

Original Research: Technique Comparison: Free Gingival Graft Versus Modified Apically Repositioned Flap
This study compares the free gingival graft and modified apically repositioned flap techniques in terms of surgical wound area and quantity of anesthetic delivered in patients with bilateral mucogingival deficiencies.
This study compares the free gingival graft and modified apically repositioned flap techniques in terms of surgical wound area and quantity of anesthetic delivered in patients with bilateral mucogingival deficiencies
EDITOR’S NOTE: This practice-based research article presents an alternative treatment modality to augment the zone of attached gingiva during periodontal treatment.
Periodontal plastic surgery is frequently used to maintain the functional dentition and improve patient’s esthetics. Among various surgical techniques utilized to augment the zone of attached gingiva, the free gingival graft (FGG)1 and modified apically repositioned flap (MARF)2 techniques have shown long-term and predictable increases in the apicocoronal dimension of the soft tissues. Even though the FGG has been considered the gold standard to increase the zone of attached gingiva, alternative surgical techniques have been proposed to avoid the palatal donor graft. The wound area created on the palate has been associated with high possibility of bleeding during and after the procedure, and also with great postoperative discomfort.3

In comparing MARF to FGG,4 both techniques provide significant augmentation of the apicocoronal dimension of attached gingiva. Although the final results showed good numeric statistical outcomes in terms of probing depth, attachment level, and amount of keratinized and attached gingiva dimensions, these results did not reflect the greater picture involved in each procedure. Consideration should be given to side effects provoked by the procedure — such as morbidity and anesthetic delivered, and its implications for patient health. The information presented here provides evidence to inform clinicians and patients about treatment decisions and alternatives, and raise awareness of another technique for managing soft tissue deformities.
When developing study protocols and assessing the results of a surgical technique, McGuire et al5 suggest that assessment of postsurgical pain and discomfort, esthetic outcome, patient satisfaction, and cost effectiveness be included, as most studies do not consider self-reported outcomes as part of overall treatment assessment.5,6
The purpose of this paper is to compare the results obtained with the free gingival graft and modified apically repositioned flap techniques in terms of patient morbidity (based on the size of the wounds created) and the volume of anesthetic solution administered during surgery. The null hypothesis tested was that both surgical techniques generated similar morbidity.
CLINICAL PRESENTATION
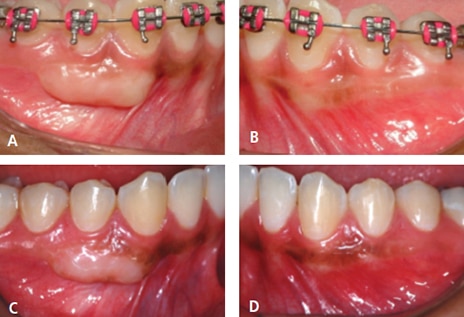
This was a split-mouth-design study comparing the increase in the apicocoronal dimension of keratinized and attached gingiva between the FGG and MARF techniques.4 Fifteen systemically healthy patients (11 women and four men) participated, and the subjects ranged from age 18 to 54 (mean 34.4 years), all were nonsmokers, and had bilateral mucogingival deformities in the mandibular arch (Figure 1). Each subject received a FGG and MARF procedure during the same appointment. The surgical technique selected for each side was determined by the toss of a coin. A total of 35 teeth were treated with the FGG1 approach and 41 teeth were treated with the MARF technique.2 The treated area consisted of a minimum of one and a maximum of four adjacent teeth (mean of 2.3 sites for FGG, and 2.7 sites for MARF).
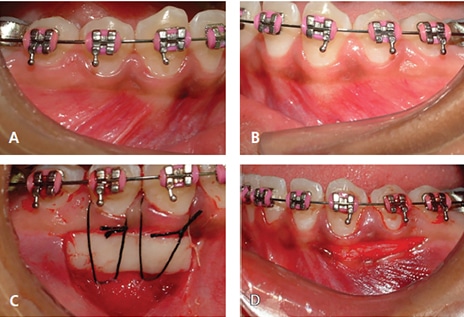
Wound Areas: To compare the surgical wound created by each technique, the areas were measured during the procedure and calculated per patient and per site (tooth) (Figures 2A through 2D). For the FGG sites, the wound areas included the recipient and donor sites. Because there is no donor site with MARF, however, the wound area involved only the treatment site. Wound area dimensions were calculated as described below.
