

Strategies for Periodontal Risk Assessment and Prognosis
Early detection and proper management of periodontal disease can help patients maintain their natural dentition.
Early detection and proper management of periodontal disease can help patients maintain their natural dentition
PURCHASE COURSE
This course was published in the September 2017 issue and expires September 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
Determining a tooth’s prognosis is a critical step in patient care that is established after a diagnosis has been made, but before treatment has been planned and presented. Because periodontal disease is a multifactorial condition, establishing a periodontal prognosis involves both art and science. Further complicating matters, periodontal prognostic outcomes also depend on the individual’s risk factors and his or her compliance with biofilm control. With the goal of improved outcomes, this article will review the literature surrounding classification systems that can be used to assess periodontal prognosis.
This course was published in the September 2017 issue and expires September 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Explain the various periodontal prognosis systems, as well as risk factors affecting treatment and prognoses.
- Discuss the prevalence of peri-implant disease, and treatments that can improve a tooth’s prognosis.
- Detail the challenges in establishing an absolute prognostic value for periodontal patients.
Although dental implants represent a viable solution for many patients with periodontally compromised dentition, these are not necessarily lifelong restorations. Peri-implant mucositis and peri-implantitis are common complications following implant placement. Derks and Tomasi1 reported the prevalence of peri-implant mucositis and peri-implantitis at 19% to 65%. These are the most common pathological conditions that lead to soft- and hard-tissue loss around implants and compromise the functional and esthetic outcome of implant therapy.
Growing recognition that implants are not a panacea for either full or complete edentulism has led to renewed interest in saving teeth by using established therapies to improve the periodontal prognosis. Assuming they are supported by appropriate maintenance, the literature indicates that high survival and success rates can be achieved with compromised teeth.2–4 Early detection and proper management of periodontal conditions are critical to successful outcomes. Toward this goal, identifying the prognosis of each tooth — as well as systemic and local risk factors for disease progression — are critical during active periodontal treatment and supportive periodontal therapy (SPT).
PERIODONTAL PROGNOSIS
According to The Merriam-Webster Dictionary, “Prognosis” is defined as “the prospect of recovery as anticipated from the usual course of disease or peculiarities of the case.” In medicine, however, the term is commonly defined by the mortality rate. Although many periodontal prognosis systems have been developed, most of the prognoses are based on tooth mortality (i.e., extractions).5–8 Assigning an accurate prognosis for each tooth benefits patients and clinicians by providing information on whether proposed periodontal and restorative treatment promises the likelihood of a successful long-term outcome. That said, in this era of evidence-based dentistry, there is no gold standard for periodontal prognosis tools. Because disease progression is affected by many factors — including systemic conditions, local influences and the practitioner’s skill level — it is virtually impossible to establish an absolute prognostic value. Accordingly, Samet and Jotkowitz9 introduced the term “relative prognostic value.” The idea is to help practitioners identify teeth that appear to have a more favorable treatment outcome, as opposed to those more severely compromised by disease.
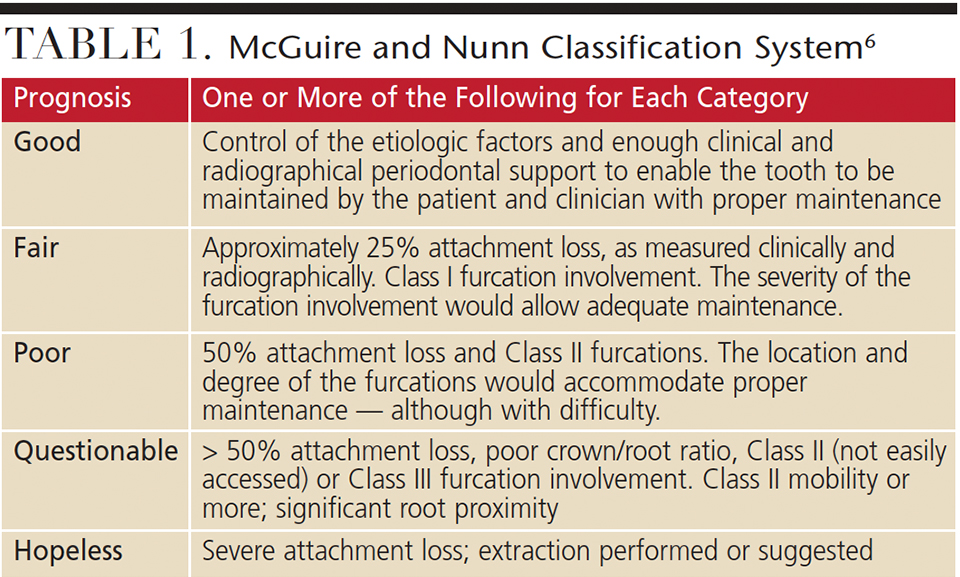
Among the various periodontal prognosis systems, the one most widely used was proposed by McGuire and Nunn in 1996.6 It consists of five categories that include good, fair, poor, questionable and hopeless (Table 1). In this system, clinicians assign each tooth to a category based on their ability to control the etiology of disease, attachment loss, presence of furcation involvement, crown/root ratio, and the degree of tooth mobility. Over five years, the researchers evaluated the accuracy of prognostic values in 100 periodontal patients. Prognostic categories were assigned following active periodontal therapy and prior to initiating the SPT phase. The study demonstrated that prognostic values are not stable over time, especially for teeth that are categorized as fair, poor or questionable; in fact, only 50% of teeth assigned into one of these three prognoses remained in the same category during subsequent assessments.

