
 ALEKSANDARGEORGIEV/ISTOCK/GETTY IMAGES PLUS
ALEKSANDARGEORGIEV/ISTOCK/GETTY IMAGES PLUS
Uses for Cone Beam Computed Tomography In Endodontic Care
Three-dimensional radiography is a helpful adjunct that supports accurate endodontic diagnosis, case planning and treatment.
The field of endodontics has long embraced technology in its efforts to improve the quality of care. Rotary instruments, electronic apex locators and surgical operating microscopes have expedited and improved endodontic care. They have also led to improved outcomes.1 Comparable to these advances, the advent of cone beam computed tomography (CBCT) has propelled the field to greater heights. It offers a unique technological advantage in endodontic care, as it not only greatly facilitates the diagnosis of endodontic pathology,2 it also has proven useful as a treatment aid.3
The more this three-dimensional (3D) imaging modality is utilized, the more applications are discovered. While CBCT imaging is not recommended for routine screening, several position statements on the topic demonstrate recognition by organized dentistry of its increasing utility.4 Though CBCT technology may not be available in every clinical situation, its increasing availability in both general and specialty offices assures access to this important tool by referral in most communities. Thus, in cases where CBCT will clearly aid diagnosis and/or treatment, clinicians must consider its use. Though it is clear CBCT should be employed in cases in which insufficient information is present to make a definitive diagnosis, the appearance of incidental, unexpected findings that may alter the treatment plan warrants consideration of broader application (Figures 1A and 1B). In fact, research demonstrates that many clinicians change their proposed treatment plans after reviewing CBCT findings.5 This article will review applications for CBCT in diagnosis and treatment planning, as well as in the direct delivery of endodontic care — from access through posttreatment follow-up imaging.
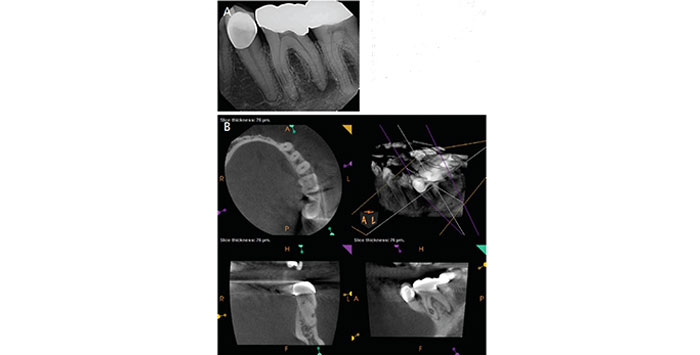
discovered while working up a tooth with pulpal necrosis and acute apical abscess (A, B).
As an imaging modality, CBCT greatly surpasses two-dimensional (2D) radiographic techniques in its ability to detect endodontic disease. The resulting images are dimensionally accurate,6 eliminating concerns over distortion with conventional 2D radiography. This dimensional accuracy facilitates precise measurement of endodontic pathology. Unlike conventional radiographs that are limited by anatomic noise, or the overlay and artifact from adjacent bone and anatomic structures that mask pathology,7 CBCT scans are not subject to anatomic noise. Consequently, these images are capable of detecting smaller areas of radiographic pathology located exclusively within cancellous bone. Conversely, traditional radiographs can only detect pathology that has escaped the confines of cancellous bone into the surrounding cortex.7 Consequently, 3D radiography eliminates the need for multiple angles of periapical imaging traditionally required to fully visualize pathosis. If one considers that radiation from limited-field-of-view CBCT is only two to three times greater than periapical imaging, the gain in information with CBCT is easily justified.
DIAGNOSIS
As a diagnostic tool, CBCT possesses particular utility in cases involving:
- Difficult-to-localize symptoms
- Areas subject to anatomic noise
- Diagnosis of previously endodontically treated teeth
- The workup of traumatic dental injuries
- Assessment of resorptive lesions
- Fracture diagnosis
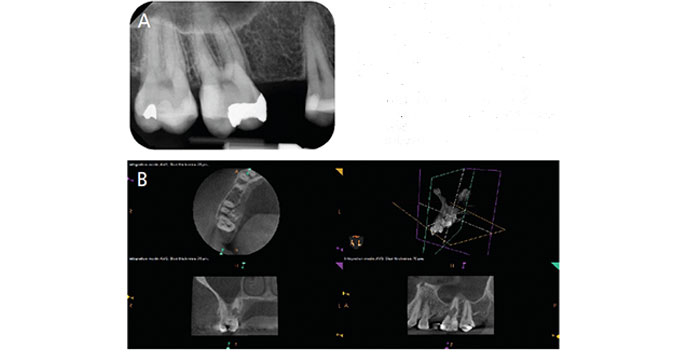
A common indication for CBCT relates to cases with a potentially difficult diagnosis due to contradictory clinical signs and symptoms, or otherwise hard to localize pain.4,8 When insufficient information is obtained from a clinical or traditional radiographic exam, a CBCT scan can be utilized to pinpoint a definitive site of endodontic pathosis (Figures 2A and 2B). In cases of pain associated with previously treated teeth, 3D imaging may better pinpoint the cause of treatment failure — namely, missed anatomy or fracture pathology. The absence of radiographic changes can suggest a non-endodontic source of pain, such as traumatic occlusion, sinus issues or even neuropathic pain. In these cases, CBCT imaging is a unique tool to confirm or refute endodontic disease as an etiology.
