

The Case for Implant-Retained, Tissue-Supported Overdentures
This approach is a viable alternative to conventional complete dentures and complex, fixed, implant-supported prostheses.
This approach is a viable alternative to conventional complete dentures and complex, fixed, implant-supported prostheses
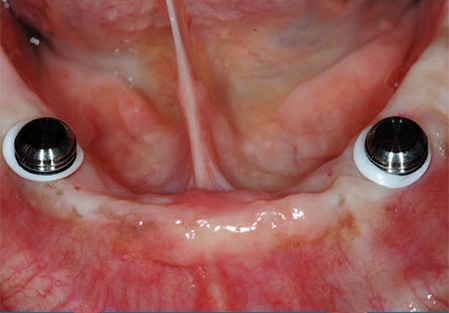
Implant-retained, tissue-supported mandibular overdentures are becoming the standard of care for edentulous patients.1 Implant-retained, tissue-supported overdentures are considered an alternative to conventional complete dentures, as well as complex, fixed, implant-supported prostheses.2 The implant-retained overdenture is secured by either a bar/retainer combination, or individual attachments that are fitted to each implant fixture (Figure 1 through Figure 3). These act as both retentive components and stabilizing elements for the complete denture.

Patients with extreme mandibular resorption usually develop chronic sore spots due to lack of adequate stability and retention of conventional dentures. These patients can benefit from a simple overdenture retained by two implants with uncomplicated retention devices. The improved retention and stability help relieve the typical sore spots caused by movement of conventional prostheses, and can often alleviate the “removable” feeling of complete dentures. Patients with implant-retained overdentures have reported increased function and comfort.3
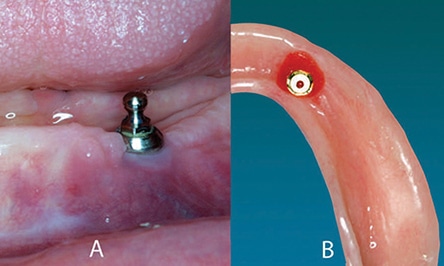
devices in place on the retentive
abutments.
The severe resorption patterns seen in denture patients will often require tissue support for optimum function and esthetics; these are provided by conventional flanges and acrylic resin bases, and cannot be duplicated by fixed, implant-supported prostheses. These overdentures can easily be removed by the patient and, by virtue of the implant components’ simple design, hygiene procedures are usually easier for the patient to perform.4 In addition, the less complex, removable overdentures are more economical due to the limited number of implants needed and the lower cost of components. However, because there are still changes in the supporting structures under the implant-retained, tissue-supported overdenture, these elements must be monitored and corrected if the prostheses become unstable. Even though the implants themselves stabilize the bone and soft tissue in their immediate vicinity, relines or rebases will be needed on a periodic basis to compensate for the areas that remain tissue supported.5
TREATMENT PLANNING
For the most part, treatment planning for implant-retained overdentures is no different than for conventional dentures. The exceptions are the timing of implant placement, determining the implant site, modification of the prostheses for the retentive components, and the increased cost of treatment.

devices after transfer and bonding to the
prosthesis
The patient considering implant-retained, tissue-supported dentures has often been wearing prostheses for many years. If the patient has existing complete dentures, they must be evaluated to determine if they will be usable as temporary dentures during the healing process after implant placement. When inspecting the existing prostheses, the clinician should evaluate the fit of the intaglio surfaces, esthetic and phonetic contours of the anterior teeth, vertical dimension of occlusion, type of posterior occlusion (intended function and wear), and the closure position in reference to the centric-relation position.
Occasionally, the existing dentures meet all of the requirements for a final set of implant overdentures and can be successfully retrofitted to the new implant components. More commonly, however, the patient will require a set of complete dentures that (1) are adequate from esthetic and functional aspects, (2) will allow use as a guide for implant placement, (3) can serve as temporary prostheses during healing, and (4) function as a guide for the fabrication of the new, implant-retained, tissue-supported overdentures. On the other end of the spectrum will be patients whose existing dentures are not useful in any manner due to bone resorption, loss of vertical dimension, poor esthetics, and the inability to refit them effectively. These patients may require new denture fabrication to the point of the esthetic and functional try-in to establish the proper information for successful implant placement. In some cases, the prostheses should be finished and the patient made comfortable with the new dentures before proceeding with the implant placement and the retrofit to add the retentive components.
Available restorative space is an important factor that must be assessed during treatment planning of implant overdentures and before implant placement. Restorative space is the three-dimensional oral space available to receive the proposed prosthodontic restoration.6 It includes the vertical and horizontal space required for the implant attachments, a denture base of adequate thickness, and denture teeth. Implant-retained overdentures with individual attachments typically require 10 to 12 mm of vertical restorative space from the incisal edge to the implant platform,7 and 9 mm of horizontal space.8 Insufficient restorative space may lead to inadequate esthetics and phonetics, or mechanically compromised prostheses. Any areas that need correction prior to implant placement should be scheduled for the appropriate procedure(s) as soon as possible.
The final occlusal scheme for a maxillary complete denture opposing a mandibular implant-retained/tissue-supported overdenture should be based on sound complete denture philosophies.9 Occlusal schemes should avoid anterior contact in centric relation, and either support anterior contact in excursive positions — with a balanced posterior occlusion — or avoid anterior dislodging forces by using a nonbalanced scheme with no vertical overlap of the anterior teeth. Lingualized occlusal concepts should be strongly considered for implant-retained, tissue-supported overdentures.10

