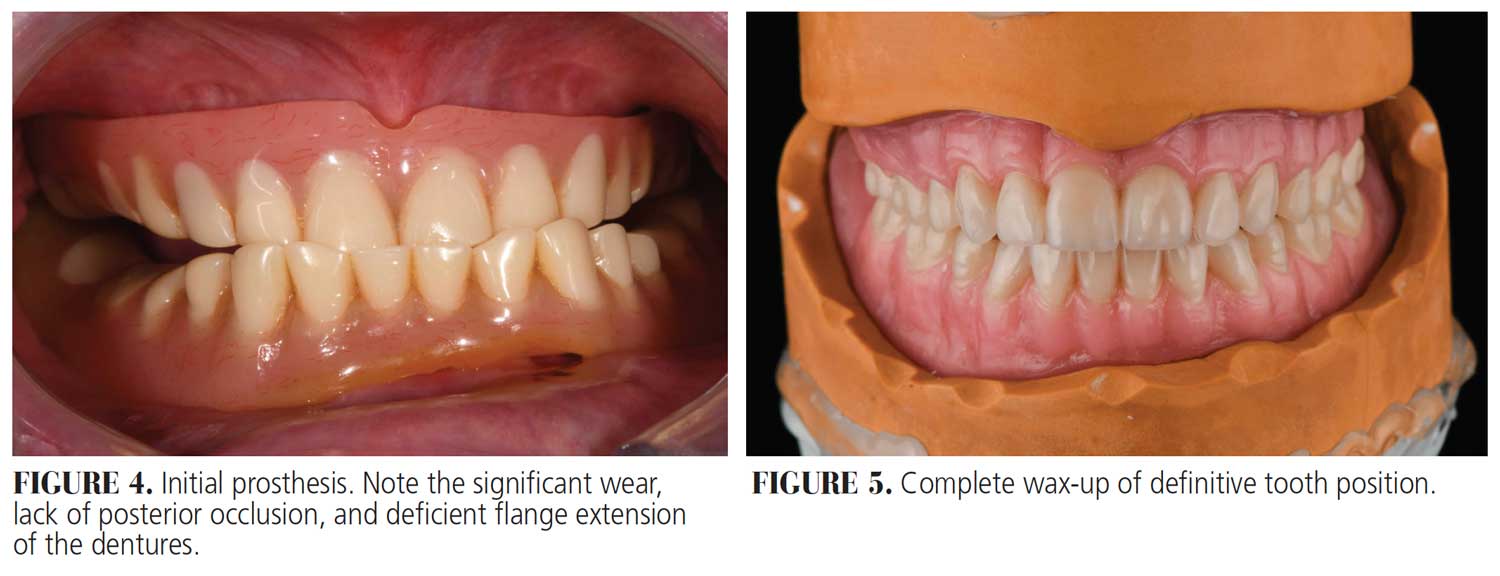
- Wax-up of the definitive location of the maxillary and mandibular teeth
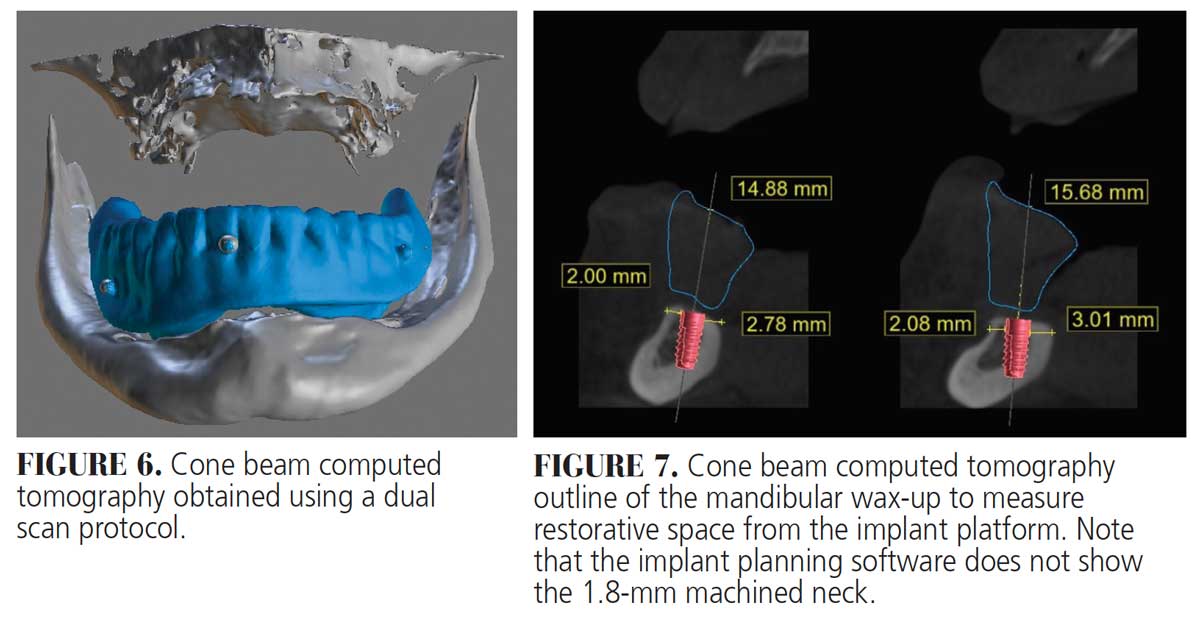
- Cone beam computed tomography (CBCT) with the mandibular denture in place using a dual scan protocol to plan for future implant placement
- Placement of two interforaminal implants
- Fabrication of the definitive maxillary complete denture and mandibular implant-assisted bar overdenture
Maxillary and mandibular wax-ups were completed, and six radiographic markers were placed on the mandibular wax-up for both scans. The dual scan protocol was performed with an initial CBCT scan of the mandibular arch with the wax-up in place, followed by a separate scan of the wax-up alone. This provides visibility of the definitive tooth position within the implant planning software, and acts as a reference of restorative space during implant planning. Due to anatomical restrictions from an atrophic mandible, narrow 8 mm-long implants were planned for sites #22 and 27. Occlusal forces will be distributed across, and shared between, the buccal shelves of the posterior mandible and implant fixtures. This distribution pattern allows for the use of implants of smaller diameter and length.
As noted, an implant-assisted bar overdenture was planned for the definitive mandibular prosthesis. Parallelism of implants was not critical in this case due an increase in restorative flexibility afforded by the bar splinting the fixtures. A nonrestrictive guide, duplicated from the proposed overdenture, helped idealize the implant position for correct three-dimensional implant placement. Nonrestrictive guides are relatively inexpensive, allow for visualization of the proposed restoration, and afford intraoperative flexibility to the clinician during implant placement. While such flexibility may be considered beneficial, it leads to an increase in the number of decisions made at the time of surgery. Caution should be taken to ensure visualization and careful management of the surgical field in order to prevent surgical complications.
