

Decision-Making In Modern Mucogingival Therapy
Properly managing mucogingival defects will set appropriate clinical expectations and improve long-term surgical outcomes.

The treatment of soft tissue deformities presents unique challenges for the dental team. Gingival recession and a minimal or absent band of attached keratinized tissue are among the leading mucogingival problems today. In fact, 50% of adults aged 18 to 64 have more than one site of recession, which only increases with age.1 Exposed root surfaces may be esthetically displeasing, hypersensitive, and/or predisposed to caries and noncarious cervical lesions. The majority of untreated buccal recession worsens in time, compromising the amount of thick, healthy tissue at the cervical area, often leading to discomfort during oral hygiene and poorer clinical parameters overall.2
Even with advances in soft tissue grafting materials and techniques, choosing the most appropriate and predictable surgical approach for a given case is one of the most disputed facets of periodontics. The need for surgical intervention, or type required, are often determined by the underlying etiology, oral hygiene compliance, and any planned orthodontic or restorative treatment (including implant therapy). However, the potential for root coverage or gain in keratinized tissue width largely depends on various tooth-, site- and patient-related risk factors.3 Learning to readily diagnose and treat mucogingival defects will set appropriate clinical expectations and improve long-term surgical outcomes.
The 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions adopted a new classification system for gingival recession.4 The existing Miller classification has considerable limitations, including the use of bone or soft tissue loss as the interdental criteria and the mucogingival junction as a landmark for measuring recession depth — both of which can be difficult to identify. It also lacks information on tooth- and site-related conditions to adequately prognosticate root coverage. Most notably, the predictability of root coverage was based on results from a free soft tissue autograft, which is not the preferred technique today.5

While other systems have been proposed, the newer Cairo et al6 classification is treatment-oriented and mindful of the latest surgical principles for root coverage. Recession is measured from the cementoenamel junction (CEJ) to the free gingival margin. Interproximal attachment is then measured from the CEJ to the most apical extent of the sulcus/pocket. Buccal attachment loss, if any, is similarly measured yet from the direct buccal aspect. The Cairo et al6 classification is as follows:
- Recession Type 1 (RT1): Gingival recession without interproximal attachment loss. The interproximal CEJ is not detectable. Miller Class I and II equivalency (Figure 1).
- Recession Type 2 (RT2): The amount of interproximal attachment loss is less than or equal to the buccal attachment loss. Miller Class III equivalency (Figure 2).
- Recession Type 3 (RT3): The amount of interproximal attachment loss is greater than the buccal attachment loss. Miller Class IV equivalency (Figure 3).
In these cases, the CEJ is detected visually or with a probe. However, about 40% of recession defects have no identifiable CEJ caused by dental lesions that modify or reshape the crown or root surface. Therefore, reconstruction of the CEJ should be included as part of mucogingival treatment either by the surgeon or referring dentist.7 Using the CEJ as an anatomical marker for root coverage also ensures the blood supply travels to the most coronal aspects of the grafted tissue. Pini-Prato et al8 developed a classification for the CEJ and associated root conditions that should be used with a diagnosis of recession, as follows:
- Class A: CEJ is detectable with (+) or without (-) a root step or concavity > 0.5 mm (Figure 4).
- Class B: CEJ is undetectable with (+) or without (-) a root step or concavity > 0.5 mm (Figure 4).

