

Treatment Approaches for Patients With Sjögren’s Syndrome
Oral complications among this population can be managed to prevent caries, treat oral fungal infections, and increase comfort.
Oral complications among this population can be managed to prevent caries, treat oral fungal infections, and increase comfort.
Sjögren’s syndrome (SS) is a chronic inflammatory autoimmune disease that affects the salivary and lacrimal glands, resulting in the classic presentation of dry eyes and dry mouth (sicca symptoms). The clinical spectrum of SS is broad. One patient with SS may experience only mild symptoms, while another may present with sicca symptoms, as well as significant joint pain and fatigue. Individuals with SS may also experience severe systemic manifestations, including vasculitis, interstitial lung disease, glomerulonephritis, arthritis and lupus. Significant neurological dysfunction may also be present.
Patients with SS are divided into two classifications: Primary SS occurs when the patient only has symptoms of SS, whereas secondary SS is the diagnosis for patients who have another autoimmune disease, in addition to SS.1 Between 1 million and 2 million individuals in the United States have SS1 and it is more common in women (90%) than men (10%).2
The diagnosis can be challenging. After the initiation of symptoms, individuals sometimes wait six to nine years before a diagnosis of SS is reached.3 This is often stressful for patients because they experience symptoms, but the cause remains unclear. Oral health professionals are in a unique position to identify, evaluate and manage symptoms of dry mouth, as well as reduce delays in SS diagnosis. This is because many individuals have regular dental care prior to being diagnosed with SS.4 In one study, for example, patients with SS spent nearly three times more on out-of-pocket dental expenses and had 1.7 more dental visits than subjects without SS.2 Patients who exhibit clinical symptoms of dry mouth and dry eyes should be referred to their primary care physicians for further evaluation and blood tests (anti-SSA, anti-SSB, rheumatoid factor, and antinuclear antibody).5
SALIVARY FLOW
Saliva is mainly water but also contains electrolytes, digestive enzymes, antimicrobial agents, buffering agents and functional proteins. Thus, saliva plays an important role in maintaining oral health by initiating digestion, buffering pH, and protecting, lubricating and repairing the oral mucosa. It also facilitates taste. Consequently, a reduction in salivary flow can result in oral mucosal infections, dental caries, and difficulty with taste and swallowing.
Patients who exhibit clinical symptoms … should be referred to their primary care physicians for further evaluation and blood tests
Individuals typically notice xerostomia symptoms when salivary flow rates drop to less than 50% of normal levels.6 While the majority of patients with SS experience significantly reduced salivary flow, some may have salivary function within normal range. To determine whether a patient’s salivary flow is impaired, oral health professionals should ask:7
- Do you feel the saliva in your mouth is too little or too much — or you do not notice it?
- Does your mouth feel dry when eating?
- When eating, do you sip liquids to aid in swallowing?
An affirmative answer to one or more of these questions may indicate dysfunctional salivary glands.
The next step in evaluating patients’ salivary production is to have them expectorate into a preweighed tube, following the Sjögren’s International Collaborative Clinical Alliance protocol.8 Another option is to refer patients to a hospital setting for salivary scintigraphy performed by a physician. This test involves the injection of a small amount of a radioactive tracer, followed by evaluation under a gamma scintillation camera that allows the operator to watch the tracer move through the salivary glands. Patients are also given a substance that encourages elimination through the salivary glands, and the camera captures additional images that are used for comparison.9
MANAGING ORAL COMFORT
The sensation of dry mouth and dry tongue (Figure 1) occurs when the oral soft tissues do not glide over the hard tissues. The tongue adheres to the palate, while labial and buccal mucosa adhere to the teeth. In the most severe cases of oral dryness, oral health professionals may hear a “clicking” or “kissing” sound when the patient speaks. This is the sound of the oral soft tissue detaching from the dental structures. The presence of lipstick on the anterior maxillary teeth may also be a symptom of dry mouth.