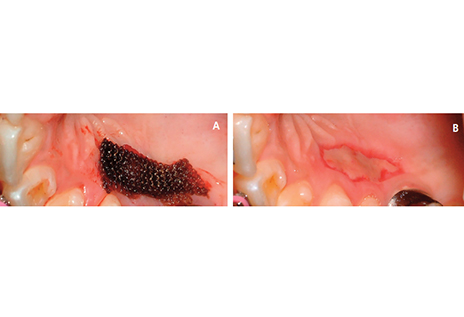
Free Gingival Graft Donor Area: After harvesting the FGG (Figures 3A and 3B), the donor site was immediately measured in millimeters with a periodontal probe with 1-mm increments and rounded to the nearest 0.5 mm. The multiplication of the height (apicocoronal) and length (mesiodistal) provided the area of the donor site. To calculate the FGG area per recipient tooth, the mesiodistal dimension of the graft was divided by the number of teeth involved in the grafting site and multiplied by the height.7
Free Gingival Graft Recipient Area: The recipient area (Figures 2A through 2D) was calculated by measuring the graft’s final dimensions, plus an additional 3 mm in apical height. The additional 3 mm dissection in the apical direction was necessary in order to attain a desirable muscle-free periosteal bed to accommodate the graft, and to facilitate the periosteal suture at a safe distance from the gingival graft’s apical border.
Modified Apically Repositioned Flap: The exposed periosteal area between the initial horizontal incision and coronal border of the apical repositioned flap was measured in height (apicocoronal) and length (mesiodistal) (Figures 2A through 2D). To calculate the area per recipient tooth, the mesiodistal dimension of the graft was divided by the number of teeth involved.
Quantity of Anesthetic Solution Utilized: Each patient was anesthetized with 2% lidocaine containing epinephrine at a concentration of 1:100,000, with each anesthetic cartridge (AC) containing 1.8 ml of anesthetic. To measure the quantity of anesthetic solution delivered, the ACs were marked with red tape in the middle. When more than half of the AC was dispensed, it was counted as full unit; and when less than half was utilized, it was considered a half cartridge. At the receptor area, the FGG was performed using the inferior alveolar nerve block for hard tissues and a buccal nerve block for soft tissues. The palatal donor area was anesthetized by a soft tissue infiltration and by a greater palatine nerve block. The mandibular nerve block injection was selected for the FGG group because it provides anesthesia for a great number of teeth and lasts longer, as the FGG surgical procedure takes more time to execute. The MARF technique was performed with only soft tissue infiltration.
Data Analysis: The data obtained for the (A) total wound area, (B) wound area per site (based on the number of sites), and (C) the number of AC utilized were averaged for the FGG and MARF groups (mean ± standard error of the mean). Statistical analysis was performed by applying Students’ t-test (GraphPad Software, La Jolla, Calif.) to the two groups. All tests were performed at 5% level of significance, and p values ≤ 0.05 were considered statistically significant.
CLINICAL OUTCOMES
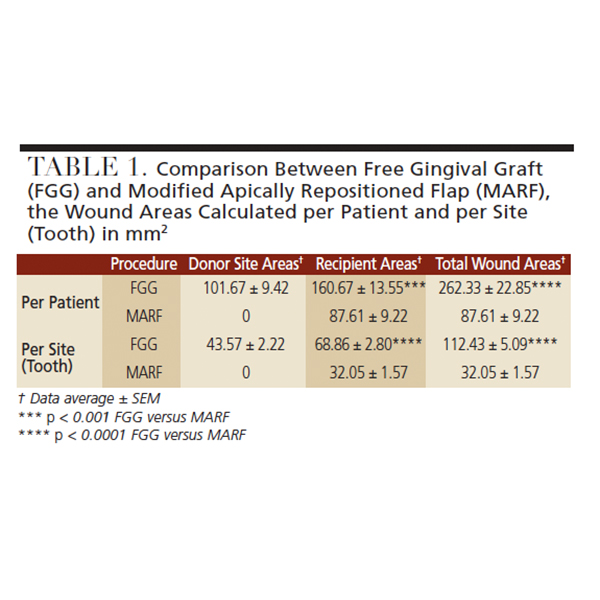
In comparing the techniques, the free gingival graft resulted in a significantly larger wound area (Figures 4A through 4D) than the modified apically repositioned flap (Table 1). The former resulted in a total wound area of 262.33 ± 22.85 mm2, which was significantly greater than the total wound area of 87.61 ± 9.22 mm2 obtained with the latter (p < 0.0001). When the wound area was prorated to the number of teeth, FGG still exhibited statistically greater morbidity than MARF (Table 1). The total wound area per tooth for FGG was 122.43 ± 5.01 mm2, compared to 32.05 ± 1.57 mm2 (p < 0.0001) for MARF.
