

Update on Sugar Alcohols and Their Role in Caries Prevention
Here’s what the evidence says about the potential oral health benefits of commonly used sugar alcohols.
Here’s what the evidence says about the potential oral health benefits of commonly used sugar alcohols
This course was published in the July 2016 issue and expires 07/31/19. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Provide the definition of a sugar alcohol.
- Identify the different types of sugar alcohols.
- Discuss the research behind the use of sugar alcohols in caries prevention.
Although largely preventable, dental caries remains the most common chronic disease in children.1 Caries prevention is challenging due to the disease’s multifactorial etiology and risk factors. The three primary factors attributed to the etiology of dental caries are the host (teeth), cariogenic microflora and diet.2,3 Specific to diet, early milestone research, such as the Vipeholm study,4 Hopewood House study5 and Turku sugar studies,6 found a direct association between the consumption of dietary sugars and dental caries. Since then, voluminous research has been published on the role of dietary sugars in caries development.7 Without the presence of sugars, the chain of causation is incomplete and decay does not occur, demonstrating that dental caries is a diet-mediated disease.7
Upon ingestion of fermentable sugars such as sucrose, glucose and fructose, acidogenic bacteria produce acid that can lower the pH of dental biofilm to levels that cause demineralization.8 Among the various dietary sugars, sucrose is thought to be the most cariogenic. Sucrose is readily fermented by cariogenic bacteria and serves as a substrate for synthesis of extracellular and intracellular polysaccharides that play roles in bacterial adhesion to enamel.9 The extracellular polysaccharides also may increase the porosity of the biofilm, thereby facilitating the diffusion of sugars to the microbiota in the deepest parts of the biofilm.10 High-sucrose biofilms also have notably lower concentrations of calcium, phosphate and fluoride, thus limiting tooth remineralization.11
There has been ongoing interest in the use of sugar alcohols to replace traditional sugars in light of potential health benefits, such as reduced cariogenicity and fewer calories, as well as decreased glycemia and insulinaemia.12 This is because sugar alcohols are hydrogenated carbohydrates that are not readily metabolized by bacteria, making them less cariogenic when used as alternatives to dietary sugars, especially sucrose.13 The defining characteristic of sugar alcohols is the presence of an alcohol group in place of carbonyl group in the aldose and ketose moieties of mono-, di-, oligo- and polysaccharides.12 They also are referred to as polyol/polyhydric alcohol (compounds containing three or more hydroxyl groups). Polyols can be acyclic compounds, such xylitol, erythritol and sorbitol, or cyclic polyols, such as myo-inositol.14
As noted, noncariogenicity is common to all sugar alcohols because they are scarcely metabolized by microorganisms in the dental plaque.15 Thus, sugar alcohols can be classified as hypo- or nonacidogenic, with reduced or virtually no extracellular polysaccharide production.16 The fact that sugar alcohols do not produce extracellular polysaccharides is believed to be one of the reasons for their proven noncariogenicity. Another beneficial effect of sugar alcohol-based chewing gum is that chewing stimulates salivary secretion.17 Saliva can reduce caries due to its mechanical cleansing/flushing action, its ability to deliver ions for remineralization and buffer plaque acids, and its own antibacterial properties.18
In 2010, Makinen14 suggested that the efficacy of sugar alcohols for caries prevention can be determined by each molecule’s number of hydroxyl groups, with erythritol ≥ xylitol > sorbitol. Yet the effect on caries rates between erythritol and xylitol is not fully established.14 In 1989, Grenby and Mistry19 reported that the amount of polysaccharide matrices synthesized by incubated microorganisms varied between sugar alcohols, with sorbitol > mannitol > lactitol > xylitol.