The authors identified possible clinical factors that led to the altering of the initially assigned prognosis. These included smoking, diabetes, probing depth, furcation involvement and parafunctional habits. One of the study’s limitations was that regenerative treatment — such as guided tissue regeneration and the utilization of growth factors around teeth — was not performed. In periodontal patients, it is well established that regenerative procedures on certain defects can lead to bone fill and clinical attachment level gain, and thus improve a tooth’s prognosis (Figures 1A and 1B and Figures 2A and 2B).10,11 Another limitation was the classification utilized teeth mortality, which is usually determined (and affected) by the clinician and his or her treatment philosophy.

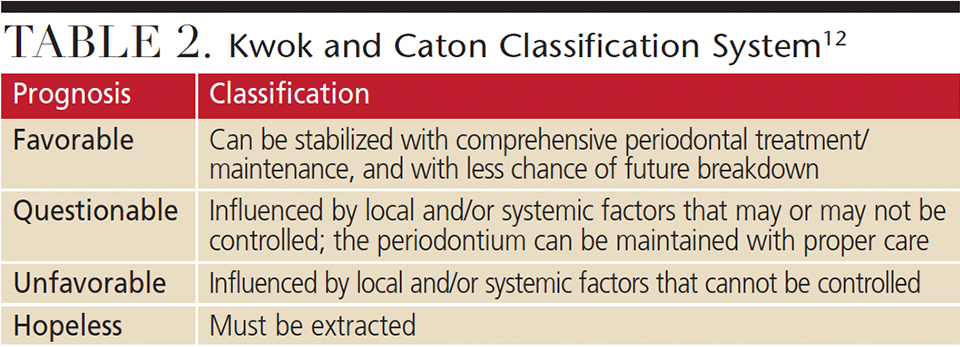
In order to account for these limitations, Kwok and Caton12 proposed a prognosis system based on future periodontal stability with treatment (Table 2). Unlike McGuire’s and Nunn’s classification, Kwok’s and Caton’s model focuses on how periodontal disease activity is suppressed by controlling systemic and local factors. These include patient compliance, smoking status and diabetic conditions as general factors, with deep probing depth, plaque retentive factors, mobility and trauma from occlusion considered as local factors. As is evident from these classifications, periodontal prognosis is dynamic because systemic and local risk factors are not permanent conditions. For example, glycemic control in a patient with diabetes might worsen during the periodontal maintenance phase, possibly contributing to progression of periodontal disease. Conversely, the prognosis of each tooth might improve if a patient quits smoking.
Periodontal conditions — such as probing depth, attachment level, bleeding on probing (BOP) and furcation involvement — are confirmed at each maintenance appointment. Thus, identifying a tooth’s prognosis only during the initial appointment does not allow adequate judgment of the probability of tooth survival, as this requires continuous monitoring of potential changes. Determining the prognosis at multiple appointments is also necessary because periodontal destruction does not occur at the same rate. Goodson et al13 evaluated disease progression in 22 subjects with untreated periodontitis for one year, with each subject receiving monthly measurements of probing depth and attachment levels. Of the subject sites, 82.8% did not show any progression in probing depths, 11.5% improved significantly and 5.7% increased in depth. Socransky et al14 cast doubt on the linear progression of periodontitis by proposing that a random burst of destructive periodontal conditions might occur at certain periods in a patient’s life. It was also emphasized that continuous monitoring of periodontal conditions longitudinally is important to maintaining natural dentition. Understanding specific progressive patterns of periodontitis with continuous monitoring, early detection and proper management of the patient’s individual risk factors are essential components of successful treatment.