As CBCT images are dimensionally accurate and not limited by anatomic noise, they are two times more likely to detect periapical radiolucencies than periapical radiography alone.2 This improved sensitivity is an obvious benefit in terms of its utility as a diagnostic tool. In addition to its generally greater ability to detect apical pathology, 3D imaging is of further use in areas subject to significant anatomic noise.9 For example, due to the anatomic noise of the maxillary sinus and zygomatic process, periapical imaging of the posterior maxilla can miss about a third of lesions picked up by CBCT.6 Furthermore, early changes to the maxillary sinus — namely, development of localized maxillary sinus mucositis that can precede definitive endodontic lesions — may be easily detected with CBCT.10 Beyond identifying the exact location or source of an infection, this imaging modality can identify the extension of periapical lesions in relation to other important anatomic structures. This can play a role in the monitoring of neighboring teeth or ill effects of untreated disease. Sinus tracts, traditionally traced by gutta-percha, can be accurately assessed by localization of cortical plate breakthrough for increased diagnostic accuracy.
The use of CBCT is considered routine in the workup of traumatic dental injuries, suspected resorption or fractures, and in previously treated teeth.4 Oral trauma can involve multiple subsets of injuries, and the acute nature of such diagnoses warrants careful identification of fractured teeth and jaws, as well as displacement of teeth in bone. The American Association of Endodontists’ Guidelines for the Management of Traumatic Dental Injuries suggest that CBCT imaging, when available, should be utilized in baseline evaluations.11 These images can help identify and demonstrate the extent of both tooth and alveolar fractures, as well as guide subsequent surgical repositioning or interdisciplinary treatment planning. For luxation-type injuries, including concussion, subluxation, and lateral, intrusive and extrusive luxation injuries, 3D imaging should be utilized to visualize the periodontal ligament space and directly identify displacements. In managing avulsive injuries, CBCT imaging post-replantation can confirm positioning and rule out associated cortical plate fractures.
This advanced imaging technology is also essential in the accurate diagnosis and subsequent treatment of resorptive dental diseases. Resorptive dental diseases are multifaceted, and their management and prognosis are specific to the location, extent and type of resorption. As resorption is not often localized to just the mesial and distal aspects of teeth visible by traditional radiography, CBCT imaging is an obvious choice to fully visualize the exact location, extent and type of resorptive defect. Periapical imaging will significantly underestimate the size, circumferential spread and location of external cervical resorption.12 By comparison, CBCT imaging not only enhances the correct localization of this pathology, it also has been shown to significantly alter clinicians’ chosen treatment plans.12 Likewise, it can greatly aid in the differentiation of internal root resorption and external cervical resorption. It further allows for direct visualization of potential sources of resorption, namely, endodontic pathology that can cause apical external inflammatory root resorption, misaligned erupting teeth or non-odontogenic pathology that may cause pressure resorption.
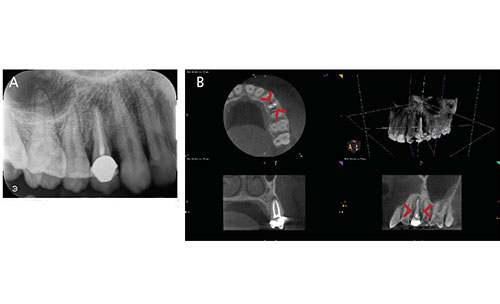
In a limited capacity, CBCT imaging can detect root fractures.13 Fracture lines can be detected only when they are of a diameter larger than the resolution of the image.13 As vertical root fractures occur with greatest frequency in previously endodontically treated teeth (oftentimes restored with metallic posts), artifacts can render fractures even harder to detect.14 That said, 3D images often show indirect findings associated with fractures, rather than the fracture lines themselves (Figures 3A and 3B). This imaging modality can detect localized areas of bone loss suggestive of root fractures, particularly areas of midroot bone loss with intact bone coronal and apical to the defect, loss of the entire buccal cortical plate, midroot radiolucencies in the area of termination of a post, and space between the buccal and lingual cortical plate and root surface.15 These areas may be seen as the classical “J-shaped” or “halo” radiolucency on traditional radiography, but considering that fractures are not confined to the mesial and distal aspects of the tooth, the use of CBCT will allow for broader identification of such lesions.