Patients with SS need to maximize the amount of saliva present in the oral cavity. To prevent saliva from evaporating, patients should try to breathe through the nose, and keep the mouth closed as much as possible.10
Improving the oral comfort of individuals with SS is important. During dental appointments, patients must keep their mouths open, while suction is used to remove residual saliva, and already dry, cracked lips may be retracted to provide access for the procedure. To minimize potential discomfort, lips may be moisturized. If the lips are extremely dry, place water or water-based emollient on the lips before applying any oil-based material. The oil-based material seals the waterbased moisture onto the lips. During and after the dental procedure, water may be sprayed or artificial saliva may be applied to the palate and oral mucosa. The sensation of dry mouth may be caused by localized areas of mucosal dryness, especially on the palate.6
At home, patients may implement three main strategies to increase oral comfort: use of wetting agents, nonpharmacologic and pharmacologic methods to stimulate saliva, and careful management of existing saliva. The use of wetting agents, such as saliva substitutes and water, helps the oral soft tissues glide over the palate and teeth. Patients should apply the artificial saliva throughout the oral cavity, but especially on the hard palate. The selection of artificial saliva products is based on preference. Some products provide information about their pH levels, which is helpful because patients with SS may be especially susceptible to the demineralizing effect of low-pH products.11 Some patients may prefer water over commercial products. A small amount of olive or other oil (1⁄4 teaspoon to ½ teaspoon per 16 oz. of water) may be added to a bottle of water that is sipped throughout the day.
Sucking sugar-free hard candies or using sugar-free chewing gum stimulates salivary production. Gum and hard candies are available with baking soda to neutralize acid, xylitol to help prevent caries, and green tea to provide antioxidant benefits. Gleeking, a process in which the tongue and associated musculature are used to stimulate saliva production from the submandibular/sublingual glands, may be helpful in moisturizing the oral cavity and palate. Alternatively, patients can massage their salivary glands using their hands to gently push saliva from the parotid glands or submandibular/sublingual glands into the oral cavity.12 The expressed saliva can be used to wet dry areas of the oral mucosa and palate. The majority of patients with SS have some residual salivary function. The goal is also to maximize the functions of the saliva produced by not allowing it to evaporate through mouth breathing, and making sure the fluid is utilized effectively by swirling to areas of dryness before swallowing.
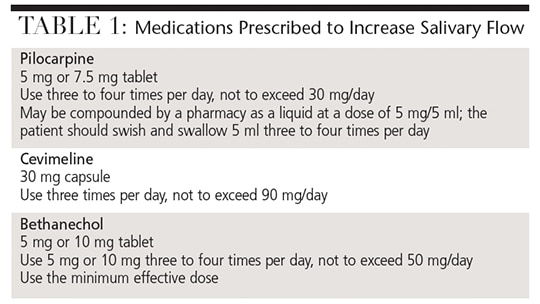
Three medications are prescribed to increase salivary flow via stimulation of the muscarinic receptors: pilocarpine, cevimeline and bethanechol (Table 1, page 18). The benefits of saliva include neutralization of pH, caries prevention, initiation of digestion, and antibacterial/viral and antifungal activity. It is unknown if the use of these medications will actually prevent caries and decrease intraoral infections. Many, but not all, patients obtain significant relief from xerostomia symptoms with these drugs. The few studies comparing these parasympathomimetic medications show that some patients prefer one medication over the others, and that selection of the best medication may be a simple case of preference.13–15
CARIES PREVENTION
Patients with dry mouth are at increased risk for dental caries. They should be educated about the role of sugar in the caries process, and have their toothbrushing technique periodically reviewed using a plaque-disclosing agent. A dental chart indicating the areas of the dentition where plaque is not being properly removed — and the location of any incipient caries — gives patients a visual reminder of the importance of plaque removal and where fluoride should be placed.