RISKS FOR DISEASE PROGRESSION
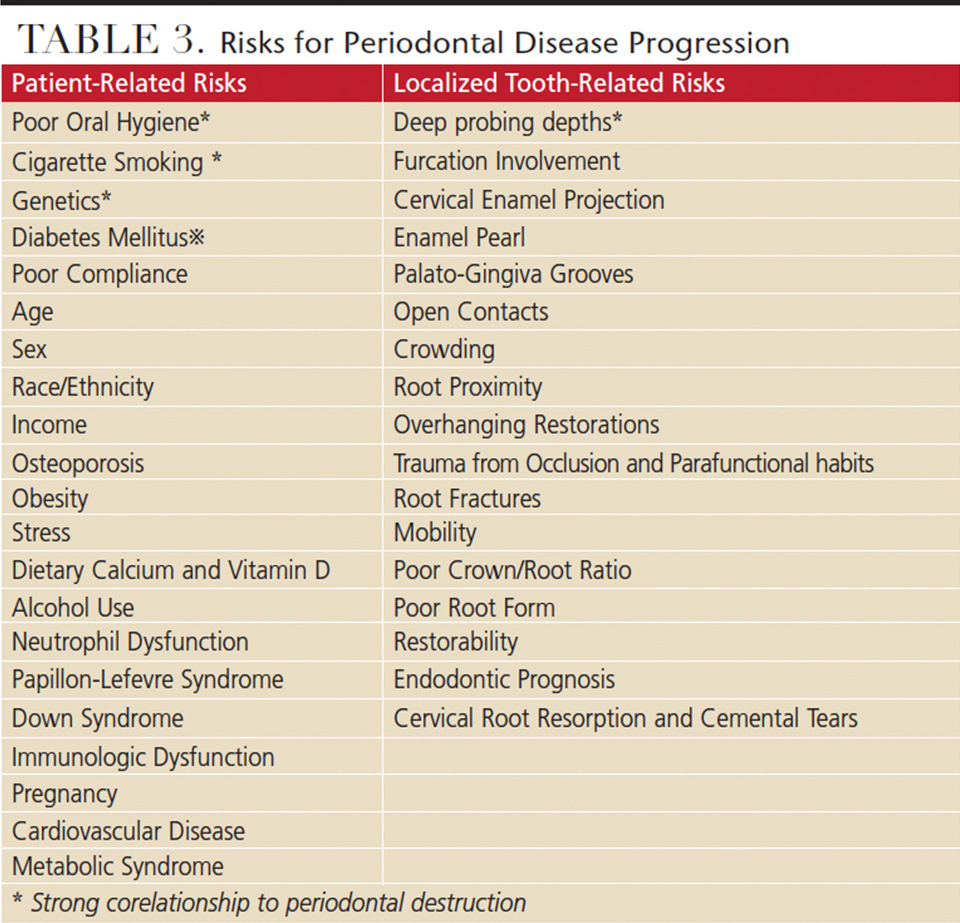
While it is accepted that the primary etiology of periodontitis is bacterial infection and a susceptible host response,15,16 the initiation and rate of destruction is affected by systemic and local risk factors. These include smoking, uncontrolled diabetes mellitus, interleukin-1 genotype, BOP, poor oral hygiene, deep probing depth (> 6 mm), severity of alveolar bone loss, age, socioeconomic status and iatrogenic factors (Table 3).
A number of studies have discussed each factor’s relationship to disease progression. However the outcomes indicate that some of these results are conflicting.17 In a day-to-day clinical setting, many clinicians simply equalize risk of disease progression with the severity of clinical attachment loss. In other words, if a patient presents with little or no periodontal destruction, it is anticipated that he or she is at low risk of future breakdown, whereas a patient with severe periodontal tissue destruction is expected to have a higher risk of future disease. The American Academy of Periodontology (AAP) defines risk assessment as, “The process by which qualitative or quantitative assessments are made of the likelihood for adverse events to occur as a result of exposure to specified health hazards or by the absence of beneficial influences.” The AAP guideline also notes that risk assessment is a necessary part of each examination, as it contributes to predicting future disease progression.18 Ultimately, assessment reduces the complexity of periodontal treatment and improves communication between general practitioners, dental hygienists and periodontists.