RETREATMENT CASES
Previously treated teeth with existing endodontic fillings offer another routine consideration for CBCT. Whether pathology is visible on traditional radiography or not, pain in a previously endodontically treated tooth warrants a CBCT scan. If apical pathology is not seen in an otherwise completely filled root with an adequate coronal seal, clinicians can often rule out endodontic disease as a contributing factor. If apical pathology is present, consideration should be given to the potential etiology of the failure. Initially untreated anatomy is an obvious potential reason for failure that can be improved upon with root canal retreatment by a skilled provider. Cases with evidence of an initial poor-quality root fill have the best prognosis following nonsurgical root canal retreatment.16 Prior complications — including overextension of root filling materials and separated instruments that may negatively impact retreatment — can be visualized using CBCT, which helps improve assessment of retreatment options.
When considering surgical retreatment procedures, CBCT is indispensable in the identification of adjacent anatomic considerations, including the size and extent of pathology, nuances in root anatomy, and proximity to important structures, including the maxillary sinus and mandibular nerve canal.17 Previously endodontically treated teeth may fail for reasons not entirely related to the endodontic procedure — such as developing root fractures or perforations — and CBCT imaging can be a useful adjunct for identifying these etiologies when nonsurgical or surgical endodontic retreatment is unlikely to be successful.
It is evident that CBCT imaging can have a great impact on endodontic diagnosis. It follows then that treatment planning should be positively affected by its use. Research demonstrates that when clinicians evaluate cases, first using traditional periapical radiographs, and two weeks later with CBCT imaging, their diagnosis and treatment plans change 62% of the time.5 This number increases when the provider deems the case more difficult, and is more likely to include extraction when CBCT scans are utilized.18 Given its ability to help practitioners develop better treatment plans, the justification for image exposure is clear, particularly in complex cases.
ENDODONTIC TREATMENT
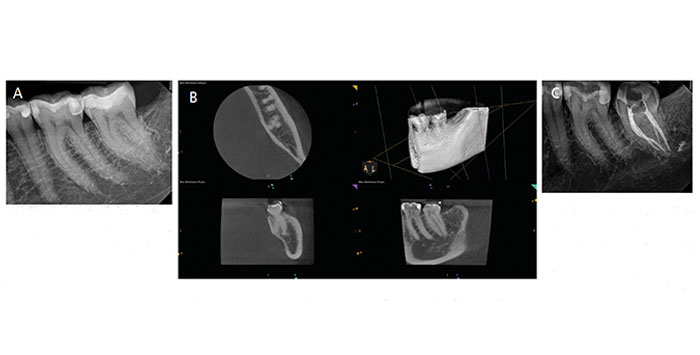
Beyond diagnosis and treatment planning, CBCT scans have great utility in enhancing the delivery of endodontic care. As the surgical operating microscope enhanced clinicians’ abilities to visualize canal anatomy, locating previously unreachable canals and managing calcification, CBCT provides a road map before an access is even made. Gone are the days of searching for that suspected second mesiobuccal canal in a maxillary molar (present 95% of the time).19 With use of a preoperative CBCT, clinicians have definitive knowledge of the location and numbers of canals in the tooth prior to treatment. The benefit of this anatomic knowledge extends beyond lessened pain and long-term failures. Prior knowledge of the nuances of treatment will result in efficiencies directly benefiting the patient in reduced treatment time, local anesthesia and patient fatigue (Figures 4A through 4C). The dimensional accuracy of CBCT scans allows for accurate working length estimation in cases in which an electronic apex locator is inaccurate.20 Future applications of CBCT may involve the creation of surgical guides, like those used in implant dentistry.3
When considering nonsurgical retreatment procedures, knowledge of the locations of previously untreated anatomy allows for considerable improvement in treatment outcomes (Figures 5A through 5D). Similarly, when planning for surgical care, preoperative CBCT imaging helps operators plan the best approach to expose the lesion, anticipate sinus involvement, and avoid anatomically challenging spaces, such as the mandibular or nasopalatine nerve canals.17