IMPLANT EVALUATION
After arriving at the prosthodontic treatment plan and completing the conventional denture workup, the patient should be evaluated for implant placement. The patient’s medical conditions (such as diabetes or chronic and acute diseases that affect healing potential) and personal habits (e.g., smoking) that may affect the success of the implant fixture placement must be assessed. The recipient sites should be evaluated for adequate quantity and quality of bone to complete fixture placement. Conventional radiographs and computed tomograms made with standardized size markers are needed to complete the diagnosis. The radiographic evaluation should be augmented by a physical examination of ridge topography and assessment of the keratinized gingiva in the implant zone.11

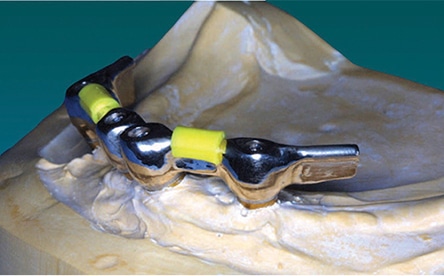
The mandible typically requires two implants placed in the anterior symphyseal region equidistant from the midline. These implants can be joined by a metal bar or used as single retainers. With a bar substructure, various clips or other types of retentive components can be used for retention (Figure 4). Selection of the attachment system depends on various factors that must be recognized early in the treatment planning process. These include implant angulation, need for cross-arch stabilization, size of the prosthesis, available restorative space, opposing arch, oral hygiene and patient’s financial situation.12 Often, the support provided by the extended bar substructure may support the overdenture in the premolar region, which removes a great deal of load from the tissue (Figure 5 and Figure 6). If single components are used, they usually have some type of retention/support system, such as a ball/O-ring, magnets or other design (Figures 7A and 7B). With reasonable tissue support, many patients find the simplest design adequate for their needs (Figure 1 through Figure 3).
If the number of implants is to be kept at a minimum, the ability of the soft tissue to support part of the load of the implant-retained, tissue-supported overdenture is critical. Soreness problems associated with conventional dentures are more likely related to stability problems than vertical forces against the ridge. The lateral stability of the overdenture — provided by the two individual attachments — will make a marked improvement in patient comfort. In patients with severe mandibular bone resorption and hyperesthesia caused by the pressure effect of the denture, the number of implants should be increased to remove the load from the alveolar tissue.

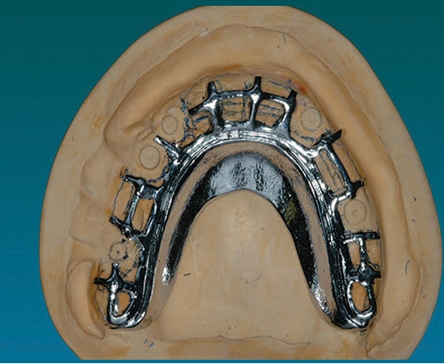
If a maxillary implant-retained, tissue-supported overdenture is planned, the maxilla is typically treated with three to four implants, along with a bar substructure for support and retention.13 However, many patients function well with unconnected implants using simpler retentive component designs14 (Figure 8 and Figure 9). If retention is sufficient, the palate may be removed from the maxillary denture for patient comfort. If the palate is removed, the structure may be weakened, however, and a metal framework may need to be part of the prosthesis design (Figure 10).