TOOTH-RELATED RISK FACTORS
Different surface conditions, such as caries, lesions or cervical restorations, can mask the proper outline of the CEJ. Noncarious cervical lesions (NCCLs) result from abrasion, erosion and corrosion. Traumatic occlusal forces only theoretically contribute to these lesions, where no causal association has been established.9 Their prevalence increases with age and ranges from 10% to 60%.10 According to a nine-year multilevel analysis, NCCLs were identified as a negative predictor for complete root coverage for coronally advanced flap and connective tissue grafting procedures.11 After gingival augmentation with a free soft tissue autograft, NCCLs > 0.5 mm were present in 60% of untreated sites compared to 36% of treated sites. A thin phenotype and < 2 mm keratinized tissue were significantly correlated with the development of NCCLs over a 20- to 30-year period.12
Tooth morphology and location also affect root coverage outcomes. The total area of the avascular tooth surface should consider the actual crown or root shape. A “prominent” tooth usually features a curved root that extends beyond the arch form. Reducing this convexity with a curet or bur along the long axis of the tooth shortens the distance cells need to migrate to establish plasmatic circulation for successful integration of the donor graft.13
It is now clear these tooth-related conditions must be diagnosed prior to surgery, and NCCLs, root caries, and poorly adapted restorative margins should be treated first. The contralateral tooth or interproximal line angles of the existing tooth can be used to imagine the line for the new CEJ prior to grafting and/or final restoration.

SITE- AND PATIENT-RELATED RISK FACTORS
The role of tissue phenotype has garnered attention — and controversy — in recent years. Thin phenotypes are often associated with increased recession and reduced root coverage. Augmenting tissue thickness with a connective tissue graft by means of phenotype modification has shown long-term stability around teeth.14 The addition of a connective tissue graft for single sites with a restored NCCL had higher recession reduction and esthetic scores when gingival thickness was < 0.84 mm.15 Generally, tissue thickness > 1.1 mm serves as the threshold for weighted mean and complete root coverage per a Mann-Whitney U test; weighted flap thickness was significantly correlated with root coverage in this systematic review.16
Baseline parameters present another surgical consideration, as < 3 mm of initial recession with a thick band of attached, keratinized tissue can predictably achieve complete root coverage.17 In fact, baseline recession and keratinized tissue width at the initial recall visit were most indicative of marginal stability according to a recent network meta-analysis.18 Sites with < 2 mm of keratinized tissue were prone to apical tissue migration over 20 years when a bilaminar surgical technique was used with connective tissue grafting for maxillary single recession-type defects.19 It is worth noting that the widely used “2 mm rule” for keratinized tissue width was misinterpreted from findings of the classic Lang and Löe20 study. The mandibular premolars anatomically have minimal attached tissue and are thereby predisposed to recession.20 No exact amount of keratinized tissue was defined by the 2017 World Workshop; instead, one that promotes an inflammation-free environment, maintains patient comfort and esthetics, prevents recurrence, and supports oral hygiene should be considered healthy.4