The use of topical fluoride is critical to caries prevention efforts in this population. Recent guidelines sponsored by the Sjögren’s Syndrome Foundation (Sjogrens.org) state that topical fluoride should be used in patients with SS and dry mouth.16 This recommendation is for individuals who complain of dry mouth, regardless of whether their salivary production is low. The fluoride recommendation reflects a trend toward a more aggressive approach to using topical fluoride in individuals who report xerostomia symptoms, especially if they have exposed root surfaces (which are highly susceptible to decay). Limited but encouraging data suggest the root caries process can be slowed, or even reversed, with the application of 5% fluoride varnish17 or the recently introduced 1% chlorhexidine varnish.18
The use of topical fluoride is critical to caries prevention efforts in this population
The use of xylitol, either ingested or applied topically, has been recommended to help prevent decay.16 The rationale is that acid-producing bacteria in the oral cavity cannot metabolize the sugar alcohol, causing a shift in the intraoral flora away from caries promotion. The evidence for use of xylitol in caries prevention comes primarily from research with children who have high caries rates. The literature supporting the use of chlorhexidine to alter the oral microbiota to prevent caries is considered weak.16 Current recommendations for individuals at “high or extreme risk” for caries suggest that patients rinse with 0.12% chlorhexidine once per day for a week each month to decrease the bacterial load.19
Nonfluoride remineralizing agents — such as amorphous calcium phosphate (ACP), casein phosphopeptide-ACP, calcium sodium phosphosilicate and tricalcium phosphate — deliver calcium and phosphate to the tooth surface and enhance the function of fluoride. The available research was evaluated for the use of nonfluoride remineralizing agents in individuals with dry mouth and/or SS, but the evidence for use of these agents in preventing caries in such patients was deemed weak.16 These therapeutic agents should be considered adjunctive measures to enhance the function of fluoride and to help treat early, noncavitated lesions.
The oral buffering capacity in patients with reduced or no salivary production is compromised. These individuals may have an intraoral pH that is more acidic, which may facilitate the demineralization/caries process. Additional acidic insults may come from a diet heavy in carbonated drinks, wine and juice, and the presence of gastric reflux. To counter these acidic insults and promote remineralization, patients should be advised to rinse with water after each meal to clear away and dilute the acidic material, and use sugar-free gum or sugar-free candy to increase salivary flow that can buffer and clear debris. Commercial products may be used to help patients with intraoral buffering.
TREATMENT OF ORAL CANDIDIASIS
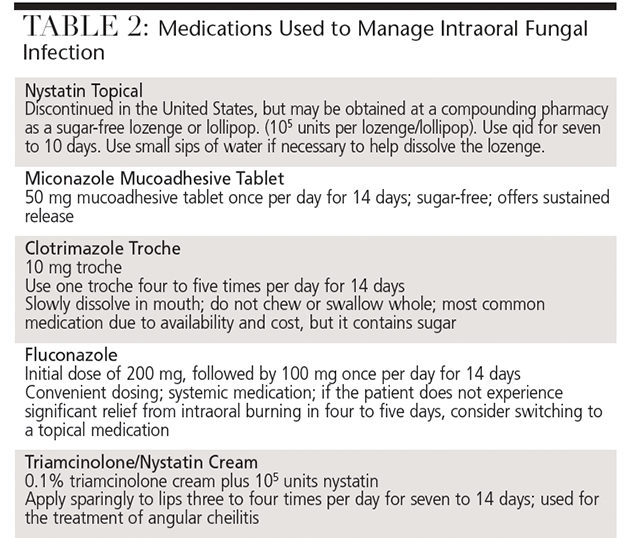
Oral fungal infection is the most common soft tissue problem affecting individuals with SS. Typically, patients will complain of a burning sensation on the tongue and specific areas of the oral mucosa. The location of the sensation will correlate visually with mucosal erythema. Angular cheilits may occur by itself or with an intraoral infection. Treatment is complicated when patients with intraoral fungal infections also wear dentures, as the prostheses will also need to be treated. If the denture is metal-free, it may be soaked overnight in a diluted 1:10 solution of sodium hypochlorite and water. If the denture contains metal, it should soaked overnight or twice daily in a chlorhexidine solution. The treatment endpoint is two to three days after the burning and erythema resolve. Medications can also be used to manage intraoral infections (Table 2).
KEY TAKEAWAYS
- A chronic inflammatory autoimmune disease, Sjögren’s syndrome (SS) affects the salivary and lacrimal glands, resulting in the classic presentation of dry mouth and dry eyes.
- Patients who exhibit clinical symptoms of dry mouth and dry eyes should be referred to their primary care physicians for further evaluation.5
- At home, patients may implement three main strategies to increase oral comfort: use of wetting agents, stimulation of the salivary glands via pharmacologic and nonpharmacologic means, and careful management of existing saliva.
- While patients with dry mouth have increased caries risk, oral fungal infection is the most common soft tissue problem affecting individuals with SS.