RISK ASSESSMENT MODELS
In 2002, Page et al19 published a periodontal risk calculator that included more than 10 risk factors, including smoking, age, diabetic condition, history of periodontal procedures, probing depth, BOP, type of restorations and bone height, among others. Using a computer-based system, risk was established on a scale of 1 (lowest) to 5 (highest). Following publication of that article, Page and Martin20 introduced the Oral Health Information Suite (OHIS), which provides a disease score on scale of 1 (health) to 100 (severe periodontal condition). More than 500 subjects were investigated (with up to 15 years of follow-up) to evaluate the relationship between the scale and actual tooth loss. The study showed that OHIS risk and disease scores provided an accurate and valid means of evaluating tooth loss and disease progression. The risk of disease and disease state score were calculated and described as objective numbers that can be used in devising interventions. This is a useful communication tool for general practitioners, dental hygienists and periodontists, especially when managing patients who are seen at multiple offices. A possible limitation is that it can be difficult to become familiar with the details of this system. Although it has been shown to be accurate, assessment tools need to be simple enough to allow efficient chairside use.
Lang and Tonetti21 introduced a Periodontal Risk Assessment (PRA) model that evaluates the risk of periodontal breakdown based on a combination of six parameters: percentage of BOP, total sites of residual pockets > 5 mm, number of teeth lost, bone loss in relation to the patient’s age, systemic/genetic condition, and environmental factors (e.g., smoking status). This tool is used to assess risk following active periodontal therapy and prior to SPT. It does not require any specific formula to calculate risk and is easy to fill out chairside. In addition, it is relatively easy to visualize the degree of risk. However, this system has several disadvantages. Because clinicians initiate PRA after active periodontal therapy, for example, this tool is not a good indicator for treatment planning or active periodontal therapy. In addition, while the six parameters have been shown to be major risk factors, patient compliance and local plaque-retentive factors are not included in the criteria.
In a retrospective study, Matuliene et al22 evaluated the validity of PRA with 160 patients for an average of 9.5 years. Based on the PRA system, all subjects were assigned to low-, moderate- or high-risk profile following active periodontal therapy. Most patients with low and moderate risk had a twice-yearly recall interval, while more than half of the high-risk patients were seen three to four times per year. During the SPT phase, 2.59 teeth per patient were lost in the high-risk group; by comparison, 1.02 teeth per patient were lost in the moderate-risk group, while the low-risk patients lost an average of 1.18 teeth. Based on this study, if a patient is categorized in the high-risk group, a standard three- or four-month recall might not prove sufficient to prevent future breakdown of periodontal tissue. Thus, recall intervals should be based on disease activity, residual risk factors and patient compliance — not on insurance coverage.
As noted, there is no gold standard in periodontal risk assessment tools because there are advantages and disadvantages to each system. The goal of using an assessment tool is to provide more predictable care and facilitate communication between dental teams and specialists. Although periodontal risk evaluation is a powerful tool for periodontal and restorative treatment, it must be appreciated that caries, endodontic failures, fractured teeth and similar conditions also affect a patient’s prognosis. Risk assessment and prognosis systems need to account for these conditions as well.
Technological advances also allow clinicians to utilize noninvasive methods — such as salivary biomarker tests — to assess periodontal conditions. Various host-related cytokines and biomarkers have been detected in the progression of periodontal disease. Studies have shown a positive relationship between salivary biomarkers and the severity of periodontitis,23,24 and, unlike a blood examination, saliva collection does not require any special training. Thus, it appears that salivary tests can be used in the diagnosis of periodontal disease and to better understand risk assessment. In addition, disease stability during maintenance can be monitored, along with the evaluation of treatment outcomes. In the future, personalized therapy that includes salivary examination seems likely to improve the quality of periodontal care.25

PRACTICE RECOMMENDATIONS
Although this article has emphasized the importance of risk analysis, specific guidelines for periodontal treatment — including the timing of referral to a specialist — are challenging due to the disease’s multifactorial nature. In a study of periodontal status, treatment, and when patients were referred to periodontists, Dockter et al26 found that among 100 newly referred patients, 74% were diagnosed with severe periodontitis and needed to have teeth extracted due to the severity of disease. This suggests that diagnosis, treatment and timely referral to a specialist were not satisfactory.
At the time of initial examination, during nonsurgical periodontal treatment and throughout SPT, clinicians need to consider the risks of disease development and possible need for referral. Although many periodontal patients can be managed appropriately by general practitioners, there is no single best treatment for every patient. Accordingly, the authors of this paper propose instructions that clinicians can use in referral decisions (Table 4). These are intended to foster a multidisciplinary approach with the goal of improved care.
In conclusion, determining a periodontal prognosis requires an evidence-based evaluation that utilizes data from a thorough clinical and radiographic examination. Risk assessment is an ongoing process that requires clinicians to be knowledgeable of the various — and dynamic — factors that influence the disease state. Together, these evaluations will help ensure appropriate periodontal treatment and optimal outcomes.