Beyond the utility of pretreatment CBCT images in care delivery, this imaging modality can be used as an intratreatment adjunct to help locate suspected anatomy. Removing the dental dam and exposing a CBCT scan can illuminate the direction of endodontic access and allow for corrections when searching for calcified canals. These images can also be used to identify intraoperative complications, such as perforations or transportations. Unique applications have been discussed in the literature, such as using CBCT to carefully map out a dens invaginatus, allowing for its conservative management.21
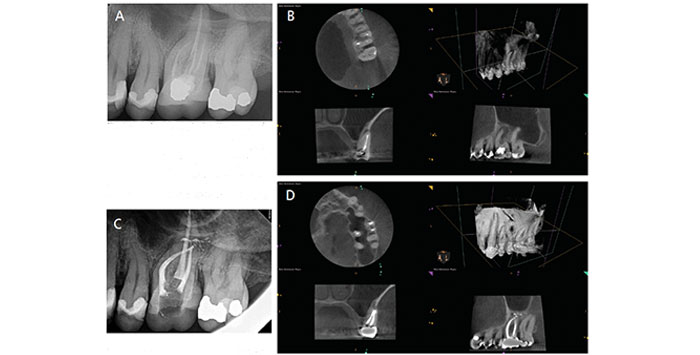
should begin with preoperative cone beam computed tomography (B). As shown here, an untreated second mesiobuccal canal was the likely source of recurrent infection, and addressing this via nonsurgical root canal retreatment resulted in apical healing (C, D).
POSTTREATMENT FOLLOW-UP
This imaging modality also allows more efficient monitoring of the healing process (Figures 5A through 5D). In cases where posterior maxillary endodontic pathology has resulted in adjacent maxillary sinus mucositis, healing of both the apical pathology and mucositis can also be monitored with CBCT imaging during postoperative evaluations.
Furthermore, when compared to periapical radiography, earlier evidence of healing will be seen with 3D imaging. When lesions extend to the lateral surfaces of other roots, monitoring for early healing can ensure that adjacent teeth remain healthy. Of course, CBCT scans — like traditional radiography — cannot help providers determine whether a lesion is pathologic or scar tissue, and new evidence suggests this more sensitive means of radiography will result in remaining apical radiolucencies in 20% of previously endodontically treated teeth.22 Thus, it is important for providers to consider how the patient is healing, as well as clinical signs and symptoms, in making any determination of success or failure.

CONCLUSION
Though its usefulness in endodontic treatment is becoming more apparent, CBCT imaging is still considered an adjunctive tool. It does not replace critical review of the patient’s history, clinical characteristics, and traditional bitewing and periapical radiographs. Extensive restorative histories involving metallic materials can create beam hardening artifacts and scatter that can greatly reduce the diagnostic yield of an image,23 and caries is still best detected through bitewing radiographs. Due to the need for thorough diagnosis, clinicians must engage in continuing education to ensure accuracy in reading CBCT images and enlist the help of a licensed oral radiologist for over-reads whenever necessary.
Ultimately, CBCT imaging is a tool to enhance the management of endodontic pathosis that should be applied when existing information is inadequate or inconclusive (Table 1). That said, its broad utility in endodontic diagnosis, treatment and follow-up should not be underestimated.
KEY TAKEAWAYS
- Cone beam computed tomography (CBCT) offers a unique technological advantage in endodontic care.
- This imaging modality not only greatly facilitates the diagnosis of endodontic pathology,2 it also has proven useful as a treatment aid.
- While CBCT is not recommended for routine endodontic screening, several position statements demonstrate recognition by organized dentistry of its increasing utility.4
- Three-dimensional radiography eliminates the need for multiple angles of periapical imaging traditionally required to fully visualize endodontic pathoses.
- Research demonstrates that many clinicians change their proposed treatment plans after reviewing CBCT findings.5
- This imaging modality also allows more efficient monitoring of the healing process.
- Ultimately, CBCT imaging is a tool to enhance the management of endodontic pathosis that should be applied when existing information is inadequate or inconclusive.
REFERENCES
- Khalighinejad N, Aminoshariae A, Kulild JC, Williams KA, Wang J, Mickel A. The effect of the dental operating microscope on the outcome of nonsurgical root canal treatment: a retrospective case-control study. J Endod. 2017;43:728–732.
