
 AlessandroPhoto / iStock / Getty Images Plus
AlessandroPhoto / iStock / Getty Images Plus
Screw- Vs Cement-Retained Prostheses in Implant Therapy
Both screw- and cement-retained prostheses are acceptable treatment options for single and multiple fixed implant restorations. However, there is debate over which is the better option in the long term.
A cement-retained prosthesis has several advantages over a screw-retained prosthesis in terms of cost, ease of fabrication, lack of an access hole (advantageous for a narrow-diameter implant with limited restorative space), and ability to change the angulation of the implant axis by utilizing angled abutments.1,2 A systematic review by Wittneben et al3 compared cement- and screw-retained implant-supported restorations. The 5-year cumulative survival rate of cement-retained reconstruction was 96.03%, while it was 95.55% for screw-retained prostheses. There was no statistically significant difference between the two groups. However, this study revealed that screw-retained fixed prostheses exhibited a slightly lower biological complication rate, such as the presence of fistula/suppuration rates. In addition, the major negative aspect of cement retention is the presence of residual cement following delivery of the prosthesis that can lead to peri-implant mucositis and peri-implantitis. A clinical trial has shown that approximately 80% of the cement-retained implant prostheses with radiological and clinical signs of peri-implant disease had subgingival residual cement.4 Thus, it was concluded that residual cement might play an important role as a bacterial reservoir, leading to soft tissue irritation that contributes to peri-implant tissue breakdown.
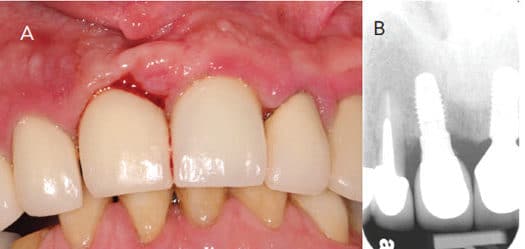
In this case (Figure 1), the patient presented to a graduate clinic with 5-mm to 7-mm probing depths and bleeding on probing around implant #8. Clinically, tissue inflammation was noted on the gingival margin of #8. Upon examination, residual cement was noted in the subgingival area. This represents the obvious etiologic factor for iatrogenic peri-implant disease (Figure 2). To reduce complications associated with the presence of residual cement, clinicians should consider using screw retention as the connection of choice.2 Linkevicius5 investigated the relationship between crown margin position and undetected residual cement. This study revealed that more remnant cement was found on sites with a deeper subgingival margin area. In addition, the majority of excess cement was not found with radiographic examination. If implant position is compromised and a screw-retained connection cannot be used, utilizing a custom abutment to place the crown margin < 2 mm submarginally is recommended.

References
- Shadid R, Sadaqa N. A comparison between screw- and cement-retained implant prostheses. A literature review. J Oral Implanto 2012;38:298–307.
- Wittneben JG, Joda T, Weber HP, Brägger U. Screw retained vs. cement retained implant-supported fixed dental prosthesis. Periodontol 2000. 2017;73:141–151.
- Wittneben JG, Millen C, Brägger U. Clinical performance of screw- versus cement-retained fixed implant-supported reconstructions — a systematic review. Int J Oral Maxillofac Implants. 2014;29 (Suppl):84–98.
- Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 2009;80:1388–1392.
- Linkevicius T, Vindasiute E, Puisys A, Linkeviciene L, Maslova N, Puriene A. The influence of the cementation margin position on the amount of undetected cement. A prospective clinical study. Clin Oral Implants Res. 2013;24:71–76.
This information originally appeared in Hamada Y, Hill K, Chang J, John V. Addressing risks of implant complications. Decisions in Dentistry. 2017;3(10):14–21.