Because sugar alcohols are poorly metabolized, they are only partially digested. As such, they may contribute to more frequent bowel movements, increased flatulence and diarrhea. Tolerance to sugar alcohols may vary from person to person, but most adapt to polyols within a few days.20
Based on the evidence indicating that replacing sugars with sugar alcohols reduces the risk of dental caries, the U.S. Food and Drug Administration (FDA) approved a “do not promote dental caries” claim for various sugar alcohols such as xylitol, sorbitol, erythritol, mannitol, maltitol, hydrogenated starch hydrolysate (HSH), and lactilol.21 The FDA recently added isomalt to this list.22 The purpose of this paper is to provide an evidence-based update on the commonly used sugar alcohols and their role in caries prevention.
XYLITOL
The sugar alcohol Xylitol (C5H12O5) is a five-carbon sugar. It naturally occurs in many fruits and vegetables, and is produced commercially from plants, such as birch and other hardwood trees.23 Xylitol is the most studied sugar alcohol and thought to be most effective in reducing caries. There are conflicting results from research, however, regarding the role of xylitol in caries prevention.
Twetman24 reported that xylitol reduced dental caries when given in doses of at least 5 g three to four times per day. The paper suggested that xylitol is nonfermentable, reduces the volume of dental plaque, prevents decreases in plaque pH, exerts a stimulating effect on saliva, and promotes selection of less virulent, xylitol-resistant mutans streptococci (MS).24
A systematic review was conducted in 2008 on the use of xylitol as part of an oral hygiene regimen to prevent caries. This review included two randomized clinical trials and four controlled clinical trials that compared xylitol chewing gum with no chewing gum. In their conclusions, the authors noted that research gaps existed around the dose-response relationship, and relative efficacy of different sugar alcohols.25 Another systematic review by Antonio et al26 concluded that xylitol-based candies and lozenges may help reduce the risk of noninterproximal caries, but the level of evidence was noted as inconsistent and of limited quality.
Major health organizations have expressed limited recommendations regarding the use of xylitol for preventing caries. A systematic review sponsored by the American Dental Association Council on Scientific Affairs recommended that xylitol chewing gum marginally reduces the incidence of caries.27 The 2014 U.S. Preventive Services Task Force reported insufficient evidence to formally recommend xylitol’s routine use for caries prevention.28 A Cochrane review found low-quality evidence to support the use of fluoride toothpaste containing xylitol over fluoride-only toothpaste for preventing dental caries in children’s permanent teeth, as well as insufficient evidence to support the role of other xylitol interventions in caries prevention.18 In addition, the American Academy of Pediatric Dentistry (AAPD) revised their policy on xylitol use in 2015, stating that the results from trials of xylitol aimed at reducing dental caries, transmission of MS from mothers to children, and reduction of MS levels in children varied and were inconclusive. The AAPD policy emphasized that most studies used very large doses and frequencies, which may be unrealistic in clinical practice.29
In summary, the three possible ways in which xylitol may reduce caries are by substitution of cariogenic free sugars, saliva stimulation, and a possible antibacterial effect. The literature suggests that xylitol may be effective against Streptococcus mutans when given above the daily dose threshold of 5 g to 6 g per day in three or more divided doses. It is difficult to conclude, however, if this anticaries effect is over and above sugar substitution and salivary stimulation.18 Therefore, there is low-quality evidence that supports the inclusion of xylitol in a caries prevention regimen.
SORBITOL
The sugar alcohol sorbitol (C6H14O6) is a bulk sweetener naturally found in some fruits and manufactured commercially from dextrose produced from cornstarch.23,30 Though the mechanism of anticariogenic action is the same for sorbitol as for other sugar alcohols, Ikeda31 reported that MS can metabolize sorbitol and produce acid. The amount of acid, however, was far smaller than that produced from sucrose.