- Aminoshariae A, Kulild JC, Syed A. Cone-beam computed tomography compared with intraoral radiographic lesions in endodontic outcome Studies: a systematic review. J Endod. 2018;44:1626–1631.
- Connert T, Zehnder MS, Weiger R, Kühl S, Krastl G. Microguided endodontics: accuracy of a miniaturized technique for apically extended access cavity preparation in anterior teeth. J Endod. 2017;43:787–790.
- AAE/AAOMR. AAE and AAOMR joint position statement: use of cone beam computed tomography in endodontics 2015 Update. J Endod. 2015;41:1393–1396.
- Ee J, Fayad MI, Johnson BR. Comparison of endodontic diagnosis and treatment planning decisions using cone-beam volumetric tomography versus periapical radiography. J Endod. 2014;40:910–916.
- Low KM, Dula K, Bürgin W, von Arx T. Comparison of periapical radiography and limited cone-beam tomography in posterior maxillary teeth referred for apical surgery. J Endod. 2008;34:557–562.
- Patel S, Dawood A, Mannocci F, Wilson R, Pitt Ford T. Detection of periapical bone defects in human jaws using cone beam computed tomography and intraoral radiography. Int Endod J. 2009;42:507–515.
- Fayad MI. The Impact of Cone Beam CT in Endodontics: A New Era in Diagnosis and Treatment. Available at: https://www.aae.org/specialty/newsletter/the-impact-of-cone-beam-computed-tomography-in-endodontics-a-new-era-in-diagnosis-and-treatment-planning/. Accessed December 13, 2019.
- Lofthag-Hansen S, Huumonen S, Gröndahl K, Gröndahl HG. Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:114–119.
- Nascimento EH, Pontual ML, Pontual AA, Freitas DQ, Perez DE, Ramos-Perez FM. Association between odontogenic conditions and maxillary sinus disease: a study using cone-beam computed tomography. J Endod. 2016;42:1509–1515.
- American Association of Endodontists. The Recommended Guidelines of the American Association of Endodontists for the Treatment of Traumatic Dental Injuries. Available at: http://www.nxtbook.com/nxtbooks/aae/traumaguidelines/index.php. Accessed December 13, 2019.
- Patel K, Mannocci F, Patel S. The assessment and management of external cervical resorption with periapical radiographs and cone-beam computed tomography: a clinical study. J Endod. 2016;42:1435–1440.
- Brady E, Mannocci F, Brown J, Wilson R, Patel S. A comparison of cone beam computed tomography and periapical radiography for the detection of vertical root fractures in nonendodontically treated teeth. Int Endod J. 2014;47:735–746.
- Costa FF, Gaia BF, Umetsubo OS, Cavalcanti MG. Detection of horizontal root fracture with small-volume cone-beam computed tomography in the presence and absence of intracanal metallic post. J Endod. 2011;37:1456–1459.
- Fayad MI, Ashkenaz PJ, Johnson BR. Different representations of vertical root fractures detected by cone-beam volumetric tomography: a case series report. J Endod. 2012;38:1435–1442.
- de Chevigny C, Dao TT, Basrani BR, et al. Treatment outcome in endodontics: the Toronto study-phases 3 and 4: orthograde retreatment. J Endod. 2008;34:131–137.
- von Arx T, Hanni A, Sendi P, Buser D, Bornstein MM. Radiographic study of the mandibular retromolar canal: an anatomic structure with clinical importance. J Endod. 2011;37:1630–1635.
- Rodriguez G, Abella F, Durán-Sindreu F, Patel S, Roig M. Influence of cone-beam computed tomography in clinical decision making among specialists. J Endod. 2017;43:194–199.
- Kulild JC, Peters DD. Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molars. J Endod. 1990;16:311–317.
- Jeger FB, Janner SF, Bornstein MM, Lussi A. Endodontic working length measurement with preexisting cone-beam computed tomography scanning: a prospective, controlled clinical study. J Endod. 2012;38:884–848.
- Patel S. The use of cone beam computed tomography in the conservative management of dens invaginatus: a case report. Int Endod J. 2010;43:707–713.
- Torabinejad M, Rice DD, Maktabi O, Oyoyo U, Abramovitch K. Prevalence and size of periapical radiolucencies using cone-beam computed tomography in teeth without apparent intraoral radiographic lesions: a new periapical index with a clinical recommendation. J Endod. 2018;44:389–394.
- Scarfe WC, Levin MD, Gane D, Farman AG. Use of cone beam computed tomography in endodontics. Int J Dent. 2009;2009:634567.
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. January 2020;6(1):10,12–14,17.