After careful assessment of the patient’s condition, the treatment plan can be formulated. Treatment may need to be phased in order to evaluate the effect of each step in improving the patient’s ability to function with his or her prostheses. For example, once a mandibular denture is stabilized by the two implant attachments, the opposing arch may offer improved function because the increased stability of the mandibular denture benefits the entire system. Many treatment plans should begin by addressing the mandible first, followed by reevaluating the condition of the maxilla.15
CLINICAL PROCEDURES
This manuscript will limit the clinical discussion to single retentive components for the mandible, and will not discuss the bar substructure technique.
Retrofitting Existing Prostheses: Patients with existing prostheses that are optimal in design and function can have them retrofitted to the new implant components. The prostheses will often need a soft liner added to the areas of the fixture surgical sites, and the patient can wear them during the integration phase of the implants. At the second-stage surgery, the soft liner can be modified to accommodate the retentive abutment component or a healing cap, depending on the treatment plan. If significant soft tissue changes occurred during either surgical phase, the denture may need to be relined with conventional acrylic before proceeding with implant component incorporation.
The single implant retentive components can easily be added to the existing prosthesis. The abutment length is determined by the tissue height, as measured from the top of the implant fixture to approximately 1 mm above the tallest gingival margin. The retentive abutment is placed on the implant and torqued according to the manufacturer’s instructions. The retentive component that will be attached to the denture is placed on the abutment, and the intaglio surface of the existing denture is modified to provide passive fit over the abutments and against the tissue; the clinician must allow adequate clearance for the retentive components. The space between the tissue and retentive component should be blocked to prevent the acrylic resin from locking the denture onto the abutment. Autopolymerizing resin is used to pick up the retentive component in the existing denture (Figure 11 and Figure 12). The patient’s existing occlusal vertical dimension and occlusal position are maintained during the pick-up procedure by placing the patient in light contact in the proper closure position, without compression of the soft tissue.