REFERENCES
- Derks J, Tomasi C. Peri‐implant health and disease. A systematic review of current epidemiology. J Clin Periodontol. 2015;42(Suppl 16):S158–S171.
- Carnevale G, Pontoriero R, di Febo G. Long‐term effects of root‐resective therapy in furcation‐involved molars. A 10-year longitudinal study. J Clin Periodontol. 1998;25:209–214.
- Fugazzotto PA. A comparison of the success of root resected molars and molar position implants in function in a private practice: results of up to 15-plus years. J Periodontol. 2001;72:1113–1123.
- Giannobile WV, Lang NP. Are dental implants a panacea or should we better strive to save teeth? J Dent Res. 2016;95:5–6.
- Becker W, Berg L, Becker BE. The long term evaluation of periodontal treatment and maintenance in 95 patients. Int J Periodontics Restorative Dent. 1984:4;54–71.
- McGuire MK, Nunn ME. Prognosis versus actual outcome. II. The effectiveness of clinical parameters in developing an accurate prognosis. J Periodontol. 1996;67:658–665.
- Hirschfeld L, Wasserman B. A long-term survey of tooth loss in 600 treated periodontal patients. J Periodontol. 1978;49:225–237.
- Miller PD Jr, McEntire ML, Marlow NM, Gellin RG. An evidenced-based scoring index to determine the periodontal prognosis on molars. J Periodontol. 2014;85:214–225.
- Samet N, Jotkowitz A. Classification and prognosis evaluation of individual teeth — a comprehensive approach. Quintessence Int. 2009;40:377–387.
- Reddy MS, Aichelmann-Reidy ME, Avila-Ortiz G, et al. Periodontal regeneration — furcation defects: a consensus report from the AAP Regeneration Workshop. J Periodontol. 2015;86(Suppl 2):S131–S133.
- Reynolds MA, Kao RT, Camargo PM, et al. Periodontal regeneration — intrabony defects: a consensus report from the AAP Regeneration Workshop. J Periodontol. 2015;86(Suppl 2):S105–S107.
- Kwok V, Caton JG. Commentary: prognosis revisited: a system for assigning periodontal prognosis. J Periodontol. 2007;78:2063–2071.
- Goodson JM, Tanner AC, Haffajee AD, Sornberger GC, Socransky SS. Patterns of progression and regression of advanced destructive periodontal disease. J Clin Periodontol. 1982;9:472–481.
- Socransky SS, Haffajee AD, Goodson JM, Lindhe J. New concepts of destructive periodontal disease. J Clin Periodontol. 1984;11:21–32.
- Page RC, Schroeder HE. Pathogenesis of inflammatory periodontal disease. A summary of current work. Lab Invest. 1976;34:235–249.
- Löe H, Anerud A, Boysen H, Morrison E. Natural history of periodontal disease in man. Rapid, moderate and no loss of attachment in Sri Lankan laborers 14 to 46 years of age. J Clin Periodontol. 1986;13:431–445.
- Kye W, Davidson R, Martin J, Engebretson S. Current status of periodontal risk assessment. J Evid Based Dent Pract. 2012;12(Suppl 3):2–11.
- American Academy of Periodontology. American Academy of Periodontology statement on risk assessment. J Periodontol. 2008;79:202.
- Page RC, Krall EA, Martin J, Mancl L, Garcia RI. Validity and accuracy of a risk calculator in predicting periodontal disease. J Am Dent Assoc. 2002;133:569–576.
- Page RC, Martin JA. Quantification of periodontal risk and disease severity and extent using the Oral Health Information Suite (OHIS). Periodontal Pract Today. 2007;4:163–180.
- Lang NP, Tonetti MS. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev Dent. 2003;1:7–16.
- Matuliene G, Studer R, Lang NP, et al. Significance of periodontal risk assessment in the recurrence of periodontitis and tooth loss. J Clinl Periodontol. 2010;37:191–199.
- Salminen A, Gursoy UK, Paju S, et al. Salivary biomarkers of bacterial burden, inflammatory response, and tissue destruction in periodontitis. J Clin Periodontol. 2014;41:442–450.
- Korte DL, Kinney J. Personalized medicine: an update of salivary biomarkers for periodontal diseases. Periodontol 2000. 2016;70:26–37.
- Giannobile WV, Salivary diagnostics for periodontal diseases. J Am Dent Assoc. 2012;143(Suppl 10):6S–11S.
- Dockter KM, Williams KB, Bray KS, Cobb CM. Relationship between prereferral periodontal care and periodontal status at time of referral. J Periodontol. 2006;77:1708–1716.
From Decisions in Dentistry. September 2017;3(9):46–50.