Genial tubercles were used as a fixed reference when determining the maximum length of the linear incision. Mental foramina were located at the alveolar crest and palpated, and a linear incision was made slightly lingual to the ridge crest to prevent nerve damage. A buccal releasing incision was made at the midline for improved flap relaxation. A full thickness flap was reflected in order to visualize the ridge crest. Two tissue-level, 3.3 mm-wide by 8 mm-long implants were placed at sites #22 and 27, per the manufacturer’s recommendations, and primary stability was achieved. Tissue-level implants were selected to move their restorative platforms away from the floor of the mouth. The position of the platform decreases the possibility of the implant becoming submerged in soft tissue when abutments are removed and replaced. Implants were placed toward the lingual border of the mandible to facilitate restorative access. This should not be routinely performed, however, due to possible nerve damage, lingual plate perforation and mandibular fracture. Flaps were repositioned and secured using resorbable simple interrupted sutures.
Postoperative instructions were reviewed and the patient was advised to avoid wearing her mandibular complete denture during initial healing to minimize the risk of implant failure and jaw fracture. The patient returned for follow-up at two weeks, one month, and then monthly until her final recall at four months for a pre-restorative check. The tissues surrounding the implants were healthy, pink and firm, with no signs or symptoms of peri-implant disease. A panoramic radiograph established a baseline for future reevaluations. Next, 4.5 mm-tall healing abutments were attached. The patient returned to the prosthodontics clinic for fabrication of her final prostheses and will be seen for yearly recalls.