- Guidelines sponsored by the Sjögren’s Syndrome Foundation note that evidence supporting topical fluoride use is strong, and suggest that fluoride be incorporated into caries prevention regimens for patients with SS who complain of dry mouth.16
CONCLUSION
Oral health professionals are well-positioned to identify and manage oral complications from SS. Improving oral comfort in this population includes educating patients about why their oral cavities feel dry, and trying various strategies for the daily management of dry mouth. Some patients may be soothed by sipping water throughout the day, while others prefer saliva-boosting medications. In addition to maintaining a healthy diet and practicing excellent oral hygiene, fluoride exposure remains key to caries prevention in this population. Fortunately for patients and clinicians, an increasing array of adjunctive products is available to support oral comfort and caries prevention efforts.
REFERENCES
- Kruszka P, O’Brian RJ. Diagnosis and management of Sjögren syndrome. Am Fam Physician. 2009;79:465–470.
- Segal B, Bowman SJ, Fox PC, et al. Primary Sjögren’s syndrome: health experiences and predictors of health quality among patients in the United States. Health Qual Life Outcomes. 2009;7:46.
- Kassan SS, Moutsopoulos HM. Clinical manifestations and early diagnosis of Sjögren syndrome. Arch Intern Med. 2004;164:1275–1284.
- Lu MC, Jheng CH, Tsai TY, Koo M, Lai NS. Increased dental visits in patients prior to diagnosis of primary Sjögren’s syndrome: a population-based study in Taiwan. Rheumatol Int. 2014;34:1555–1561.
- Shiboski SC, Shiboski CH, Criswell L, et al. American College of Rheumatology classification criteria for Sjögren’s syndrome: a data-driven, expert consensus approach in the SICCA cohort. Arthritis Care Res. 2012;64:475–487.
- Dawes C. How much saliva is enough for avoidance of xerostomia? Caries Res. 2004;38:236–240.
- Fox PC, Busch KA, Baum BJ. Subjective reports of xerostomia and objective measures of salivary gland performance. J Am Dent Assoc. 1987;115:581–584.
- University of California, San Francisco. Sjögren International Collaborative Clinical Alliance. Available at: sicca-online.ucsf.edu. Accessed October 7, 2016.
- Johns Hopkins Medicine Sjögren’s Syndrome Center. Salivary Gland Function Scan. Available at: hopkinssjogrens.org/disease-information/diagnosis-sjogrenssyndrome/salivary-gland-function-scan. Accessed October 7, 2016.
- Dawes C. Physiological factors affecting salivary flow rate, oral sugar clearance, and the sensation of dry mouth in man. J Dent Res. 1987;66:648–653.
- Featherstone, JD. The science and practice of caries prevention. J Am Dent Assoc. 2000;131:887–899.
- Sjögren’s Syndrome Foundation. Available at: sjogrens.org/home/aboutsjogrens/brochures-and-fact-sheets. About Sjögren’s. Accessed October 7, 2016.
- Chainani-Wu N, Gorsky M, Mayer P, Bostrom A, Epstein JB, Silverman S Jr. Assessment of the use of sialogogues in the clinical management of patients with xerostomia. Spec Care Dentist. 2006;26:164–170.
- Noaiseh G, Baker JF, Vivino FB. Comparison of the discontinuation rates and sideeffect profiles of pilocarpine and cevimeline for xerostomia in primary Sjögren’s syndrome. Clin Exp Rheumatol. 2014;32:575–577.
- Wu AJ. Management of salivary hypofunction in Sjögren’s syndrome. Current Treatment Options in Rheumatology. 2015;1(3):255–268.
- Zero DT, Brennan MT, Daniels TE, et al. Sjögren’s Syndrome Foundation (SSF) Clinical Practice Guidelines for Oral Disease Management: Caries Prevention. J Am Dent Assoc. 2016;147:295–305.
- Weyant RJ, Tracy SL, Anselmo TT, et al. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013;144:1279–1291.
- Slot DE, Vaandrager NC, Van Loveren C, Van Palenstein Helderman WH, Van der Weijden GA. The effect of chlorhexidine varnish on root caries: a systematic review. Caries Res. 2011;45:162–173.
- Jenson L, Budenez AW, Featherstone JDB, Ramos-Gomez FJ, Spolsky VW, Young DA. Clinical protocols for caries management by risk assessment. J Calif Dent Assoc. 2007;35:714–723.
Featured Photo Courtesy of DECADE3D/ISTOCK/ THINKSTOCK
From Decisions in Dentistry. November 2016;2(11):16–18, 21-22.