Neighboring tissues and anatomy also influence root coverage outcomes. If not addressed before or during treatment, high frenum attachment, muscle pull, and shallow vestibular depth are typically associated with recession and reduced root coverage. These factors often tip the scale toward a free soft tissue autograft for long-term stability, unless a frenectomy and/or vestibuloplasty is performed with a connective tissue graft.3 No significant correlation has been noted between the area or height of papillae to complete root coverage.21 Donor site anatomy should be assessed preoperatively in case allografts or xenografts are better suited. According to cadaver dissections, a shallow greater palatine neurovascular bundle is 7 mm from the CEJ of adjacent teeth. Extreme caution should be used during harvest site preparation, as a lack of appreciation for surgical anatomy can result in increased intraoperative bleeding, temporary paresthesia and delayed healing.22 Non-autogenous materials are viable alternatives when there is concern for greater postoperative discomfort or treatment of multiple recession-type defects not amenable to palatal harvesting alone.23

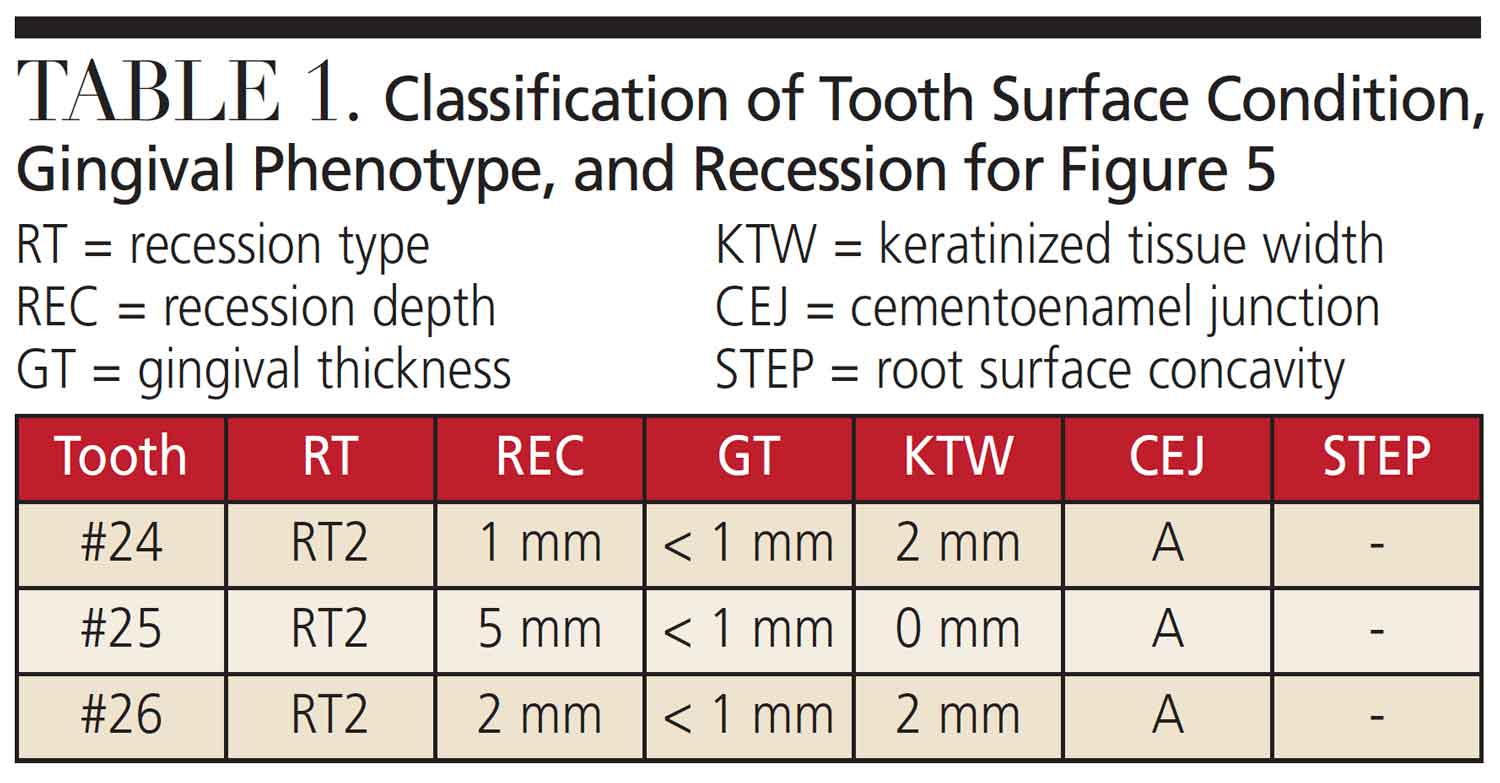
After evaluating and treating the tooth surface, tissue phenotype and width, baseline recession, and local anatomy should be recorded to accurately classify and prognosticate different mucogingival conditions. Table 1 provides an example of this comprehensive diagnostic approach, and this model can be used in addition to periodontal charting for every mucogingival case.4 Documenting that partial or complete root coverage is limited by certain risk factors in the informed consent establishes appropriate clinical expectations. When increased tissue width is the main goal, patients must understand that root coverage is not initially expected and would require further intervention. Waiting at least six months for surgical reentry allows for creeping attachment, especially in cases of narrow recession treated by a free soft tissue autograft. The gradual coronal migration of the gingival margin/sulcus is 0.8 mm on average and appreciated up to 12 months.24
Cigarette smoking is a known risk factor for periodontal and peri-implant disease. Nicotine decreases the levels and efficacy of protective chemokines and impairs the motility and function of major immune cells; it also decreases microvascular density and vessel diameter, thereby impairing healing.25
TREATMENT DRIVERS
Dentinal hypersensitivity may be a treatment driver as a result of exposed dentin. While the use of topically applied agents can be beneficial, periodontal-prosthetic treatment is more long-lasting, as reestablishment of the CEJ in conjunction with root coverage surgery can restore the exposed dentin and decrease sensitivity.26