SUMMARY
Site development procedures may not be timely, practical or affordable for some patients. Short and extra short dental implants represent sound alternatives to treating the atrophic maxilla and mandible. Advancements in implant design and surface topography only add to their efficacy and long-term marginal bone stability. Any related biologic and prosthetic complications can be managed successfully when challenges are anticipated and a detailed treatment plan is presented as part of the initial patient evaluation.
REFERENCES
- Lee SA, Lee CT, Fu MM, Elmisalati W, Chuang SK. Systematic review and meta-analysis of randomized controlled trials for the management of limited vertical height in the posterior region: short implants (5 to 8 mm) vs longer implants (> 8 mm) in vertically augmented sites. Int J Oral Maxillofac Implants. 2014;29:1085–1097.
- Ravidà A, Barootchi S, Askar H, Suárez-López del Amo F, Tavelli L, Wang HL. Long-term effectiveness of extra-short (≤ 6 mm) dental implants: a systematic review. Int J Oral Maxillofac Implants. 2019;34:68–84.
- Linkow LI, Rinaldi AW, Weiss W Jr, Smith GH. Factors influencing long-term implant success. J Prosthet Dent. 1990;63:64–73.
- Adell R, Lekholm U, Rocker B, Brånemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg. 1981;10:387–416.
- Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants. 1986;1:11–25.
- Ivanoff CJ, Gröndahl K, Sennerby L, Bergström C, Lekholm U. Influence of variations in implant diameters: a 3- to 5-year retrospective clinical report. Int J Oral Maxillofac Implants. 1999;14:173–180.
- Lekholm U, Gunne J, Henry P, et al. Survival of the Brånemark implant in partially edentulous jaws: a 10-year prospective multicenter study. Int J Oral Maxillofac Implants. 1999;14:639–645.
- Shafie HR, White BA. Different Implant-Abutment Connections. In: Clinical and Laboratory Manual of Dental Implant Abutments. Shafie HR, ed. Hoboken, NJ: Wiley-Blackwell; 2014:33–46.
- Atieh MA, Ibrahim HM, Atieh AH. Platform switching for marginal bone preservation around dental implants: a systematic review and meta-analysis. J Periodontol. 2010;81:1350–1366.
- Abuhussein H, Pagni G, Rebaudi A, Wang HL. The effect of thread pattern upon implant osseointegration. Clin Oral Implants Res. 2010;21:129–136.
- Wennerberg A, Albrektsson T. Effects of titanium surface topography on bone integration: a systematic review. Clin Oral Implants Res. 2009;20(Suppl 4):172–184.
- Thoma DS, Haas R, Sporniak-Tutak K, Garcia A, Taylor TD, Hämmerle CH. Randomized controlled multicentre study comparing short dental implants (6 mm) versus longer dental implants (11–15 mm) in combination with sinus floor elevation procedures: 5-year data. J Clin Periodontol. 2018;45:1465–1474.
- Esposito M, Grusovin MG, Coulthard P, Worthington HV. The efficacy of various bone augmentation procedures for dental implants: a Cochrane systematic review of randomized controlled clinical trials. Int J Oral Maxillofac Implants. 2006;21:696–710.
- Papaspyridakos P, De Souza A, Vazouras K, Gholami H, Pagni S, Weber HP. Survival rates of short dental implants (≤ 6 mm) compared with implants longer than 6 mm in posterior jaw areas: a meta-analysis. Clin Oral Impl Res. 2018;29(Suppl 16):8–20.
- Omura AJ, Latthe V, Marin MM, Cagna DR. Implant-assisted removable partial dentures: practical considerations. Gen Dent. 2016;64:38–45.
- Garaicoa-Pazmiño C, Suárez-López del Amo F, Monje A, et al. Influence of crown/implant ratio on marginal bone loss: a systematic review. J Periodontol. 2014;85:1214–1221.
- Taylor TD, Wiens J, Carr A. Evidence-based considerations for removable prosthodontic and dental implant occlusions: a literature review. J Prosthet Dent. 2005;94:555–560.
- Zipprich H, Weigl P, Ratka C, Lange B, Lauer HC. The michromechanical behavior of implant-abutment connections under a dynamic loading protocol. Clin Implant Dent Relat Res. 2018;20:814–823.
From Decisions in Dentistry. June 2021;7(6)36-39.