New Prostheses: In cases in which patients do not have adequate existing dentures, new prostheses will need to be completed through the esthetic and functional try-in stage. The new prostheses will be used to evaluate the space available for implant components. This assessment will also help the clinician choose the appropriate retentive system.
In addition to the pick-up procedure, the single implant retentive components can be added to new prostheses during the denture processing procedure. The final denture impression is made using implant-level impression copings, and the subsequent master cast is fabricated with abutment analogs. The record base and occlusion rim are fabricated to fit on the abutment to stabilize the record base during the jaw relations appointment. Once the esthetic and functional try-in is completed, the processing step is accomplished after proper block out of the abutment analogs and the addition of the retentive components to the abutment analogs. The exact procedure may vary by manufacturer, thus, clinicians are advised to check the technical procedure manual.
Guidelines provided by the American College of Prosthodontists regarding patient recall, professional maintenance and at–home maintenance should be emphasized.16 Patients with implant-retained overdentures should have a professional examination every six months as a lifelong regimen. Professional biological maintenance should include an extraoral and intraoral health and dental examination, oral hygiene instructions, and hygiene instructions for the implant abutments and prostheses. Clinicians should use chlorhexidine gluconate oral topical agent when antimicrobial effect is needed in the clinical environment. Oral health professionals should use cleaning instruments compatible with the implants, abutments and prostheses. Implant-retained overdentures should be professionally cleaned extraorally using accepted mechanical and chemical cleaning methods.
Professional mechanical maintenance should include a detailed examination of the prostheses, as well as intraoral and extraoral prosthetic components. Patients should be advised about anticipated problems that could compromise function of the restoration. Clinicians should recommend and perform adjustment, repair, replacement or remake of any parts of the prostheses and prosthetic components that could impair function.
In regard to at-home maintenance, clinicians should advise patients to clean their intraoral implant components at least twice daily, using a soft brush and the professionally recommended oral topical agent. Patients should also be advised to clean their prostheses at least twice daily using a soft brush and the recommended denture cleaning agent. They should be instructed to remove restorations while sleeping, and the removed prostheses should be stored in a prescribed cleaning solution.
SUMMARY
As noted at the outset, implant-retained, tissue-supported mandibular overdentures are becoming the standard of care for edentulous patients,1 and provide an alternative to conventional complete dentures, as well as complex, fixed, implant-supported prostheses.2 The addition of simple implant retentive components can improve the stability, retention and function of complete dentures with relative ease and at reasonable cost.
KEY TAKEAWAYS
- Implant-retained, tissue-supported overdentures provide an alternative to conventional complete dentures and complex, fixed, implant-supported prostheses.2
- The implant-retained overdenture is secured by either a bar/retainer combination, or individual attachments that are fitted to each implant fixture. These act as both retentive components and stabilizing elements.
- Many treatment plans should begin by addressing the mandible first, followed by reevaluating the condition of the maxilla.15
- If the number of implants is to be kept at a minimum, the ability of the soft tissue to support part of the load of the implant-retained, tissue-supported overdenture is critical.
- Available restorative space is an important factor that must be assessed during treatment planning of implant overdentures and prior to implant placement.
REFERENCES
- Feine JS, Carlsson GE, Awad MA, et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Gerodontology. 2002;19:3–4.
- Emami E, Heydecke G, Rompré PH, de Grandmont P, Feine JS. Impact of implant support for mandibular dentures on satisfaction, oral and general health-related quality of life: a meta-analysis of randomized-controlled trials. Clin Oral Implants Res. 2009;20:533–544.
- Harris D, Höfer S, O’Boyle CA, et al. A comparison of implant-retained mandibular overdentures and conventional dentures on quality of life in edentulous patients: a randomized, prospective, within-subject controlled clinical trial. Clin Oral Implants Res. 2013;24:96–103.
- Feine JS, de Grandmont P, Boudrias P, et al. Within-subject comparisons of implant-supported mandibular prostheses: choice of prosthesis. J Dent Res. 1994;73:1105–1111.
- Thomason JM, Kelly SA, Bendkowski A, Ellis JS. Two implant-retained overdentures –– A review of the literature supporting the McGill and York consensus statements. J Dent. 2012;40:22–34.
- Ahuja S, Cagna DR. Defining available restorative space for implant overdentures. J Prosthet Dent. 2010;104:133–136.
- Sadowsky SJ. Treatment considerations for maxillary implant overdentures: a systematic review. J Prosthet Dent. 2007;97:340–348.
- Lee CK, Agar JR. Surgical and prosthetic planning for a two-implant-retained mandibular overdenture: a clinical report. J Prosthet Dent. 2006;95:102–105.
- Denissen HW, Kalk W, van Waas MA, van Os JH. Occlusion for maxillary dentures opposing osseointegrated mandibular prostheses. Int J Prosthodont. 1993;6:446–450.
- Lang BR, Razzoog ME. Lingualized integration: tooth molds and an occlusal scheme for edentulous implant patients. Implant Dent. 1992;1:204–211.
- Bouri A Jr, Bissasa N, Al-Zahrani MS, Faddoul F, Nouneh I. Width of keratinized gingiva and the health status of the supporting tissues around dental implants. Int J Oral Maxillofac Implants. 2008;23:323–326.
- Massad JJ, Ahuja S, Cagna DR. Implant overdentures: selections for attachment systems. Dent Today. 2013;32:128,130–132.
- Eckert SE, Carr AB. Implant-retained maxillary overdentures. Dent Clin North Am. 2004;48:585–601.
- Stoumpis C, Kohal RJ. To splint or not to splint oral implants in the implant-supported overdenture therapy? A systematic literature review. J Oral Rehabil. 2011;38:857–869.
- Chee W, Jivraj S. Treatment planning the edentulous mandible. Br Dent J. 2006;201:337–347.
- Bidra AS, Daubert DM, Garcia LT, et al. Clinical practice guidelines for recall and maintenance of patients with tooth-borne and implant-borne dental restorations. J Am Dent Assoc. 2016;147:67–74.
The authors have no commercial conflicts of interest to disclose.
Featured image and Figures courtesy of PLUMMER KD, IVANHOE JR, RAHN AO. TEXTBOOK OF COMPLETE DENTURES. 6TH ED. SHELTON, CONN: PEOPLE’S MEDICAL PUBLISHING HOUSE. 2009.
From Decisions in Dentistry. July 2017;3(7):28—31.