Van Loveren16 concluded that most clinical trials with sorbitol-sweetened gum have a caries preventive effect in comparison with no gum use. Due to the limited number of studies included in this review, the caries preventive effect was difficult to quantify.16 Deshpande and Jadad25 concluded from a systematic review that sorbitol (alone) chewing gum reduced dental caries, but there is a research gap regarding the dose-response relationship. Conflicting evidence regarding the efficacy of sorbitol was reported by Splieth et al,32 who found that the consumption of five xylitol lozenges per day for four weeks reduced acidogenicity of plaque. Such effects were not seen with sorbitol.
Makinen33 reported that plaque can become adapted to sorbitol and its efficacy may be weaker than xylitol. Mickenautsch and Yengopal34 concluded from a systematic review that the evidence to support the use of xylitol over sorbitol is contradictory, with studies having high risk for bias and other confounders. They called for more high-quality, randomized clinical trials to provide conclusive evidence regarding the efficacy of sorbitol.
ERYTHRITOL
Erythritol (C4H10O4) is a natural tetritol sugar alcohol with four hydroxyl groups. It is a zero calorie sweetener and the newest sugar alcohol to be manufactured from cornstarch via a fermentation process. It occurs naturally in fruits, mushrooms and fermentation-derived foods, such as wine and cheese. Erythritol is rapidly absorbed in the small intestine, reducing the likelihood of laxative effects and increased flatulence.23,30
In 2013, Runnel et al35 studied the effects of three years of erythritol candy consumption in schoolchildren. They found lower levels of acetic acid and propionic acid in dental plaque, as well as a reduction in oral counts of MS when compared with the xylitol and sorbitol groups.35 Honakala et al36 conducted a randomized clinical trial on schoolchildren that compared caries variables in long-term users of erythritol or xylitol candy, as compared with a control (sorbitol candy) on dental caries. The children consumed four erythritol, sorbitol or xylitol candies three to four times a day in school for three years. Daily intake of these polyols was about 7.5 g, and caries data were collected at 12 months, 24 months and 36 months using the International Caries Detection and Assessment System. The fewest lesions and the longest time to develop caries were found in the erythritol group.36 In summary, erythritol is thought to be comparable to xylitol in caries prevention — however, more research is needed to support this claim.
MANNITOL
Mannitol (C6H14O6) is a sugar alcohol similar to sorbitol. It is found in fruits, leaves and other parts of plants and mushrooms. For commercial purposes, it is manufactured from fructose, which is derived from cornstarch. Deshpande and Jadad25 published a systematic review that reported that a combination of sorbitol and mannitol did not affect dental caries with statistical significance. In summary, there is inadequate evidence to support the use of mannitol alone for caries prevention.
MALTITOL
Maltitol (C12H24O11) is a sugar alcohol that is a reduced calorie bulk sweetener manufactured by hydrogenating maltose, which is derived from cornstarch.23,30 Birkhed et al37 evaluated the effect of maltitol lozenges over three months and observed no statistical significant difference in relative numbers of facultative anaerobic bacteria. Edgar and Dodds17 reported that maltitol affects plaque by increasing salivary flow. Holgerson et al38 conducted a randomized clinical trial among schoolchildren and reported that xylitol or sorbitol/maltitol reduced the amount of acid production in saliva and dental plaque, but only xylitol interfered with microbial composition.
In another randomized clinical trial, Lenkkeri et al39 studied caries preventive effects of xylitol/maltitol and erythritol/maltitol lozenges in children. These interventions did not provide additional preventive benefits when compared with comprehensive prevention. Thabuis et al40 conducted a randomized clinical trial on maltitol and xylitol chewing gum. The maltitol group showed higher plaque pH and reduction in cariogenic bacteria in the four-week evaluation. They concluded that sugar-free chewing gum with either maltitol or xylitol could reduce plaque acidogenicity by decreasing the level of oral bacteria.40 In summary, there is some evidence to support that maltitol affects bacterial acidogenicity, but evidence is lacking on whether it prevents caries.