Patient interests and needs for multidisciplinary treatment should be discussed prior to surgery. This is especially important for labial tooth movement or arch expansion, which can be performed after gingival augmentation. There is currently no evidence that supports phenotype modification prior to orthodontics, as health can be maintained with good oral hygiene and removal of underlying etiologies. However, a recent best-evidence consensus statement found that 20% to 25% of patients develop recession two to five years after orthodontic treatment. Higher incidences of dehiscence and recession were noted in patients with thin phenotypes or teeth moved beyond the alveolar housing.27
Even if tooth- and site-related conditions are amenable to mucogingival surgery, a patient’s medical or dental history can prove otherwise. Those with increased bleeding risk due to medications or illness are less-than-ideal candidates for free soft tissue autografting out of concern for uncontrolled bleeding and hospitalization. Different hemostatic agents, palatal stents, and plasminogen-inhibiting mouthrinses should be readily available for these patients during the perioperative period. Additionally, a minimally invasive approach using an allograft or xenograft should be considered.

Maintenance frequency can also impact surgical decision-making. In a split-mouth study of patients receiving free soft tissue autografts for areas of inadequate gingiva, grafted sites that were not maintained for five years showed no inflammation or further recession,28 demonstrating these grafts may be an appropriate choice for those with poor oral hygiene or irregular compliance. Patients must not only have clear expectations of their anticipated results, but also understand the potential complications and need for ongoing care.
CASE REPORT
The following case outlines the steps taken to correct soft tissue deficiencies by means of a connective tissue graft. A 44-year-old male presented to the graduate periodontics clinic at the University of Texas Health Science Center San Antonio School of Dentistry interested in root coverage and sensitivity reduction for tooth #25 (Figure 5 through Figure 9). The patient had no significant medical history. After a thorough evaluation and review of various techniques and materials, a surgical treatment plan was developed, and consent was obtained. Treatment was performed using IV conscious sedation. The treatment plan included:
- Connective tissue grafting of tooth #25 via tunneling for root coverage and increased tissue thickness
- De-epithelialization and vestibuloplasty if adequate root coverage was not initially achieved

After initial findings were charted (Table 1), root coverage was determined to be the primary goal, so an appropriate case workflow was developed. Due to limited vestibular depth, minimal attached tissue, thin phenotype, labial tooth position, and fair oral hygiene, increasing keratinized tissue width first would also have been an appropriate treatment goal. A free soft tissue autograft with a delayed coronally advanced flap could have been performed. Therein lies the struggle most surgeons face during their daily mucogingival decision-making. In either approach, the patient was not guaranteed complete root coverage because of these site-related risk factors.