In addition, the amount of anesthetic used was significantly greater in the execution of the FGG technique than MARF (p < 0.0001). An average of 2.90 ± 0.05 cartridges were used for FGG, and 0.87 ± 0.06 cartridges for MARF (Table 2). Table 3 presents additional information comparing FGG and MARF.
DISCUSSION
Morbidity is defined as a complication or undesirable side effect following surgery or treatment.8 As noted, the primary objective of this clinical study was to compare the wound area (morbidity) and amount of anesthetic utilized during FGG and MARF surgeries. To the best of the authors’ knowledge, this is the first report in the literature comparing the size of wound areas created by two surgical techniques.
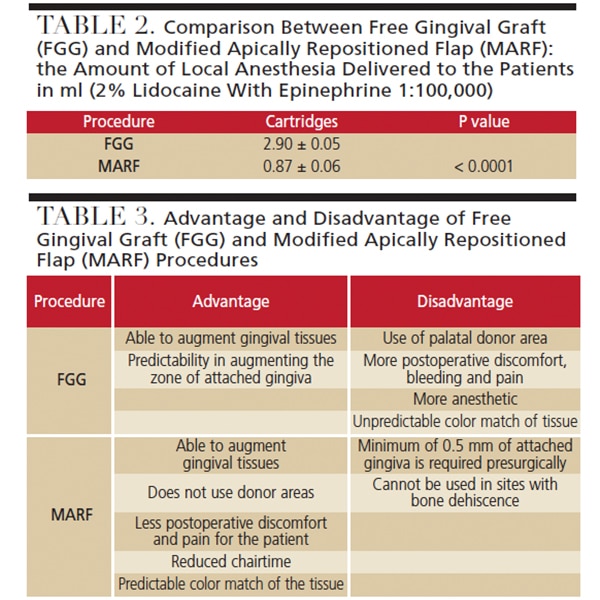
Widely used for gingival augmentation when root coverage is not intended, the main advantage of FGG is predictability in augmenting the zone of attached gingiva. Additionally, it provides the versatility of treating multiple teeth with one procedure. Disadvantages include the use of the palate as the donor area, and the generation of postoperative discomfort and pain. These drawbacks have sparked research into other surgical methods to obtain similar treatment objectives, while minimizing morbidity by improving postoperative comfort. The subepithelial connective tissue graft is another alternative with similar indications, and can also be used to increase soft tissue dimension;9 however, in this study the authors only analyzed and compared the FGG and MARF techniques.
The latter is a novel surgical technique for increasing the apicocoronal dimension of attached gingiva. Comparing the two approaches, Carnio et al4 showed that both techniques were able to increase the band of keratinized tissue and attached gingiva that exceeded 4 mm. The conclusion was that both were able to augment the gingival tissues to create dimensions that are compatible with periodontal health.4 However, despite the positive outcomes generated by the two treatment modalities in increasing the dimensions of keratinized tissue and attached gingiva, the surgical wound area created and quantity of anesthetic delivered had not previously been compared.
The average wound area created per patient with FGG was 101 mm2 and 161 mm2 at the donor and recipient areas, respectively, totaling 262 mm2 of wound area per procedure. On the other hand, MARF produced a wound area of 88 mm2; this corresponds to MARF creating 66% less wound area than the FGG approach. This difference could be explained by the use of the palatal donor site in the FGG technique, as the donor site alone produced an average of 101 mm2 of wound area. As expected, MARF produced less morbidity because it does not require palatal donor tissue. However, it is important to note that when a comparison was made between the FGG (161 mm2) and MARF (88 mm2) recipient sites, the wound created by MARF was 45% smaller than with FGG. Taking into consideration the palatal donor site is likely to result in postoperative bleeding10 and pain by virtue of creating of a wound that heals by secondary intention, it is reasonable to assume the donor site is a main cause of postoperative discomfort.11
When the size of the wound was calculated per surgical site, a similar pattern was noted, with the FGG procedure exhibiting significantly greater morbidity than MARF. Therefore, incorporating the donor and recipient site areas led to a total wound area that was 3.8 times greater in FGG compared to MARF.
As noted, another point that should be taken into consideration when planning periodontal surgeries is the amount of anesthetic with epinephrine that needs to be delivered. Most physicians have recommended special guidelines for the use of epinephrine in patients with heart conditions. Even though local anesthesia administered during periodontal surgery is considered safe and well tolerated,12 excessive amounts may produce hemodynamic responses, allergic reactions, toxicity, and increased heart rate in some patients.13 The difference in the volume of anesthetic administrated between FGG and MARF was statistically significant. The average number of ACs used for FGG was 2.9 (5.22 ml), whereas it was 0.85 (1.53 ml) for MARF, which is 70% less.