ISOMALT
Isomalt (C12H24O11), a sugar alcohol of hexopyranosyl-hexitol type, is similar to maltitol. It is derived from sucrose with the original glucose-fructose bond remaining intact. The glucose portion is unchanged, but the fructose portion is converted into equal amounts of sorbitol and mannitol. As such, isomalt is a mixture of two disaccharide alcohols: gluco-mannitol and gluco-sorbitol.23,30
Out of the four papers identified that explored isomalt for caries prevention, only one was found to be somewhat relevant, with the effect of isomalt on de- and remineralization of bovine enamel lesions in vitro and in situ.41 The authors reported that isomalt facilitated tooth remineralization. In summary, there is inadequate evidence to support the use of isomalt for caries prevention.
HYDROGENATED STARCH HYDROLYSATE
Hydrogenated starch hydrolysate (HSH) is a bulk sweetener produced by partial hydrolysis of corn, wheat or potato starch, with subsequent hydrogenation of various starch fragments. This group includes hydrogenated glucose syrups, maltitol syrups and sorbitol syrups.23,30 There is little evidence to support the efficacy of HSH in caries prevention. In 1979, Birkhed et al37 evaluated the effect of HSH lozenges over three months and observed no statistical significant difference in relative numbers of facultative anaerobes. Thus, there is inadequate evidence to support the use of HSH for caries prevention.
CONCLUSION
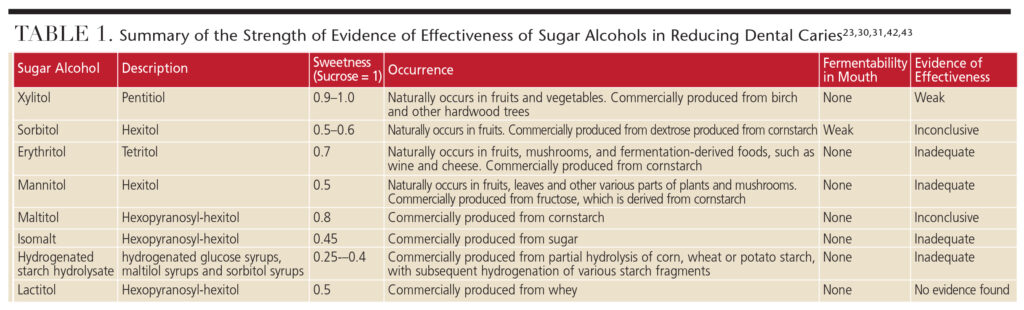
The use of sugar alcohols, especially xylitol, remains popular. This has resulted in numerous products containing xylitol, such as candies, lozenges, syrups, chewing gum, toothpaste and wipes being marketed for caries prevention. It seems prudent that dental teams be well-versed in the evidence supporting/refuting the use of such products. Some basic information found in the literature23,30,31,42,43 on sugar alcohols has been summarized in Table 1.
If sugar alcohols are used to replace sugars in between-meal snacks, a reduction in caries may occur. There is inconclusive evidence, however, to support the therapeutic effect of commercially available products containing sugar alcohols in various forms and dosages.29
Based on the literature, here are pertinent observations regarding sugar alcohols. They do not promote dental caries, and are considered passively noncariogenic. The beneficial effects of sugar alcohols may be attributed to the fact they are nonfermentable and/or promote salivary production, yet their abilities as cariostatic agents are not fully established. Currently, xylitol is the most promising sugar alcohol for caries prevention, but effective doses appear high and remain somewhat unclear. Furthermore, the high dosages used in most studies may be impractical for everyday use. Considering the inadequate evidence of efficacy and possible gastric side effects, it may be premature to support the routine use of any sugar alcohols in a caries prevention regimen.
References
- National Institute of Dental and Craniofacial Research. Oral Health in America: A Report of the Surgeon General. Available at: nidcr.nih.gov/DataStatistics/SurgeonGeneral/sgr/welcome.htm. Accessed May 3, 2016.
- Keyes PH. Infectious and Transmissable Nature of Experimental Dental Caries. Arch Oral Biol. 1960;1:304–320.