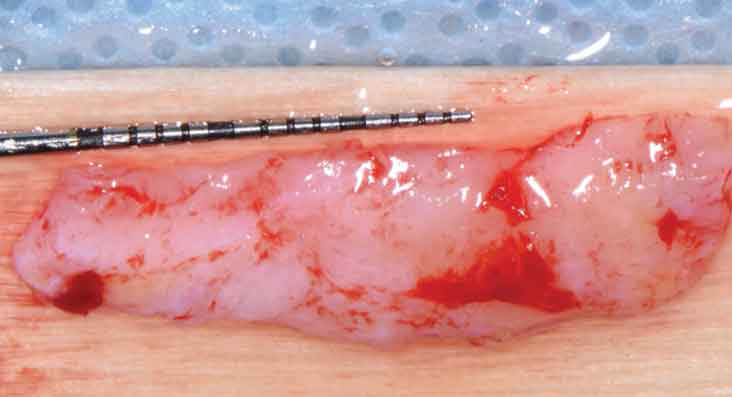
The recipient site was carefully prepared with tunneling instruments from teeth #23 to 27 to achieve partial thickness dissection. An 8-mm tall by 25-mm wide by 1.5-mm thick connective tissue graft was harvested from the right palate using a single incision. The graft was tunneled from teeth #23 to 27 and stabilized with a combination of 6-0 polypropylene simple interrupted and sling sutures after coronal tissue advancement. Gauze pressure was applied to the palatal wound and multiple layers of a cyanoacrylate adhesive were applied along the incision line for hemostasis.
The patient returned for weekly follow-ups until his final recall at eight weeks postoperatively and was instructed to continue prophylaxis every six months. After achieving 90% root coverage in a compromised scenario, the decision was made not to proceed with additional surgery to minimize scarring or further recession.

SUMMARY
It is important for patients to understand that complete or even partial root coverage is not always possible given different tooth-, site- and patient-related risk factors. With greater tooth retention and rising life expectancy, gingival recession and its destructive sequelae will require close attention and treatment. Techniques to modify phenotype, cover exposed roots, or increase keratinized tissue width have also evolved with the introduction of various allograft and xenograft materials. The predictability of these procedures should be discussed with patients as part of the initial exam based on their unique presentation. When diagnosed early and treated appropriately, mucogingival defects can be managed successfully.
Key Takeaways
- Gingival recession and a minimal or absent band of attached keratinized tissue are among the leading mucogingival problems today.
- Even with advances in soft tissue grafting materials and techniques, choosing the most appropriate and predictable surgical approach for a given case is one of the most disputed facets of periodontics.
- The potential for root coverage or gain in keratinized tissue width largely depends on various tooth-, site- and patient-related risk factors.3
- When diagnosed early and treated appropriately, mucogingival defects can be successfully managed and appropriate clinical expectations established for the patient.
References
- Kassab MM, Cohen RE. The etiology and prevalence of gingival recession. J Am Dent Assoc. 2003;134:220–225
- Chambrone L, Tatakis DN. Long‐term outcomes of untreated buccal gingival recessions: a systematic review and meta‐analysis. J Periodontol. 2016;87:796–808.
- Kim DM, Neiva R. Periodontal soft tissue non-root coverage procedures: a systematic review from the AAP regeneration workshop. J Periodontol. 2015;86(Suppl 2):S56–S72.
- Cortellini P, Bissada NF. Mucogingival conditions in the natural dentition: narrative review, case definitions, and diagnostic considerations. J Periodontol. 2018;89(Suppl 1):S204–S213.
- Pini-Prato G. The Miller classification of gingival recession: limits and drawbacks. J Clin Periodontol. 2011;38:243–245.
- Cairo F, Nieri M, Cincinelli S, Mervelt J, Pagliaro U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: an explorative and reliability study. J Clin Periodontol. 2011;38:661–666.
- Cairo F, Pini‐Prato GP. A technique to identify and reconstruct the cementoenamel junction level using combined periodontal and restorative treatment of gingival recession. A prospective clinical study. Int J Periodontics Restorative Dent. 2010;30:573–581.
- Pini-Prato G, Franceschi D, Cairo F, Nieri M, Rotundo R. Classification of dental surface defects in areas of gingival recession. J Periodontol. 2010;81:885–890.
- Fan J, Caton JG. Occlusal trauma and excessive occlusal forces: narrative review, case definitions, and diagnostic considerations. J Periodontol. 2018;89(Suppl 1):S214–S222.
- Bartlett DW, Shah P. A critical review of non‐carious cervical (wear) lesions and the role of abfraction, erosion, and abrasion. J Dent Res. 2006;85:306–312.