Other advantages of the MARF procedure include less chairtime, reduced postoperative discomfort, and more favorable esthetic results.4 Chairtime in the execution of periodontal procedures is relevant because surgical treatment is reported to produce higher levels of anxiety than other modalities of dental therapy. Reduced chairtime will also promote lower levels of discomfort and apprehension, and consequently reduce the level of patient anxiety.14 The duration of surgical procedures is directly correlated with postsurgical pain and/or swelling.15 There was a significant difference in the surgical time between the two procedures. The average surgical time was 48 minutes for FGG versus 20 minutes for MARF.4 Therefore, MARF led to 60% less surgical chairtime than FGG. At the end of the first postoperative week, 14 out of 15 patients reported more discomfort with the FGG procedure. At 12 months postoperatively, all 15 subjects gave esthetic preference to the results obtained with the MARF protocol. The color of the new gingival tissue created by the MARF technique was superior to that achieved with FGG; this was because the aspect of the new tissue resembled a natural gingiva.
Finally, if all of the data herein reported are combined with other data previously published and taken into consideration from a clinical standpoint, it suggests the MARF procedure is associated with less postoperative morbidity and lower quantity of local anesthesia than FGG.
SUMMARY
Both the free gingival graft and modified apically repositioned flap techniques have been shown to provide a clinically and statistically significant increase in keratinized tissue and attached gingiva. Although the MARF procedure is contraindicated when less than 0.5 mm of attached gingiva is present, clinicians can utilize this approach as a safe alternative for increasing the zone of attached gingiva, while reducing morbidity and the quantity of anesthetic delivered to patients. That noted, providers should consider the advantages and disadvantages of each technique — as well as clinical outcomes — when choosing a treatment modality for their patients.
REFERENCES
- Miller PD Jr. Root coverage using a free soft tissue autograft following citric acid application. Part 1: Technique. Int J Periodontics Restorative Dent. 1982;2:65–70.
- Carnio J, Camargo PM. The modified apically repositioned flap to increase the dimensions of attached gingiva: the single incision technique for multiple adjacent teeth. Int J Periodontics Restorative Dent. 2006;26:265–269.
- Harris RJ. Root coverage of a palatal recession defect: a case report. J Periodontol. 2001;72:1103–1107.
- Carnio J, Camargo PM, Pirih PQ. Surgical techniques to increase the apicocoronal dimension of the attached gingiva: a 1-year comparison between the free gingival graft and the modified apically repositioned flap. Int J Periodontics Restorative Dent. 2015;35:571–578.
- McGuire MK, Scheyer ET, Gwaltney C. Commentary: incorporating patient-reported outcomes in periodontal clinical trials. J Periodontol 2014;85:1313–1319.
- Scheyer ET, Sanz M, Dibart S, et al. Periodontal soft tissue non-root coverage procedures: a consensus report from the AAP Regeneration Workshop. J Periodontol. 2015;86:S73–S76.
- Orsini M, Orsini G, Benlloch D, Aranda JJ, Lázaro P, Sanz M. Esthetic and dimensional evaluation of free connective tissue grafts in prosthetically treated patients: a 1-year clinical study. J Periodontol 2004;75:470–477.
- Merriam-Webster Dictionary. Definition of morbidity. Available at: www.merriamwebster.com/dictionary/morbidity. Accessed July 31, 2017.
- Wessel JR, Tatakis DN. Patient outcomes following subepithelial connective tissue graft and free gingival graft procedures. J Periodontol. 2008;79:425–430.
- Berdon JK. Blood Loss during gingival surgery. J Periodontol. 1965;36:102–107.
- Brasher W, Rees T, Boyce WA. Complications of free grafts of masticatory mucosa. J Periodontol. 1975;46:133–138.
- Davenport RE, Porcelli RJ, Iacono VJ, Bonura CF, Mallis GI, Baer PN. Effects of anesthetics containing epinephrine on catecholamine levels during periodontal surgery. J Periodontol. 1990;61:553–558.
- Moore PA, Hersh EV. Local anesthetics: pharmacology and toxicity. Dent Clin North Am. 2010;54:587–599.
- Stabholz A, Peretz B. Dental anxiety among patients prior to different dental treatments. Int Dent J. 1999;49:90–94.
- Griffin TJ, Cheung WS, Zavras AI, Damoulis PD. Postoperative complications following gingival augmentation procedures. J Periodontol. 2006;77:2070–2079.
The authors have no commercial conflicts of interest to disclose.
Featured Image by KUMIKOMINI/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. September 2018;4(9):10–12,14.