- Bowden GH. The microbial ecology of dental caries. Microbial Ecology in Health and Disease. 2000;12:138–148.
- Gustafsson BE, Quensel CE, Lanke LS, et al. The Vipeholm dental caries study; the effect of different levels of carbohydrate intake on caries activity in 436 individuals observed for five years. Acta Odontol Scand. 1954;11:232–264.
- Harris R. Biology of the children of Hopewood House, Bowral, Australia. 4. Observations on dentalcaries experience extending over five years (1957–61). J Dent Res. 1963:1387–1399.
- Scheinin A, Mäkinen KK, Ylitalo K. Turku sugar studies. V. Final report on the effect of sucrose, fructose and xylitol diets on the caries incidence in man. Acta Odontol Scand. 1976;34:179–216.
- Sheilham A, James WPT. Diet and dental caries: the pivotal role of free sugars reemphasized. J Dent Res. 2015;94:1341–1347.
- Stephan RM. Intra-oral hydrogen ion concentration associated with dental caries activity. J Dent Res. 1944;23:257–265.
- Tinanoff N, Tanzer JM, Freedman ML. In vitro colonization of Streptococcus mutans on enamel. Infection and Immunity. 1978;21(3):1010–1019.
- Rölla G. Why is sucrose so cariogenic? The role of glucosyltransferase and polysaccharides. Scand J Dent Res. 1989;97:115–119.
- Paes Leme AF, Koo H, Bellato CM, Bedi G, Cury JA. The role of sucrose in cariogenic dental biofilm formation — new insights. J Dent Res. 2006;85:878–887.
- Livesey G. Health potential of polyols as sugar replacers, with emphasis on low glycaemic properties. Nutr Res Rev. 2003;16:163–191.
- Imfeld T. Efficacy of sweeteners and sugar substitutes in caries prevention. Caries Res. 1993;27(Suppl1):50–55.
- Makinen KK. Sugar alcohols, caries incidence, and remineralization of caries lesions: A literature review. Int J Dent. 2010;2010:981072.
- Tinanoff N, Palmer CA. Dietary determinants of dental caries and dietary recommendations for preschool children. J Public Health Dent. 2000;60:197–206.
- van Loveren C. Sugar alcohols: What is the evidence for caries-preventive and caries therapeutic effects? Caries Res. 2004;38:286–293.
- Edgar WM, Dodds MW. The effect of sweeteners on acid production in plaque. Int Dent J. 1985;35:18–22.
- Riley P, Moore D, Ahmed F, Sharif M, Worthington HV. Xylitol-containing products for preventing dental caries in children and adults. Cochrane Database Syst Rev. 2015;26:CD010743.
- Grenby TH, Mistry PM. Studies of the dental properties of lactitol compared with five other bulk sweeteners in vitro. Caries Res. 1989;23:315–319.
- Calorie Control Council. Polyols and Gastro intestinal effects. Available at: polyol.org/frequently-askedquestions/ fap-g. Accessed May 3, 2016.
- Office of Federal Register, General Services Administration, Code of Federal Regulations. Title 21, Section 101, Food Labeling: Health Claims; Sugar Alcohols and Dental Caries. Available at: https://www.gpo.gov/fdsys/pkg/FR-1996-08-23/pdf/96-21481.pdf. Accessed May 3, 2016.
- Office of Federal Register, General Services Administration, Code of Federal Regulations. Title 21, Section 101, Food Labeling; Health Claims; Dietary Noncariogenic Carbohydrate Sweeteners and Dental Caries. Available at: federalregister.gov/a/E7-18196. Accessed May 3, 2016.
- Calorie Control Council. Facts About Polyols. Available at: polyol.org/facts-about-polyols. Accessed May 3, 2016.
- Twetman S. Treatment protocols: Nonfluoride management of the caries disease process and available diagnostics. Dent Clin N Am. 2010;54:527–540.