- Rasperini G, Acunzo R, Pellegrini G, et al. Predictor factors for long‐term outcomes stability of coronally advanced flap with or without connective tissue graft in the treatment of single maxillary gingival recessions: 9 years results of a randomized controlled clinical trial. J Clin Periodontol. 2018;45:1107–1117.
- Agudio G, Chambrone L, Selvaggi F, Pini‐Prato GP. Effect of gingival augmentation procedure (free gingival graft) on reducing the risk of non‐carious cervical lesions: a 25‐ to 30‐year follow‐up study. J Periodontol. 2019;90:1235–1243.
- Gordon HP, Sullivan HC, Atkins JH. Free autogenous gingival grafts. II. Supplemental findings — histology of the graft site. Periodontics. 1968;6:130–133.
- Chambrone L, Pini-Prato GP. Clinical insights about the evolution of root coverage procedures: the flap, the graft, and the surgery. J Periodontol. 2019;90:9–15.
- Cairo F, Cortellini P, Nieri M, et al. Coronally advanced flap and composite restoration of the enamel with or without connective tissue graft for the treatment of single maxillary gingival recession with non–carious cervical lesion. A randomized controlled clinical trial. J Clin Periodontol. 2020;47:362–371.
- Hwang D, Wang HM. Flap thickness as a predictor of root coverage: a systematic review. J Periodontol. 2006;77:1625–1634.
- Allen EP, Miller JD Jr. Coronal positioning of existing gingival: short term results in the treatment of shallow marginal tissue recession. J Periodontol. 1989;60:316–319.
- Tavelli L, Barootchi S, Cairo F, et al. The effect of time on root coverage outcomes: a network meta-analysis. J Dent Res. 2019;98:1195–1203.
- Pini-Prato GP, Franceschi D, Cortellini P, Chambrone L. Long‐term evaluation (20 years) of the outcomes of subepithelial connective tissue graft plus coronally advanced flap in the treatment of maxillary single recession‐type defects. J Periodontol. 2018;89:1290–1299.
- Lang NP, Löe H. The relationship between the width of keratinized gingiva and gingival health. J Periodontol. 1972;43:623–627.
- Saletta D, Pini-Prato G, Pagliaro U, et al. Coronally advanced flap procedure: is the interdental papilla a prognostic factor for root coverage? J Periodontol. 2001;72:760–766.
- Reiser GM, Bruno JF, Mahan PE, Larkin LH. The subepithelial connective tissue graft palatal donor site: anatomic considerations for surgeons. Int J Periodontics Restorative Dent. 1996;16:130–137.
- Dai A, Huang JP, Ding PH, Chen LL. Long‐term stability of root coverage procedures for single gingival recessions: a systematic review and meta‐analysis. J Clin Periodontol. 2019;46:572–585.
- Matter J, Cimasoni G. Creeping attachment after free gingival grafts. J Periodontol. 1976;47:574–579.
- Ryder MI, Couch ET, Chaffee BW. Personalized periodontal treatment for the tobacco– and alcohol-using patient. Periodontol 2000. 2018;78:30–46.
- de Oliveira DW, Oliveira‐Ferreira F, Flecha OD, Gonçalves PF. Is surgical root coverage effective for the treatment of cervical dentin hypersensitivity? A systematic review. J Periodontol. 2013;84:295–306.
- Kao RT, Curtis DA, Kim DM, et al. American Academy of Periodontology best evidence consensus statement on modifying periodontal phenotype in preparation for orthodontic and restorative treatment. J Periodontol. 2020;91:289–298.
- Kennedy JE, Bird WC, Palcanis KG, Dorfman HS. A longitudinal evaluation of varying widths of attached gingiva. J Clin Periodontol. 1985;12:667–675.
The author has no commercial conflicts of interest to disclose.
From Decisions in Dentistry. May 2021;7(5)18,21-23.