- Deshpande A, Jadad AR. The impact of polyol-containing chewing gums on dental caries. A systematic review of original randomized controlled trials and observational studies. J Am Dent Assoc. 2008;139:1602–1614.
- Antonio AG, Pierro VS, Maia LC. Caries preventive effects of xylitol-based candies and lozenges: a systematic review. J Public Health Dent. 2011;71:117–124.
- Rethman MP, Beltrán-Aguilar ED, Billings RJ, et al. Nonfluoride caries-preventive agents: Executive summary of evidence-based clinical recommendations. American Dental Association Council on Scientific Affairs Expert Panel on Nonfluoride Caries-Preventive Agents. J Am Dent Assoc. 2011;142:1065–1071.
- Moyer VA, U.S. Preventive Services Task Force. Prevention of dental caries in children from birth through age 5 years: U.S. Preventive Services Task Force recommendation statement. Pediatrics. 2014;133:1102–1111.
- American Academy of Pediatric Dentistry. Policy on the use of xylitol. Pediatr Dent. 2015/16;37:45–47.
- The Sugar Association. Sugar Alcohols. Available at: sugar.org/other-sweeteners/sugar-alcohols. Accessed May 3, 2016.
- Ikeda T. Sugar substitutes; reasons and indications for their use. Int Dent J. 1982;32:33–43.
- Splieth CH, Alkilzy M, Schmitt J, Berndt C, Welk A. Effect of xylitol and sorbitol on plaque acidogenesis. Quintessence Int. 2009;40:279–285.
- Makinen KK. Sugar alcohols sweeteners as alternatives to sugar with special consideration of xylitol. Med Pric Pract. 2011;20:303–320.
- Mickenautsch S, Yengopal V. Effect of sylitol versus sorbitol: a quantitative systematic review of clinical trials. Int Dent J. 2012;62:175–188.
- Runnel R, Makinen KK, Sisko H, Olak J, et al. Effect of three-year consumption of erythritol, xylitol and sorbitol candies on various plaque and salivary caries-related variables. J Dent. 2013;41:1236–1244.
- Honakala S, Runnel R, Saag M, et al. Effect of erythritol and xylitol on dental caries prevention in children. Caries Res. 2014;48:482–490.
- Birkhed D, Edwardsson S, Ahlden ML, Frostell G. Effects of 3 months frequent consumption of hydrogenated starch hydrolysate (Lycasin), maltitol, sorbitol and xylitol on human dental plaque. Acta Odontologica Scandinavica. 1979;37:103–115.
- Holgerson PL. Sjostrom I, Stecksen-Blicks C, Twetman S. Dental plaque formation and salivary mutans streptococci in schoolchildren after use of xylitol-containing chewing gum. Int J Paediatric Dent. 2007;17:79–85.
- Lenkkeri AM, Pienihakkinen K, Hurme S, Alanen P. The caries-preventive effect of xylitol/maltitol and erythritol/maltitol lozenges: results of a double blinded, cluster-randomized clinical trial in an area of natural fluoridation. Int J Paediatric Dent. 2012;22:180–190.
- Thabius C, Cheng CY, Wang X, et al. Effects of maltitol and xylitol chewing gums on parameters involved in dental caries development. Eur J Paediatr Dent. 2013;14:303–308.
- Takatsuka T, Exterkate RA, Ten Cate JM. Effects of isomalt on enamel de- and remineralization, a combined in vitro pH-cycling model and in situ study. Clin Oral Investig. 2008;12:173–177.
- Makinen KK, Isokangas P. Relationship between carbohydrate sweeteners and oral diseases. Progress in Food and Nutrition Science. 1988;12:73–109.
- Sugar and Sweetener guide. Available at: http://www.sugar-and-sweetener-guide.com/all-sweetenerlist. html. Accessed May 3, 2016.
From Decisions in Dentistry. July 2016;2(07):44–47.

